
Abstract
Abstract
Introduction
C
Case
A 55-year-old postmenopausal female (para 4) presented in Department of Obstetrics and Gynecology, King George Medical University, Lucknow, Uttar Pradesh, India, with a history of irreducible genital prolapse of 10 years' duration. This prolapse was associated with an intermittent foul-smelling, blood-mixed discharge and voiding difficulty. There was no history of urinary frequency or urgency, postcoital bleeding, fever, lower abdominal pain, weight loss, chronic cough, or constipation. This patient's past history or contact history was negative for tuberculosis. On general examination, the patient was noted to be of a poor build with moderate pallor. Her systemic examination was within normal limits. Per speculum examination, a 5×5–cm, irregular, fungating mass was seen protruding from her introitus. Her cervical lips were not noticeable. A uterine sound was inserted through the cervical os (Fig. 1). Thus, a growth replacing all of the cervix was noted. Hence, a clinical diagnosis of cervical cancer or genital tuberculosis with a third-degree cervical descent was made.

Uterine sound inserted through the cervical os.
With respect to laboratory tests, this patient's chest X-ray was normal; a Mauntaux test was negative; and blood work revealed moderate anemia, a raised total leucocyte count with lymphocytosis, and a normal erythrocyte sedimentation rate. Pelvic ultrasonography revealed a normal uterus and adnexa. Cystoscopy was positive for mild inflammatory changes and edema at the triagone. A Papanicolaou smear revealed chronic inflammation. A biopsy from the cervical growth revealed chronic cervicitis with no evidence of dysplasia.
The patient underwent surgery to correct her third-degree cervical descent. A panhysterectomy was performed. Her bladder was noted to be adherent to her uterus. The left infundibulopelvic ligament was thickened. On gross examination, her uterus was atrophic with a bulky cervix. A cut section of the specimen showed smooth endometrial and endocervical canals. (Fig. 2).
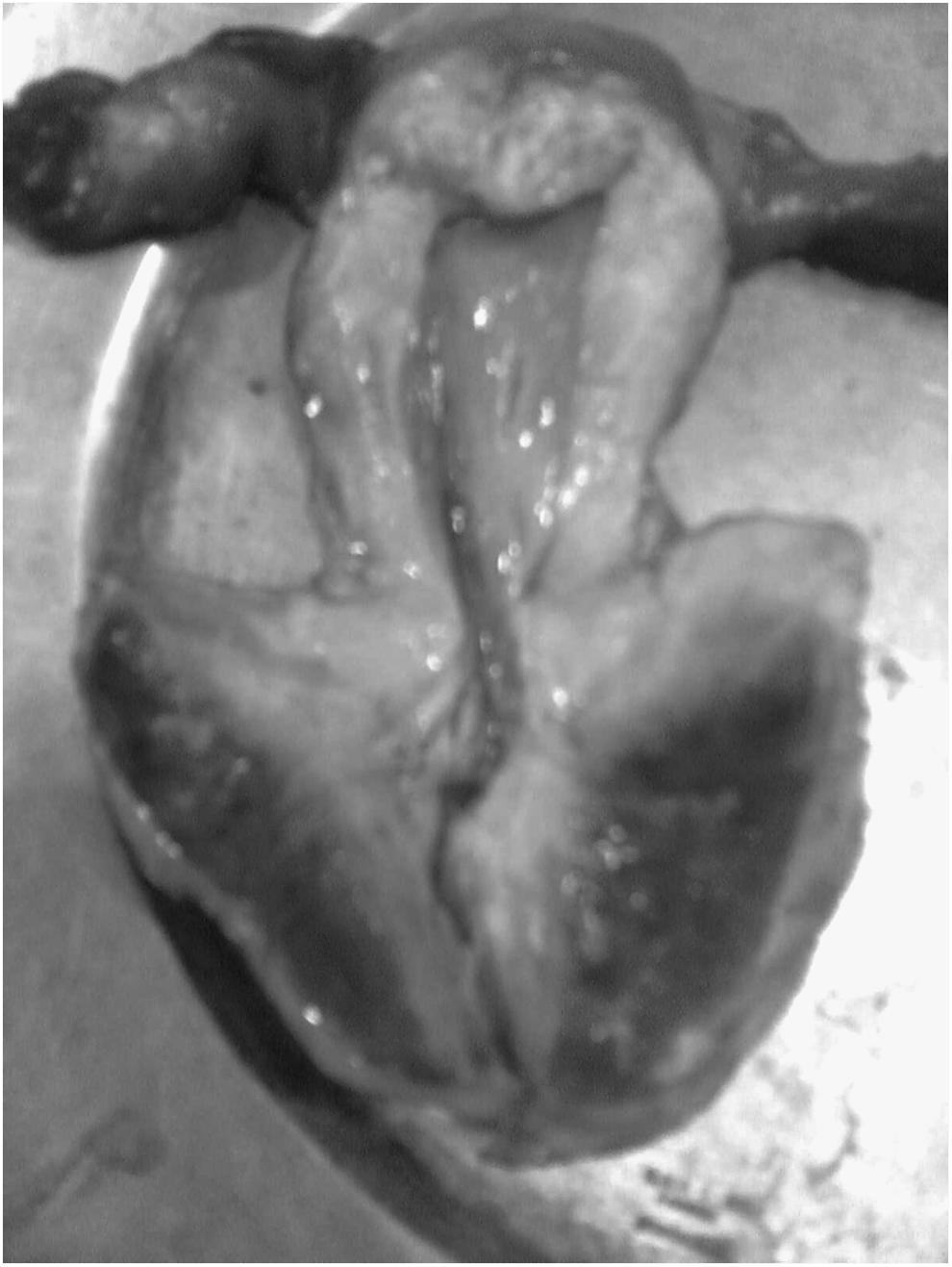
Cut section of the patient's uterus and cervix showing gross hypertrophy of her cervix.
Results
Histopathology results from the specimen were consistent with chronic cervicitis. The patient's postoperative period was uneventful.
Discussion
Exophytic cervical growth is usually seen in cases of cervical malignancy. Some benign cervical conditions, such as cervical tuberculosis, cervical fibroid growths, or cervical polyps, may also present as cervical growths, but chronic cervicitis presenting in a similar manner is rare and usually a result of delayed treatment of this otherwise medically managed condition. A cervical polyp is very common and easily diagnosed. A problem persists for patients with chronic cervicitis and cervical tuberculosis, both of which are rare,4–6 at times associated with athird-degree cervical descent,7,8 and present as growths resembling cervical carcinomas.
A review of the literature, using search words such as
Nigam et al. 10 reported a case of a 21-year-old, unmarried nulliparous female with a history of a mass protruding from her vagina and a discharge from her vagina; this condition had lasted for 8 years. A local examination revealed a large, reducible cystic swelling protruding from the introitus. Ultrasonography findings on this patient were normal except for the presence of an anechoic cyst in her cervix. She underwent a cystectomy, and histopathologic testing revealed the presence of a Nabothian cyst. On follow-up, reduction of this patient's prolapse to the first degree was noticed after 6 weeks.
Conclusions
The current case was unique because of the signs (size and friability) mimicking cervical carcinoma so much so that it was difficult to discern the cervical os. It is rare to find cervical cancer with prolapse.11,12 There are only a few case reports of chronic cervicitis with third-degree prolapse.2,3 Hence, such cases should be managed with patience, so that complete evaluation can be performed. Surgical intervention should be implemented for a patient after histologic confirmation of the lesion.
This case also highlights the lack of patient awareness in developing countries as a result of which patients present in late stages with unusual presentations leaving no choice for the physicians for cases which if recognized early can be treated medically.
Footnotes
Acknowledgments
This case was diagnosed and managed by Dr. Nisha Singh. The manuscript was prepared by Dr. Anubha Arorae, and revised by Dr. Nisha Singh.
Disclosure Statement
There were no commercial associations of either author that might create a conflict of interest in connection with this article. There are no conflicts of interest, actual or potential, to be disclosed.