
Abstract
Abstract
Introduction
C
Case
A 50-year-old, parous postmenopausal woman presented with a 4-month history of watery vaginal discharge and lower abdominal pain. Her general condition was fair and, on examination of abdomen, tenderness was elicited in the left iliac fossa without any palpable mass. Per speculum examination showed watery vaginal discharge through external os. A bimanual examination revealed a normal-sized uterus and a tender, solid left adnexal mass. Tranvaginal sonography showed a normal-sized uterus with a small fibroid and fluid-filled endometrial cavity; the right side ovary was 2.5×2×1.5 cm and left ovary was not visualized. A well-defined heterogeneous left adnexal mass of size 5×4.5 cm with solid and few cystic areas with increased peripheral vascularity was seen (Fig. 1). Contrast Enhanced Computer Tomography (CECT) of the abdominal–pelvis revealed a well-defined heterogeneously enhancing solid mass lesion posterior to the bladder in the midline and extending to the left adnexa. It measured 6×4.5×4.1 cm without any infiltration into the uterus (Fig. 2). The left ovary was not seen separately from the mass and the right ovary was normal. No ascites or enlarged lymph nodes were seen. The CA-125 level was 8.5 IU/mL. Pap smear showed a normal cytology; both the vaginal fluid cytology and the diagnostic curettage were negative for malignant cells.

Transvaginal ultrasonography showing a retroverted uterus, sausage-shaped and well-defined heterogeneous left adnexal lesion with solid and few cystic areas.
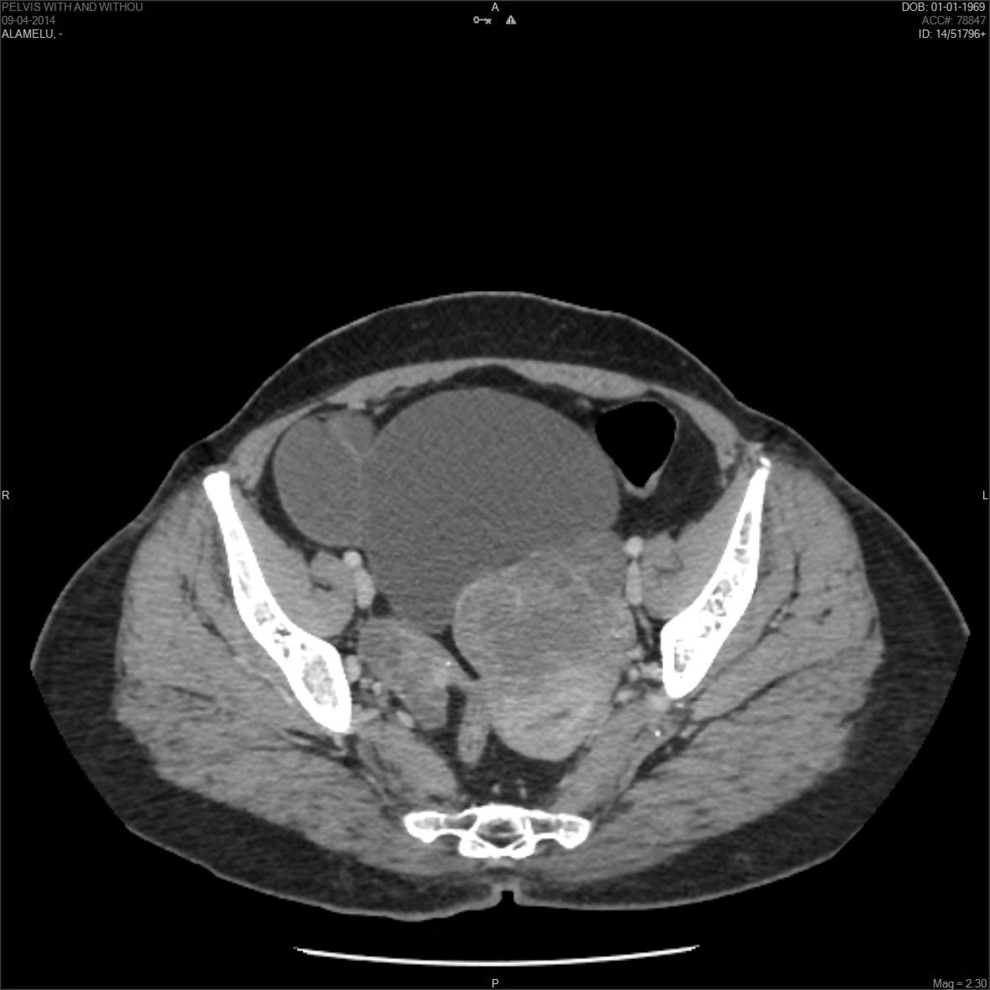
Abdominopelvic CECT showing endometrial cavity collection and a well-defined heterogeneously enhancing solid lesion seen posterior to the bladder in the midline and extending to the left adnexa. CECT, Contract Enhanced Computer Tomography.
Even though the imaging studies, tumor marker (CA-125), and the vaginal fluid cytology were not helpful in evaluating the nature of adnexal mass, clinically, there was a suspicion of fallopian tube carcinoma. This was due to the presence of the classical triad of watery vaginal discharge, pelvic pain, and a pelvic mass. Therefore, we proceeded for staging laparotomy comprising total abdominal hysterectomy with bilateral salpingo-oophorectomy, omentectomy, and selective lymphadenonectomy. Intraoperatively, we found a unilateral, solid tubal mass arising from the fimbrial end of left fallopian tube of size 6×5×5 cm. The contralateral tube was normal and bilateral ovaries were atropic and found separate from the mass. The uterus was normal in size and there was no evidence of any peritoneal deposits, ascites, or enlarged lymph nodes. On gross examination, the uterus was normal in size with multiple seedling fibroids and distended endometrial cavity lined by thin endometrium (Fig. 3). The right side tube and both ovaries appeared normal. The left fallopian tube was grossly dilated with a smooth outer surface and a solid mass arising at the fimbrial end of the tube measuring 6×5×5 cm. The cut surface of tube showed a gray white friable tumor occupying the dilated tubal lumen and a solid fimbrial mass with areas of hemorrhage. Histopathology revealed a normal right fallopian tube and bilateral ovaries. The microscopic examination of left fallopian tube showed tumor arising from tubal epithelium infiltrating the submucosa and muscularis layer, tumor cells were arranged in solid sheets and a papillary pattern, and cells were pleomorphic with a high nuclear to cytoplasm ratio (Figs. 4, 5). The omentum bilateral ovaries were free of tumor cells and the peritoneal washing was negative for malignant cells. Based on the above findings, a diagnosis of primary fallopian tube carcinoma of papillary serous type with FIGO Stage 1A was made. After uneventful recovery from the postoperative period, further treatment with adjuvant chemotherapy was planned for the patient.

Gross picture showing uterus with multiple seedling fibroid and distended endometrial cavity. Dilated left fallopian tube with a solid mass arising from the fimbria end.

Histopathology picture showing tumor cells invading upto muscularis layer of fallopian tube, with tumor cells arranged in sheets and cords (hematoxylin and eosin [H&E], 5×).

Histopathology picture showing tumor cells showing pleomorphic vesicular nuclei with prominent nucleoli, scanty cytoplasm, and increased nucleus to cytoplasmic ratio.
Discussion
Primary fallopian tube carcinoma usually presents in the fifth or sixth decade of life with peak age of incidence at around 54 years. 7 Nulliparity, infertility, inflammatory pelvic disease, and the presence of BRCA genetic mutation, although not well established, are considered to be the risk factors for developing primary fallopian tube carcinoma.8,9 Symptoms include profuse vaginal discharge, abnormal vaginal bleeding, pelvic or abdominal colicky pain, and a palpable pelvic and/or abdominal mass. 10 Latzko's triad, which comprises watery vaginal discharge, pelvic and/or abdominal colicky pain, and a pelvic mass, is pathognomonic of fallopian tube carcinoma, but this is seen in less than 15% of the patient. 11 A differential diagnosis of primary fallopian tube carcinoma should be kept in mind in patients presenting with vaginal discharge or abnormal genital bleeding with negative diagnostic curettage. 8 The presence of a sausage-like image with incomplete septation and a highly vascular solid component seen on sonography for adnexal masses should be considered in the differential diagnosis for primary fallopian tube carcinoma. 12
The effectiveness of cytological diagnosis from the cervical and vaginal pool sample is widely variable and has been reported as positive in 40%–60% of women with tubal carcinoma. 13 The CA-125 antigen, which is expressed in the fallopian tube carcinoma, is seen to be elevated in 65% of patients, which can be used in diagnosis and follow-up. 14 Primary site for PSC remains debatable. Evidence supporting the idea that serous tubal intraepithelial carcinomas (STICs) and early invasive tubal carcinomas are the precursors of ovarian/peritoneal high-grade serous carcinomas (HGSCs). This idea is supported by two distinct inter-related variables: cell of origin and molecular pathway. The possible mechanism for the origin of ovarian HGSC is dislodgement of normal tubal epithelium from the fimbria, which may implant at the rupture site of ovulation, resulting in the formation of an inclusion cyst that may undergo malignant transformation or malignant cells may exfoliate and implant on the ovarian surface. This is supported by evidences like easy dislodgement of tubal epithelial cells after flushing the fallopian tube; most of the ovarian epithelial inclusions (OEIs) and serous cyst adenoma display morphological features and an immunophenotype of tubal-type epithelium (PAX8 positive/calretinin negative/tubulin positive) and the mesothelium-derived OEI cyst cannot grow into tumor masses due to a low cellular proliferative activity, compared to fallopian-derived OEIs that showed a high proliferative activity.15,16 Other molecular evidences supporting this proposal are as follows: in women with BRCA mutations who had undergone risk reducing salpingo-oophorectomy, their specimens showed the presence of occult carcinoma more in the fallopian tube than in the ovary. The presence of identical TP53 mutation or coexpression of p53, p16, FAS, Rsf-1, and cyclin E factors in STICs and concomitant ovarian/peritoneal HGSCs further supports the clonal relationship between them, and significant difference in telomere length between STICs and concomitant ovarian/peritoneal HGSCs supports its precancerous state. 17 Serous carcinoma from the fimbrial site is not easily recognized as primary fallopian tube carcinoma because it could either spread rapidly to other sites or become complexed with the ovary. 6 The diagnosis of primary fallopian tube carcinoma is rarely considered preoperatively and it is usually first appreciated at the time of surgery or postoperatively by the pathologist. A correct diagnosis of this carcinoma was made preoperatively in only 4.6% of cases in the series reported by Alvarado-Cabrero et al. 18 Four criteria for diagnosis of fallopian tube serous carcinoma are that (i) the main tumor is in the fallopian tube and arises from the endosalphinx, (ii) histology matches the tubal phenotype, (iii) if the tubal wall is invaded, there has to be an evident transition between normal and malignant tubal epithelium, and (iv) the fallopian tube should contain more tumor than the ovary or endometrium. 19 Our case was diagnosed to be primary tubal serous carcinoma of fimbrial origin as it presented as a diffuse replacement of the fimbrial epithelium by the tumor and histologically it met the criteria of fallopian tube serous carcinoma by arising from the endosalpinx; it matches the tubal phenotype and there was no evidence of tumor in the ovary, endometrium, and peritoneal surface. This was possible after thorough sectioning and extensive examination of the fimbrial end of the tube. The FIGO system for staging of fallopian tube carcinomas is similar to the surgical staging for ovarian carcinoma. It spreads by local invasion, transluminal migration through lymphatics and by bloodstream and, compared to epithelial ovarian carcinoma, it has a higher rate of retroperitoneal and distant metastasis. 8 Para-aortic lymphadenopathy has been documented in 33%, and the 5-year survival rate with all stages of disease has been reported to range from 30% to 50%. 20 The stage of disease at the time of diagnosis is the most important factor affecting prognosis, and the other reported prognostic factors include residual disease after initial surgery, extent into the fallopian tube and the depth of invasion into its wall, location of the tumor within the tube (fimbrial or nonfimbrial), advanced age, serous versus endometroid variety, bilaterality, positive peritoneal cytology, HER2/neu expression, P53 alteration, and elevated pretreatment CA-125 level.20,21 Surgery is the treatment of choice for any stage of fallopian tube carcinoma, and the surgical principles are the same as those used for ovarian carcinoma, the procedure of choice being total abdominal hysterectomy, bilateral salpingo-oophorectomy, omentectomy, and selective pelvic and para-aortic lymphadenonectomy. Postoperative adjuvant chemotherapy is similar to ovarian carcinoma. Patients having high-risk stage I, stage II, and advanced disease are candidates for combination of taxane- and platinum-based adjuvant chemotherapy. In our case, we followed the same surgical protocol and adjuvant chemotherapy was planned in view of the tumor invasion into the muscle layer, its poor differentiation, and in proximity to the fimbrial end. The role of postoperative radiotherapy is unclear. 20 The 5-year survival of fallopian tube carcinoma is 50.8% for stage I and II disease, which is worse when compared to 77.5% in ovarian malignancy. 22
Conclusion
Treatment of rare malignancies is always problematic as there is usually no standard therapy, which holds true for fallopian tube carcinoma. Resemblance to ovarian carcinoma has led to its treatment in a similar line. This case is being reported as the clinical presentation was classical, but we still faced a preoperative diagnostic dilemma. Our surgical treatment was adequate and postoperative adjuvant chemotherapy was planned because no definitive treatment protocol for early-stage disease exists. This needs further clinical trials, and hence, the treatment may be individualized on a case to case basis.
Footnotes
Acknowledgments
I would like to sincerely thank the Departments of Pathology and Radiodiagnosis for their support in interpreting and providing the histology slides and images. I would also like to extend my gratitude to my colleague Dr. Rupal Samal, assistant professor, Department of Obstetrics and Gynecology, MGMC and RI, Puducherry.
Disclosure Statement
No competing financial interests exist.