
Abstract
Abstract
Introduction
F
Myomectomy during cesarean section remains a controversial topic; the risk of uncontrollable hemorrhage and possible difficulty of obliterating the fibromyoma cavity are the main reasons discouraging surgeons from removing fibroids during cesarean deliveries unless the fibroids are small and pedunculated. 8 Despite this, the medical literature has reported an increasing rate of myomectomies during cesarean sections in the past decade. 9
The aim of this study was to investigate whether or not removal of myomas during cesarean section aggravates the early postoperative period.
Materials and Methods
During the years 2006–2013, the surgical outcomes of myomectomy during cesarean section were evaluated retrospectively. A total of 476 patients with documented myomas during pregnancy (detected by ultrasound or intraoperatively), who were selected for cesarean section, were enrolled. The exclusion criteria included: (1) antenatal bleeding; (2) procedures performed during cesarean section other than myomectomy; and (3) comorbid conditions with evidence of coagulopathy. Of the patients who were enrolled, 130 underwent cesarean myomectomy. Indications for cesarean myomectomy were: (1) patient's desire to have this procedure; (2) the presence of symptomatic myomas; (3) the presence of tumor previa; and (4) the presence of degenerative myomas. Informed consent, written or oral (in cases of intraoperative findings), was obtained from all of the patients.
Prophylactic antibiotics were used for all patients, with cefuroxime and metronidazole given intraoperatively. A routine intracapsular myomectomy was performed on all fibroid growths of the patients who were selected for myomectomy, through the same cesarean incision where possible, or through other incisions when necessary. In cases of myomas lying away from the low uterine segment, the myomectomy was performed always after the lower uterine segment (LUS) closure was completed. With a monopolar electroscalper at low wattage, a linear incision was made over the uterine serosa direct to the myoma until the opening of the pseudocapsule. Then, the myoma was extracted from its capsule. During the whole procedure, careful hemostasis and consequent minimal blood loss were achieved with low-wattage electrocautery. In cases of myomas in sites near the LUS, the cesarean uterine incision was not closed first. Instead, an interlocked suture was placed on the edge of the incision, and the myomectomy was performed from this site.
Postoperatively, the patients received antibiotics, fluids, electrolytes, and oxytocin for 1 day.
The patients' demographic characteristics, gestational age at delivery, number, size and location of the myomas, the duration of the operation and the days of hospital stay were recorded. Outcome measures were considered for the number and size of fibroid growths, need for blood transfusion, and other intra- and postoperative complications. Hematocrit values were obtained at the first postoperative day and were compared to the preoperative values that had been obtained.
All data were analyzed, using Fisher's exact Chi-square tests for categorical variables and Student's t-test for continuous variables. A p-value of<0.05 was considered to be statistically significant.
Results
For this study, the patients were divided into 2 groups. Group A (the myomectomy group) included women who underwent myomectomy during a cesarean section. Group B (the control group) consisted of women, who underwent “no touch” cesarean section, which meant that their myomas were not removed during the cesarean section. Group A consisted of 130 women and Group B consisted of 346 women. With the exception of myoma diameter, both myomectomy and control groups were similar in terms of characteristics (maternal age, parity, gestational week) with no statistical differences. The mean size of the myoma diameters in groups A and B was 8.5±4 cm (range: 3.5–22 cm) and 6±3.2 (range: 2.4–12 cm), respectively (Table 1).
SD, standard deviation; NS, not significant.
Most removed myomas were subserosal (41%) and intramural (14.5%), whereas pedunculated (11.2%) or submucosal (5.3%) myomas were less common. In 28% of the patients, myomas were present in more than one site (Fig. 1).

Location of removed myomas.
Differences in blood parameters and surgical outcomes between the two groups were not statistically significant. More specifically, both the incidence of hemorrhage (10.9% versus 9.3%) and the mean change in hemoglobin values (1±0.2 g/dL versus 1±0.3 g/dL) were not different in the two groups. In addition, no patient needed blood transfusion and no obstetric hysterectomy or other procedure was performed to control intraoperative bleeding. Postoperative fever was statistically nonsignificant between the myomectomy (5.6%) and control (5.9%) groups (Fig. 2; Table 2).
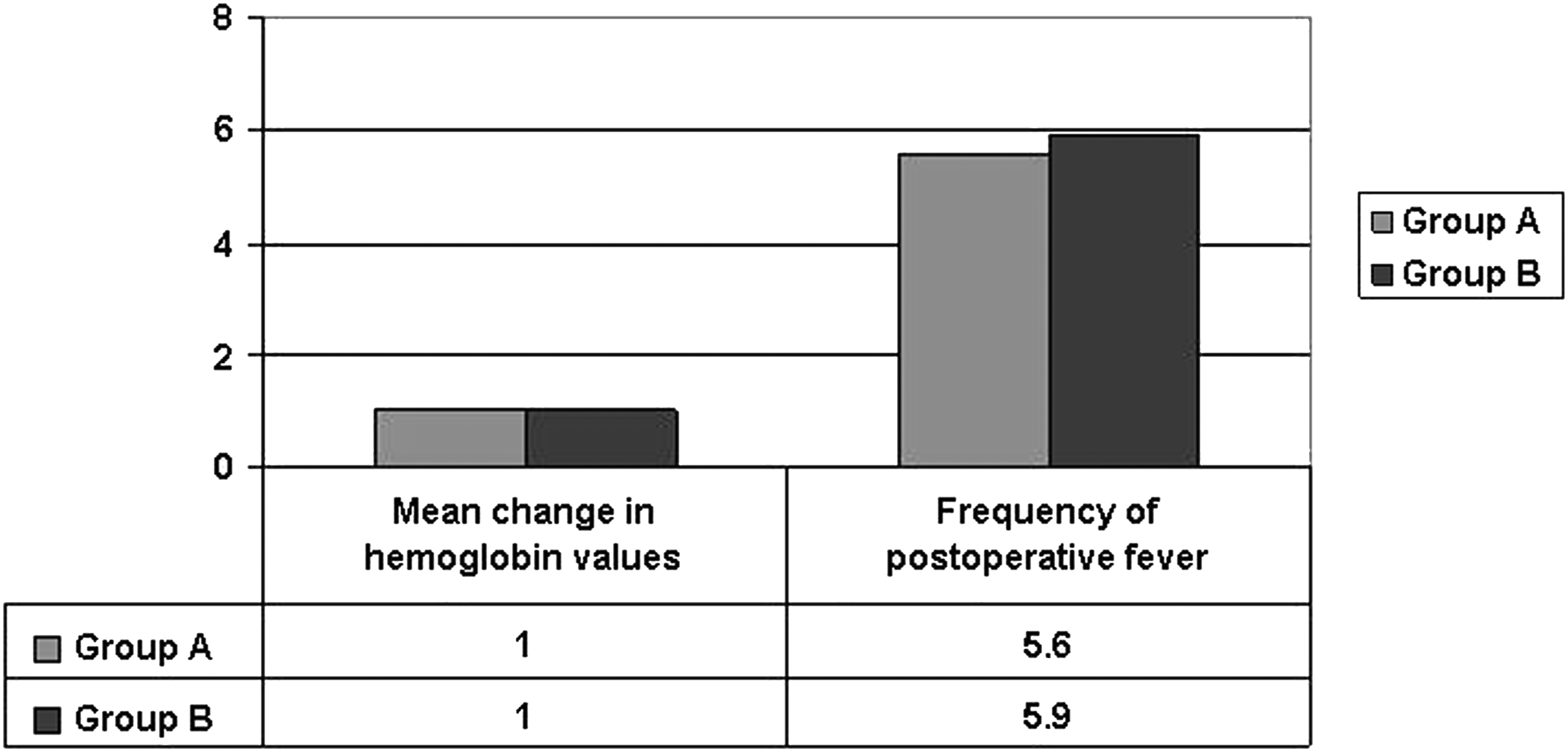
Parameters with statistically no significant differences between the two groups
NS, not significant; SD, standard deviation.
The average duration of the operation was by 13 minutes longer when myomectomy was performed. This could be characterized as a prolonged procedure, but it should also be considered that these procedures were performed by both trainees and senior staff. The mean duration of hospitalization was 3.9 days for the myomectomy group and 3.2 days for the control group, and this difference was found to be statistically significant (Fig. 3; Table 2). The longer hospital stay of patients undergoing cesarean myomectomy was the result mostly of both the surgeon's and patient's choice for to ensure that there were no complications.
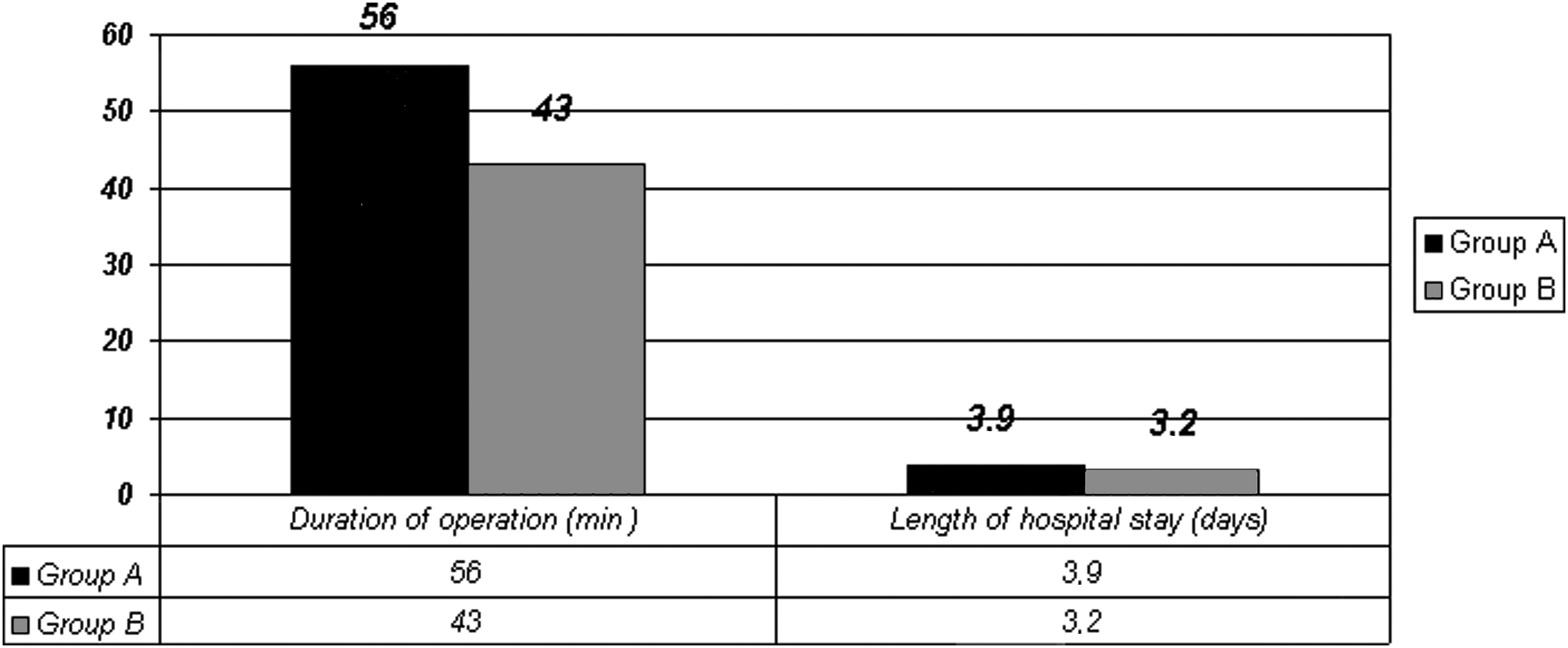
Parameters with statistically significant differences between the two groups.
The postdischarge period was uncomplicated for all the patients in the study, and no repeated surgery was required for the patients in the myomectomy group.
Discussion
The data from the current study show that the only parameters that could affect a surgeon's decision negatively to perform cesarean myomectomy are longer operation duration and longer hospital stay. However, the current study showed that there was no difference between myomectomy and control groups, in terms of preoperative hemoglobin values, mean change in hemoglobin values, incidence of intraoperative hemorrhage, frequency of blood transfusion, and postoperative fever.
Every clinician who notes fibroids during a cesarean should take into consideration the positive and negative consequences of performing a cesarean myomectomy.
Reports have indicated that, with careful case selection, cesarean myomectomy is safe and improves later pregnancy outcomes, compared with myomas that have not been surgically removed. 10 This is because uterine fibroid growths are associated with a 10%–40% obstetric complication rate and adverse obstetric outcomes. 11 Larger fibroid growths (>5 cm) can cause miscarriages, obstructed labor, malpresentations, pressure symptoms, red degeneration (i.e., necrosis, which causes the tissue to turn red), pain, preterm labor, premature rupture of the membranes, retained placentas, postpartum hemorrhage, and uterine torsion.7,12–14 The obviation of fibroid-related complications in subsequent pregnancies and of the need for interval myomectomy results in considering cesarean myomectomy as a cost-effective procedure.15,16 Technically, the incision over the uterus for myomectomy seems to be smaller during pregnancy. In addition, the myometrium is more elastic and less-fragile during pregnancy than during non-pregnancy, and, as a result, the myometrium is easier to suture during cesarean myomectomy. 17 There are reports indicating better scar integrity following cesarean myomectomy, compared with interval myomectomy, as assessed with serial ultrasound scanning in subsequent pregnancies and at subsequent cesarean sections.18,19 In addition, the uterus in the immediate postpartum phase is adapted better physiologically to control hemorrhage than at any other stage in a woman's life.
However, operations in the uterus during cesarean sections, with the exception of excisions of pedunculated myomas, are conventionally discouraged. The main reason for this is the fear of uncontrolled and perfuse bleeding and consequent severe anaemia, puerperal infection, and unwanted hysterectomy. Nevertheless, uterine tourniquet, bilateral uterine artery ligation, electrocautery, and oxytocin infusion are techniques that can be used to minimize of blood loss during cesarean myomectomy.16,20–22
Furthermore, myomas often undergo involution after delivery and may even become pedunculated. As a result, interval myomectomy (if necessary) becomes easier and safer.23,24 In addition, bizarre nuclear changes occur in myomas during pregnancy and are often confused with sarcomas, thus leading to anxiety. Removing a large myoma during a cesarean section has been considered to be a risk for uterine rupture in future pregnancy. 14 Cesarean myomectomies, like other laparotomy procedures, are associated with comparably greater risks for adhesion formation than laparoscopic procedures. 25
Nevertheless, according to the medical literature, myomectomy during cesarean has been proved to be a safer procedure than previously believed. Ortac et al. performed 22 cesarean myomectomies for large fibroid growths (>5 cm) and came to the conclusion that such a procedure minimizes postoperative sepsis. 8 Omar et al. also reported that cesaream myomectomy improves the chances of vaginal delivery in future pregnancies, especially when removed from the lower uterine segment. 26 Ehigiegba et al. reported 25 cases of cesarean myomectomies, with a total of 84 fibroid growths being removed. Although anemia was apparent in 60% of cases, only 5 of the patients needed blood transfusion, whereas no patients needed hysterectomy. Three of the patients achieved subsequent pregnancies, 2 of whom had vaginal deliveries. 27
Roman and Tabsh studied a large number of patients with myomas undergoing either cesarean section or cesarean myomectomy. Removal of the myomas was dictated by the presence of symptoms (such as pain), dystocia, and/or the unusual appearance of myomas. The researchers concluded that there was no significant difference between the two groups in that study with respect to postoperative complications, operating times, and postpartum hospital stays. 28 Kaymak et al. reached similar conclusions, and proposed removal of myomas during cesarean section by experienced obstetricians. 29
Another study by Adesiyun et al. 21 indicated that the spectrum and prevalence of encountered complications associated directly with cesarean myomectomy were not different from those reported for cesarean section alone. In addition, a rate of 76.5% was recorded for vaginal births after cesarean myomectomy, which was comparable with the range of vaginal birth after cesarean section. It was also reported that cesarean myomectomies would not affect future fertility and/or subsequent pregnancy outcomes significantly. 21
Li et al. found no significant complications during puerperium among Chinese women undergoing cesarean myomectomy. These researchers also indicated that injury to the uterus may be less traumatic when myomectomy is carried out during cesarean section, compared to during non-pregnancy. 17
Gbadebo et al. conducted a descriptive study in a tropical setting. Among the complications that occurred, the researchers listed anaemia with subsequent need for transfusion (9.1%), puerperal pyrexia and sepsis (9.1%), and fracture of the humerus and the clavicle of the baby (2.3%). No maternal and perinatal mortality were reported. Consequently, these researchers concluded that selection of patients for CM reduces blood loss, anemia and other complications. 30
Park et al. performed cesarean myomectomies with no restrictions based on location, without damaging the Fallopian tubes, even in cases in which the myomas were located in the fundus or proximal to the Fallopian tubes. The researchers concluded that cesarean myomectomy can be performed safely by experienced surgeons. 31
Kim et al. indicated that taking into consideration several factors—such as location, number, fibroid size, proximity to large vessels, and uterine contractility—can be decisive for avoiding postoperative complications. These researchers also suggested that the decision to proceed to cesarean myomectomy should depend mostly on the location of the fibroid growths and the surgeon's experience. More specifically, large, fundal, intramural fibroids in the vicinity of the Fallopian tubes should be avoided. The researchers also indicated that intramural fibroids should, in general, be excised with caution because of the high risk of uterus atony and severe hemorrhage. Kim et al. concluded that cesarean myomectomy can be performed only in selected cases, because some patients may have significant complications such as ileus and postoperative atonic bleeding. 32
Leanza et al. 33 and Igwegbe et al. 34 have also reported large myomas removed during cesarean sections and suggested that the correct handling (high-dose oxytocin infusion and skillful surgery) ensures minimal intra- and postoperative blood losses.
Celal and Hülya also showed that myomectomies that were performed on fibroid growths in appropriate locations did not increase postoperative bleeding or maternal morbidity or mortality. However, according to the experience of these researchers, the duration of the operation was generally increased. Atypia and necrosis was not found in any of the myomectomy samples. 35
Machado et al. described a series of 8 cases, in whom myomectomy was performed during cesarean section for large lower-segment fibroid growths. With an addition of 15 minutes to the operating time and of 1 day to the hospital stay, and with nonsignificant postoperative morbidity, the researchers still suggested that this procedure is safe and effective in experienced hands. 36
Another study, by Mu et al., showed that it is possible to carry a pregnancy successfully to term when the pregnancy is complicated by uterine leiomyomas. When cesarean delivery is needed, myomectomy can be performed at the time of cesarean section routinely without significant complications. 37
Simsek et al., in a study of 70 cases of cesarean myomectomy, found that there was significantly increased blood loss—which however, did not require blood transfusion—in combination with a significant increase in mean surgical time and length of hospital stay. 38
A recent prospective case-control study, by Tinelli et al., investigated the outcome of intracapsular cesarean myomectomy on 68 patients, compared with a control group of 72 patients with myomatosic pregnant uterui, who underwent cesarean section without myomectomy. No difference was found between the intracapsular cesarean myomectomy group and the control group, in terms of pre- and postoperative hemoglobin values, mean change in hemoglobin values, incidence of intraoperative hemorrhage, frequency of blood transfusion, and postoperative fever. The only two parameters that were affected negatively in the group who had intracapsular cesarean myomectomy, were the duration of the operation and the length of hospital stay. 39
Despite the positive outcomes of the studies discussed above, the surgeon should always consider all the parameters before reaching the decision as to whether or not to perform myomectomy during a cesarean section.
Exacoustos and Rosati studied a population of 9 women undergoing cesarean myomectomy. One third of them needed hysterectomy because of severe hemorrhage. These researchers emphasized the role of various ultrasound findings in identifying women at risk for myoma-related complications: size of the myoma; location; relationship to the placenta, and echogenic structure. 40
The current study, in accordance with a previous study conducted in the same hospital, 41 suggests that cesarean myomectomy is a safe procedure when performed by an experienced and skilled surgeon. No severe complications were noted in either of the studies.
Conclusions
Despite the lack of prospective, randomized studies, the retrospective data analyzed in this study clearly showed that the old dictum that discouraged cesarean myomectomy should be reassessed. According to the current authors' experience, the greatest risk for cesarean myomectomy comes from lack of knowledge of the presence or exact position of the myomas. Nevertheless, cesarean myomectomy is a feasible and safe procedure when conducted by experienced surgeons. For this reason, it is suggested that women with known myomas—if they are undergoing elective or emergency cesarean sections—be informed about the possibility of cesarean myomectomy in order obtain informed consent for performing the procedure.
Footnotes
Disclosure Statement
No financial conflicts of interest exist.