
Abstract
Abstract
Introduction
I
The mesothelial lining of the peritoneal cavity has been shown on electron microcopy to retract and bulge when exposed to a CO2 pneumoperitoneum during laparoscopic surgery. 8 The current authors showed that laparoscopic surgery is followed by acute inflammation in the entire peritoneal cavity, being the cumulative result of mesothelial-cell trauma. 9 Detrimental factors were identified as being pneumoperitoneum with CO2 (mesothelial hypoxia),10,11 with >10% of oxygen (reactive oxygen species), 12 desiccation, and a mechanical trauma. Beneficial factors were identified as the addition of small amounts of N2O13,14 or 4% of O2 to the pneumoperitoneum, and cooling of the peritoneal cavity, and preventing desiccation.13–16 This combined treatment, known as full conditioning, reduced adhesion formation by >85% in a laparoscopic mouse model. 17
The lining of the peritoneal cavity is a large area, and mesothelial cells modulate transport actively. Exchange of fluid and substances smaller than 60 daltons is known to be rapid. Larger molecules probably diffuse much more slowly, because the concentrations of luteinizing hormone, follicle-stimulating hormone, and sex-hormone–binding globulin is only 60% of the plasma concentration,17–19 whereas large proteins, such as as CA125 and PP14, secreted in the peritoneal cavity are much higher than in plasma. 20 It is unclear if mesothelial-cell retraction exposing the basal membrane and/or extracellular matrix directly affects resorption rates.
In 2010, the current authors validated a noninvasive method to measure peritoneal fluid volume by using transvaginal ultrasound 21 with a coefficient of variation of 19.3% and 7.3%, between and within patients, respectively.
This noninvasive measurement of peritoneal fluid volumes was therefore chosen to assess the resorption rate of Ringer's lactate and of 4% icodextrin. Given that full-conditioning prevents mesothelial-cell retraction and acute inflammation following CO2 pneumoperitoneum, the hypothesis was that full conditioning would slow the resorption rate of fluids down.
Materials and Methods
Full conditioning of the peritoneal cavity
Full-conditioning was derived from the results obtained in the current authors' laparoscopic mouse model and from the results of cooling the peritoneal cavity in women. 15 Instead of using CO2 for the pneumoperitoneum, a mixture of 86% CO2, 10% of N2O, and 4% of O2 was used. As described, the peritoneal cavity was cooled to 30°C by sprinkling 2–3 mL/minute of saline and the gas was humidified using a Fisher & Paykel humidifier (Fisher and Paykel Healthcare Ltd., Auckland, New Zealand) modified by eSaturnus (Leuven, Belgium) to deliver fully humidified gas of 31°C to the patients. Upon entrance in the peritoneal cavity, some cooling and condensation occurred thus preventing any desiccation. 15
Patients and randomization
Following approval by the central ethics committee of the Katholieke Universiteit Leuven, in Leuven, Belgium (S52424) on September 3, 2010, the trial was registered on www.clinicalTrials.gov with identification NCT01344499 (April 21, 2011) and, subsequently, the trial was proposed to 20 women scheduled to undergo laparoscopic total or subtotal hysterectomy for benign conditions (i.e., menorrhagia). For this-single surgeon (J.V.) trial, exclusion criteria were other pathology that was expected to increase the duration of surgery, such as a uterus of more than 300 g (judged clinically or by ultrasound), deep endometriosis (judged clinically), or severe adhesions (if more than 1 minor previous intervention), or any other disease that could affect the peritoneal cavity.
After informed consent had been obtained, the women were randomized by the research nurse to one of four groups using sealed envelopes: (1 and 2) either a pneumoperitoneum with CO2 or with full conditioning; and (2 and 3) receiving after surgery either 1 L of Ringer's lactate or icodextrin 4%. The surgeon was informed the day of surgery of the the patient's randomization group. All women entered the trial and there were no dropouts (Fig 1).
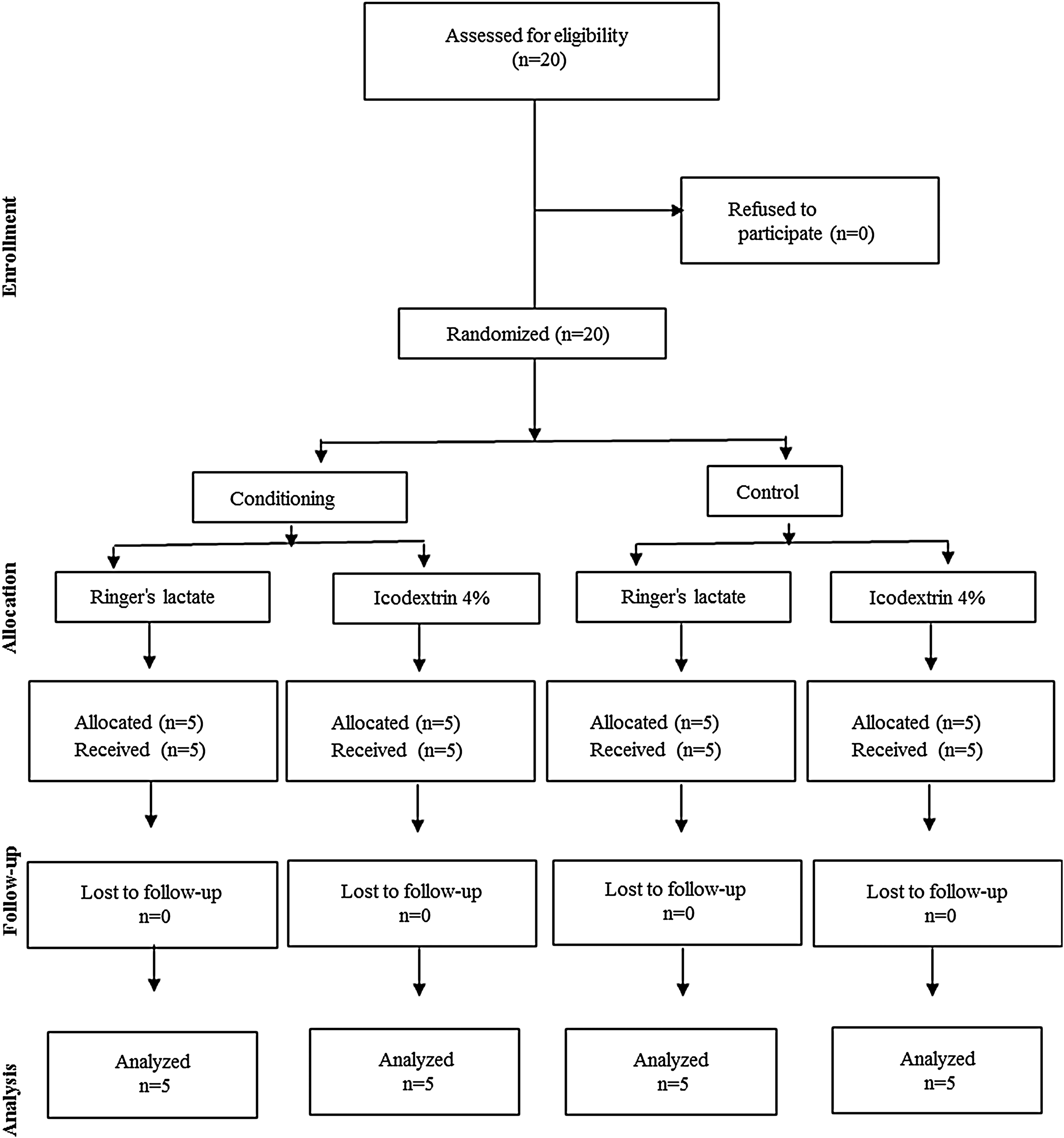
Consolidated Standards of Reporting Trials flow diagram.
Study design
The primary endpoints of this trial were the resorption rate from the peritoneal cavity of Ringer's lactate or icodextrin 4% and the effect of full conditioning, compared with pure CO2 upon these resorption rates. A factorial design was used to compare the resorption rate of Ringers lactate and of icodextrin 4% simultaneously, and to evaluate the effect of full conditioning. During surgery either humidified (MR860, Fisher and Paykel Healthcare Ltd.) CO2 or full conditioning was used. Rinsing was performed with Ringer's lactate, but any remaining fluid at the end of surgery was aspirated from the pouch of Douglas after placing the patient in an anti-Trendelenburg position. After surgery, the surgeon was informed which fluid should be used for the trial, and either 1000 mL of Ringer's lactate or 1000 mL of icodextrin 4% was left in the abdominal cavity. The volume of the fluid remaining in the peritoneal cavity was estimated by ultrasound at times 0 (10 minutes after instillation), 24 hours, 48 hours, and 72 hours.
Surgery
The laparoscopic hysterectomy was standard surgery, and the only difference between the 2 groups during surgery was the pneumoperitoneum. The insufflation pressure was 15 mm Hg. Hysterectomy was performed with 1 umbilical trocar and 3 secondary trocars, bipolar coagulation, and laparoscopic suture of the vaginal cuff or cervical stump. Rinsing was done with Ringer's lactate containing 5000 IU of heparin/L (Leo, Belgium).
Measurement of peritoneal volume
As described before, 21 women were placed in a 30° anti-Trendelenburg position and, after 1 minute, the three dimensions (length, height and depth) of the pocket of fluid was measured 3 times by ultrasonography using an Esaote Technos system with a 6.5-MHz transvaginal probe (Esaote, Genoa, Italy). Using these measurements, the peritoneal volume was calculated. When assessing peritoneal fluid after 24, 48, or 72 hours the ultrasonographer (R.C.) was blinded to the randomization group of the patients. All scans were performed within 1 hour of the time indicated. All patients completed the trial.
Statistics
Given that the within-patient coefficient of variation of the peritoneal fluid–volume measurement by ultrasound is only 7%, compared with 19% between patients, within-patient measurements were used. Therefore, fluid volumes remaining after 24, 48, or 72 hours were expressed as the percentage of fluid remaining, compared with the measured volume immediately after surgery.
Statistical analysis was performed with the SAS system (SAS Institute Inc., Cary, NC,) using Wilcoxon–Kruskal-Wallis to calculate differences between the groups. Means and standard error of the mean are given unless indicated otherwise.
Results
The weight of the uteri was <250 g and duration of surgery <90 minutes in all patients. No major adhesions or other pathology (such as endometriosis) was found. No women were excluded from the trial after signing informed consent.
Fluid absorption of both Ringer's lactate and icodextrin 4% was fast and exponential. Following a pneumoperitoneum with CO2, the resorption rate of Ringer's lactate was faster than for icodextrin 4%. After 24, 48, and 72 hours 11.7±1.0% versus 38.2%±9.5% (p=0.009), 5.3%±0.6% versus 14.9%±4.8% (NS), and 4.2%±0.7% versus 12.1%±4% (p=0.03) of the initial 1 L remained, respectively.
Conditioning decreased the resorption rate of Ringer's lactate and, after 24, 48, and 72 hours, 25.2%±3.4%, 13.2%±1.3%, and 6.0%±0.5% remained (p=0.03, 0.009, and NS versus the control group), respectively. Conditioning did not affect the resorption rate of icodextrin, of which 32.6%±11.1%, 13.2%±5.5%, and 4.4%±1.9% remained after 24, 48, and 72 hours, respectively (NS versus the control group; Fig 2).

Percentage of fluid volume remaining after instillation of 1000 mL of Ringer's lactate or icodextrin 4%, following CO2 pneumoperitoneum or pneumoperitoneum with conditioning, respectively. Means and standard error of the means of consecutive ultrasound measurements are depicted.
Discussion
These data showed that the resorption of Ringer's lactate is exponential and very fast after surgery, with only some 10% remaining after 24 hours. This could explain the marginal effect if any on adhesion formation. There are, however, no data on the necessary amount of fluid to prevent adhesions.
Surprisingly, the resorption rate of icodextrin 4% was equally exponential as that of Ringer's lactate, although the icodextrin 4% rate clearly slower, with 38% remaining after 24 hours. These data are in contradiction with the reported retention time of 3–4 days. 3 The current authors suggest that this aberrant resorption curve and the long retention time could have been caused by the fact that the small number of women investigated had undergone debulking and intraperitoneal chemotherapy for colorectal cancer. They indeed had received intraperitoneal chemotherapy every second week, alternating with instillation of 2 L of icodextrin 4%, compared to Ringer's lactate. The current authors' finding of a much faster resorption of icodextrin 4%, could explain the less-than-expected efficacy in decreasing postoperative adhesions.4–7 The reported slower absorption rate for Ringer's lactate 22 is difficult to account for, as the volumes used are smaller and the technique to measure the residual volume can be debated.
The fluid used for rinsing during surgery was not expected to cause a substantial bias. The fluid was indeed removed carefully prior to instillation of the fluid for the trial. In addition, the amount of fluid used during a laparoscopic hysterectomy was low, rarely exceeding 200 mL.
Following conditioning, the resorption rate of Ringer's lactate was much slower than following CO2 pneumoperitoneum, thus, confirming the hypothesis that mesothelial cells would retract less with conditioning of the peritoneal cavity. The remaining volumes were no longer significantly different from those of icodextrin 4%, although this absence of significance could be the result of the small number of patients in each group. Conditioning, surprisingly, did not affect the resorption rate of icodextrin 4%, which remained unchanged. To explain this difference between Ringer's lactate and icodextrin 4%, the current authors have to postulate that retraction of mesothelial cells exposing the basal membrane directly does increase resorption rate for small molecules but not for molecules >30.000 daltons, such as as icodextrin. Moreover, the data might indicate that, following conditioning, the efficacy of Ringer's lactate will no longer be much different from the efficacy of icodextrin 4% for adhesion prevention. This, however, will be difficult to demonstrate in a randomized controlled trial when the huge efforts necessary to prove the limited efficacy of icodextrin 4% are taken into account.4–7
The idea that factors from the peritoneal cavity enhance adhesion formation at trauma sites and that, quantitatively, this enhancement is more important than the surgical lesion itself, sheds new light on the mechanism of action of flotation agents. In addition to keeping surfaces separated these fluids also dilute any substances in the peritoneal cavity. The limited efficacy of these fluids, therefore, suggests that either this dilution does not decrease the effect substantially or that the duration of dilution is too short. In addition, the effect of any of these flotation agents upon the mesothelial cells and the subsequent acute inflammatory reaction has not been documented and can only be speculated about.
Conclusions
These data explain why flotation agents, including icodextrin 4%, following surgery are not that effective for decreasing adhesion formation. These data, moreover, do not confirm the longer retention time of icodextrin. The data do confirm that, after conditioning, resorption of Ringer's lactate is slower, leaving some 250 mL after 24 hours.
Footnotes
Acknowledgments
The current authors thank the Leuven Quality surgery fund that—with the help of Nordic Pharma, Fisher and Paykel (New Zealand), and eSaturnus (Leuven Belgium)—supported this trial. Thanks are also extended to Mercedes Binda, PhD (KULeuven), Christophe Lauwerys (EndoSAT NV), and Diane Wolput, RN. Special thanks are due to Karina Mailova, MD, PhD (Moscow, Russia), Anastasia Ussia, MD, and Carlo De Cicco, MD, (both in Rome, Italy) for conceptual discussions about full conditioning and for revising the article. ESaturnus NV and Fisher and Paykel are acknowledged for supplying the equipment necessary for this trial.
Disclosure Statement
None of the authors of this article have a conflict of interest, except P.R. Koninckx, who is a stockholder in EndoSAT NV.