
Abstract
Abstract
Introduction
E
Case
A 30-year-old Indian woman presented with progressively increasing vulval swelling of 5 years' duration. She also reported losses of appetite and weight. She had no history of fever, and her menses were normal. Ten years prior to presentation, she had developed inguinal lymph-node tuberculosis with discharging inguinal sinuses, for which she received a full course of antitubercular therapy. Her tuberculosis was completely cured by the antitubercular therapy, and she did not show any evidence of a recurrence. Her genital swellings were large and caused her to have difficulty in walking. On examination, she was noted to be of an average build, with no lower-limb edema. She had two giant vulval swellings, measuring 20×15 cm on the left side and 15×10 cm on the right side (Fig. 1). The skin overlying these swellings was thick and rugose. Her lower limbs were normal. Her inguinal regions had puckered scars of healed sinuses without any palpable lymph nodes. The results of the rest of her physical examination—including her vaginal wall, chest, and abdomen—were normal. She had a normal leucocyte count. Other investigations—including blood–urea–nitrogen, serum electrolytes, creatinine, Mantoux test, night blood smear, chest X-ray, ultrasonography of her abdomen and pelvis, and pap smear—yielded normal results.

Vulval elephantiasis secondary to tubercular lymphadenitis.
This patient received surgical intervention. A wide local excision and reconstruction with a split-skin graft was performed (Fig. 2). There was considerable oozing of lymph fluid during the surgery and postoperative period.
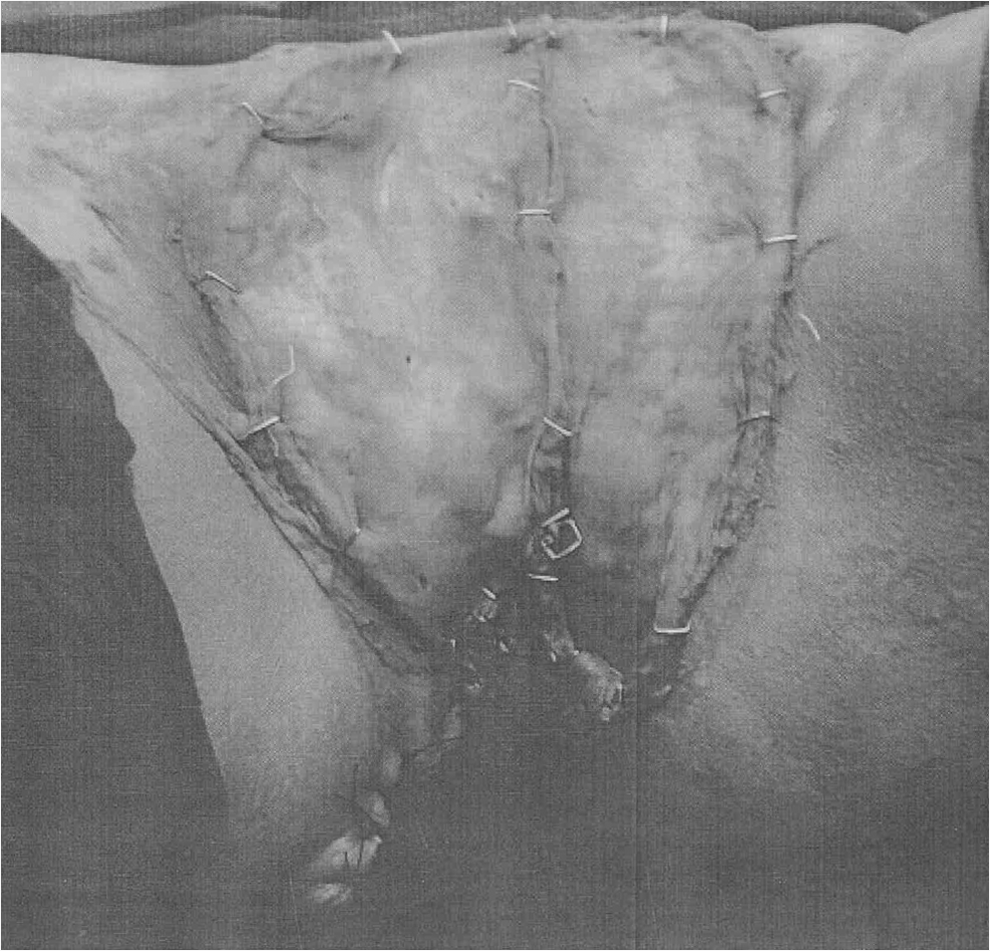
Postoperative appearance after local excision and reconstruction with a split skin graft.
Results
Other than the oozing lymph fluid, the immediate postoperative period was uneventful. A histopathologic examination of the specimen in this case showed changes that were consistent with lymphedema. The features were suggestive of nonspecific inflammation. There was, however, no clear evidence of tuberculosis in the specimens (in the form of granulomas and/or acid-fast bacilli), malignancy, filariasis, or donovanosis.
Discussion
Lymphedema occurs when the body's lymphatic system cannot accommodate the protein and fluid entering the interstitial compartment at the tissue level. In the first stage of lymphedema, impaired lymphatic drainage results in protein-rich fluid accumulation in the interstitial compartment. Clinically, this manifests as soft-pitting edema. In the second stage, there is an accumulation of fibroblasts, adipocytes, and macrophages in the affected tissues, culminating in a local inflammatory response. This results in a deposition of the connective tissue and adipose elements at the skin and subcutaneous levels, leading to nonpitting edema. In the third and most advanced stage, the affected tissues sustain further injury as a result of both the local inflammatory response and recurrent infections. Such repeated episodes injure the remaining, incompetent lymphatic channels, progressively worsening the underlying insufficiency of the lymphatic system. This eventually results in excessive subcutaneous fibrosis and scarring with associated severe skin changes characteristic of lymphostatic elephantiasis.8,9
Lymphedema is generally classified as primary when there is no known etiology, and as secondary when its cause is a known disease. 8 Primary lymphedema with an onset before age 2 is referred to as congenital; the familial version of which is known as Milroy's disease. Primary lymphedema with an onset between ages 2 and 35 is called lymphedema praecox. It is the most common form of primary lymphedema, accounting for 80% of the cases. The familial version of lymphedema praecox is known as Meige's disease. Primary lymphedema with an onset after age 35 is called lymphedema tarda. In general, primary lymphedema progresses more slowly than secondary lymphedema.8,9
The most common form of lymphedema is secondary lymphedema. In developed countries, the most common causes of secondary lymphedema involve resection or ablation of the regional lymph nodes by surgery, radiation, tumor invasion, direct trauma, or, less commonly, an infectious process. Globally, filariasis, caused by infestation of the lymph nodes by the parasite Wuchereria bancrofti, is the most common cause of secondary lymphedema.9,10
Vulval tuberculosis leading to pseudoelephantiasis—direct infiltration of the vulva by tuberculosis—is rare; however a few cases have been previously reported. 9 Vulval elephantiasis as a consequence of extensive lymph-node destruction by tuberculosis in the inguinal region is even rarer still. Sharma et al. reported 2 cases of vulval elephantiasis as a consequence of tubercular lymphadenitis; however, 1 case had smaller-size vulval swellings. 6 Chintamani et al. reported 2 cases of vulval elephantiasis as a result of tubercular lymphadenitis. 11
In the current case, the absence of a tubercular histology from the vulva ruled out direct infiltration; that is, pseudoelephantiasis. Moreover, in the current case, there was a definite past history of lymph-node tuberculosis, with evidence of the puckered scars of healed sinuses in the inguinal regions. The etiology in this current case was the extensive destruction of the inguinal lymph nodes and their channels as a result of past tuberculosis, leading to a blockage of lymphatic drainage and resulting in vulval elephantiasis.
Conclusions
Vulval elephantiasis is very rare, and vulval elephantiasis as a consequence of lymph-node destruction caused by tuberculosis, as shown in this case reports, is rarer still.
Footnotes
Acknowledgments
S.P. Singh was the chief operating surgeon. S. Katyal was the senior resident who assisted in the surgery and work-up of the patient. S.K. Singh, M. Lallar, and A. Al Huq contributed to the preparation of this article.
Disclosure Statement
No financial conflicts of interest exist.