
Abstract
Abstract
Introduction
C
Case
A 25-year-old gravida 2, para 1 previous lower-segment cesarean delivery (LSCD) was referred to the Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER) as a case of cesarean delivery scar pregnancy. She underwent medical termination of pregnancy for amenorrhea of 2 months' duration, and complained of continuous bleeding per vaginum of 25 days' duration. The bleeding was fresh and moderate in amount (soaking 5–6 pads per day), and was associated with minimal lower abdominal discomfort. Medical abortion was performed initially; then dilatation and curettage was attempted twice for persistent bleeding. The patient also received four doses of 400 μg of vaginal misoprostol, with a diagnosis of incomplete abortion, and there was no history of expulsion of products following this.
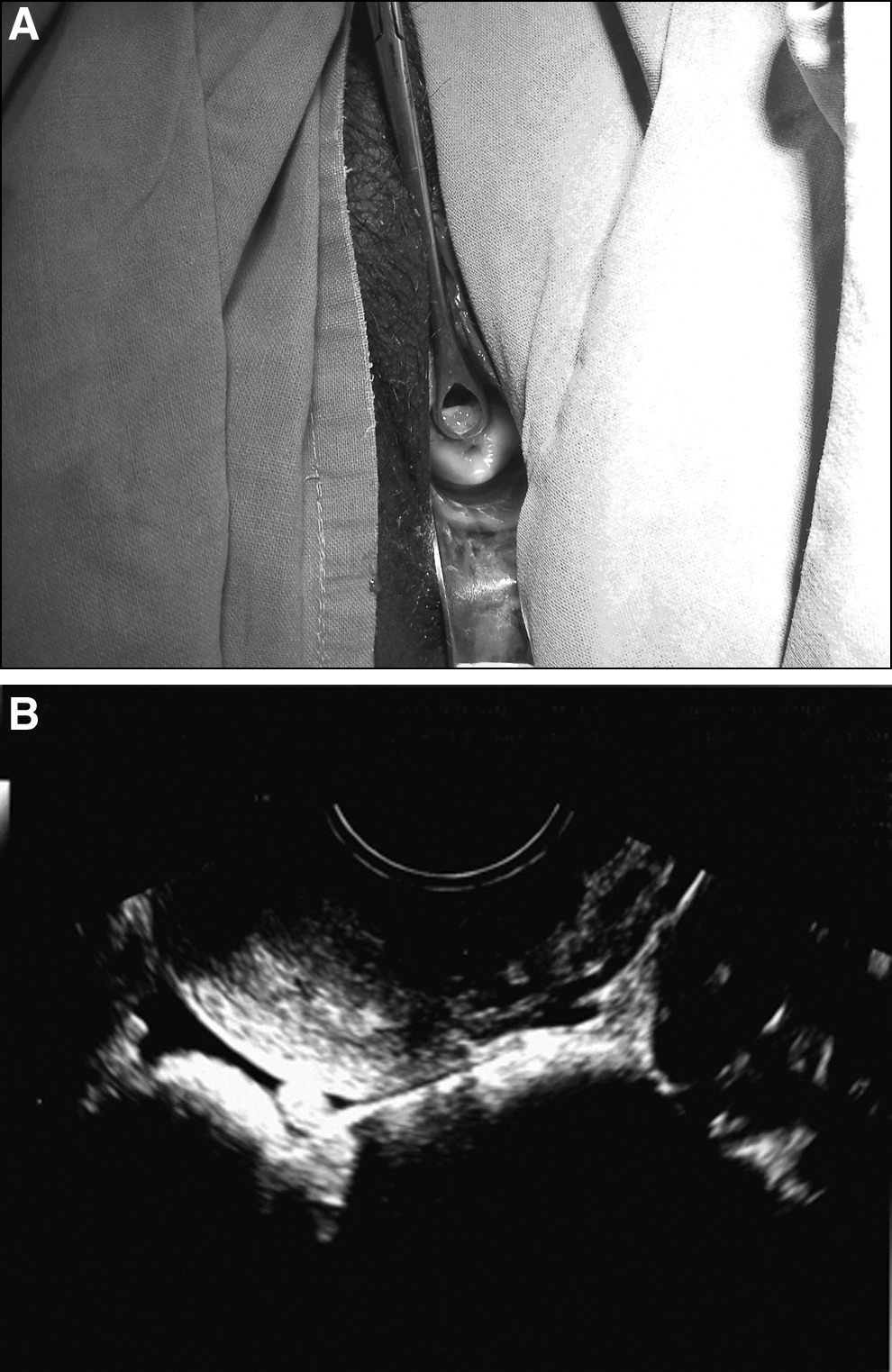
On examination, the patient had no pallor, and her vital signs were normal. Findings from systemic examination and abdominal examination were also normal. Speculum examination revealed a hypertrophied cervix with hemorrhage from the external os, which was open revealing the membranes (Fig. 1A). On vaginal examination, the cervix was felt to be enlarged and ballooned, the uterus was bulky, and the fornices were free. Transvaginal sonography revealed a gestational sac of 3.2×2.4 cm in the cervical canal below the internal os. The fetal pole was not recognized. Instead, there was an echogenic area suggesting unviable products of conception. The uterine cavity was empty (Fig. 1B). Cervical pregnancy was confirmed, and the patient was hospitalized for medical management. Her hemoglobin was 9.8 g%, and her white blood cell (WBC), T-cell, dendritic cell, and platelet counts were within normal limits. Both of her Fallopian tubes were normal. Cervical swab culture and urine culture results were sterile. The patient's serum β–human chorionic gonadotropin (β-hCG) level was 146.2 mIU/mL. She was treated with a variable dose of methotrexate (1 mg/kg body weight) on days 1, 3, 5, and 7 with an injection of folinic acid on days 2, 4, 6, and 8 (from December 11 to December 18, 2013). Bleeding from her vagina persisted but the volume of this blood was lower. Her β-hCG level was 24.4 mIU/mL on December 19, 2013 (after the last dose). The patient did not have any side-effects, and a hemogram test result was normal except that her WBC count decreased to 3500/mm3 from 12,000/mm3. She was discharged at her request, and was advised to repeat the β-hCG count at a nearby laboratory after 1 week, and to come for follow-up.

Results
After 1 week, the patient came to the outpatient department with a β-hCG level of 490 mIU/mL. The current authors considered injecting methotrexate locally into the sac. However, on speculum examination, she was found to have a surprisingly normal-looking cervix (Fig. 2A); therefore, injecting methotrexate was deferred, and a transvaginal ultrasonography (USG) was performed, which confirmed the normal cervix, with a normal endocervical canal (Fig. 2 B), revealing the complete resolution of ectopic gestation. A repeat β-hCG test at the JIPMER showed a level of <5 mIU/mL, and, on the same day, at another laboratory, was <3 mIU/mL.
Discussion
The diagnosis of cervical pregnancy is rarely made clinically, because physicians rarely consider this possibility. 3 Paalman and McElin proposed the following clinical criteria for cervical pregnancy in 1959 4 : (1) amenorrhea followed by painless uterine bleeding: (2) a softened and disproportionately enlarged cervix equal to or larger than the corpus (hourglass-shaped uterus): (3) products of conception entirely confined within and firmly attached to the endocervix; (4) closed internal os; and (5) partially open external os. However, these criteria are rarely applied in clinical practice.
The occurrence of cervical pregnancy has been attributed to various risk factors: previous uterine/cervical curettage; Asherman's syndrome; cervical endometriosis; presence of an intrauterine device; previous cesarean delivery; other uterine surgeries; and assisted reproductive techniques. In the present case, previous cesarean delivery was the probable risk factor. A large retrospective study conducted from 1985 to 2005 reported curettage as a risk factor in 50% of the cases and cesarean delivery in 17.6% of the cases. 5 The most common symptom is painless bleeding from the vagina, with some lower abdominal discomfort, as in this case. In some cases, bleeding can be severe, resulting in hemorrhagic shock and death, if not recognized promptly and treated. The clinical signs would be a hypertrophied and ballooned cervix. The confirmation of diagnosis is by ultrasound findings of the presence of a gestational sac below the internal os, rather than by histopathologic examination. 6
The life-threatening complication of cervical pregnancy is hemorrhage, which results in death, as oxytocics cannot control the bleeding, because the implantation is in the cervix, which has very few smooth muscle fibers. Failure to respond to oxytocics is also illustrated in this case, as the products were not expelled after four doses of vaginal misoprostol. Hence early diagnosis and optimum management are essential. Local and or systemic methotrexate is one of the modalities of therapy used to preserve the uterus. Transvaginal ultrasound-guided injection of methotrexate into the amnion or chorion resulted in successful management in resolution of cervical pregnancy in 49 days. Normalization of β-hCG is slow, and the mean time taken was 38 days. 7 This review showed initial high mean β-hCG levels (38,948 mIU/mL) with fetal cardiac activity.
The median time for resolution of cervical ectopic on USG was found to be 86 days, and the median time for normalization of β-hCG was 68 days when systemic methotrexate was used. The cervical pregnancy appeared as a mixed echogenic lesion with serial USG, and lagged behind the resolution of serum β-hCG. 8 In the present case, the cervical pregnancy appeared as an irregular sac with echogenic margins, and the initial β-hCG level was low, most probably because there was interference pharmacologically as well as surgically. Although the expectations of the patient's response to a single course of variable doses of methotrexate were positive, the laboratory report, which was wrong, led to a diagnosis of a persistent ectopic pregnancy, with need for further management, before clinical and sonographic reevaluation.
The other option for management of cervical ectopic pregnancy is expectant management, when there is no bleeding and β-hCG levels are <1000 mIU/mL. This approach was not used, although this patient's β-hCG levels were low, because she was bleeding. The other medical options include injection of potassium chloride into the fetal cardiac cavity, or injection of methotrexate into the gestational sac. A large review of the literature regarding the success of local injections for management of cervical pregnancies, including recurrent cervical pregnancies, has shown a success rate of 815, with a mean resolution time of 7.5 weeks. 9
Other conservative therapies include embolization of the uterine artery,10,11 transvaginal ligation of cervical branches of the uterine artery, 12 and hysteroscopic resection. 13 Hysterectomy is, rarely, needed to save a patient's life when there is intractable hemorrhage. In the series reported by Ferrara and colleagues, 1.1% of cases needed hysterectomy. 9 Uterine artery embolization is good option, and can be performed in bleeding cases, 10 and for a faster recovery, it can be safely followed by dilatation and curettage.10,11 The hospital where the case reported here was treated does not have the expertise for such a procedure.
Methotrexate may be the first-line management when the patient is stable and early in gestation, and when the β-hCG is <10,000 mIU/mL. Methotrexate cannot be used in hemodynamically unstable patients, when there is severe anemia or thrombocytopenia, when there is active tuberculosis, and in cases of hepatic dysfunction. When failure occurs with methotrexate, the case may be managed with uterine artery embolization or hysteroscopic resection. 13 Very rarely, hysterectomy is needed to save the patient's life, when conservative surgical procedures, such as uterine artery ligation, also fail to control the hemorrhage. 14
Conclusions
It is usually predicted that when β-hCG levels are low, methotrexate treatment will be successful, but one should depend on clinical and sonographic findings of response rather than β-hCG levels, which may be wrong sometimes, as in this case.
Transvaginal USG is essential/mandatory before subjecting the patient to pharmacologic termination of pregnancy (MTP). Methotrexate therapy is a better option than misoprostol for managing cervical ectopic pregnancy.
Footnotes
Disclosure Statement
No competing financial interests exist.