
Abstract
Abstract
Introduction
L
In 2010, two major retrospective reviews from Korea concluded that LESS hysterectomy for benign indications was associated with significantly lower immediate postoperative pain scores, less blood loss, improved cosmetic outcomes, and comparable surgical outcomes.2,3 Several randomized trials4–7 as well as a meta-analysis 8 compared multiple-port with LESS hysterectomy and showed similar rates of complications, comparable amounts of blood loss, longer operative times, and no significant difference in administered analgesics.
Proposed reasons for low acceptance of LESS include the technical difficulties inherent in a single-site approach. The loss of instrument triangulation results in instrument crowding and collisions (“sword fighting”), reduced visualization, and a limited operative work space. 2 Most studies describing experience with LESS hysterectomy are multi-institutional.2–4,9 They report the pooled experience of multiple providers.6,7 Consequently, they do not reflect the single-provider experience, a perspective that is most relevant to the individual practitioner.
The current study explored the initial experience of a single surgeon in a single institution who transitioned from performing conventional multiport laparoscopic hysterectomies to performing LESS hysterectomies, thus eliminating potential selection bias (e.g., a more-experienced surgeon performing one type of procedure and a less-skilled surgeon performing the other type of procedure). The study objective was to analyze surgical outcomes and experience with LESS as a primary approach to all benign hysterectomies during the first year of implementation of a single-incision program.
Materials and Methods
This retrospective cohort study was approved by the institutional review board of Huntington Hospital, a northeastern U.S. community hospital. In February 2010, a single surgeon (J.W.) switched his surgical approach to benign hysterectomies from traditional multiport laparoscopy to LESS. His experience was analyzed 1 year before and after initiation of the single-incision program. The clinical, demographic, and surgical outcomes of patients who had conventional laparoscopic supracervical hysterectomy or total hysterectomy (C-LSH/TLH) were compared with the patients undergoing the LESS approach.
Patients
Inclusion criteria were all women who had hysterectomies performed by the senior author (J.W.) from October 2008 to February 2011 using the laparoscopic approach. Cases that had been operated on during a 4-month period when the technique for LESS supracervical hysterectomy was developed were excluded. 10 A pig laboratory was initially utilized to help the senior surgeon develop single-site surgical skills.
The first LESS hysterectomy was performed in February 2010. All patients after that had a primary LESS approach to hysterectomy and were included in the study. Demographic data, intraoperative factors, and postoperative outcomes of the 37 patients in the LESS group (February 2010 to February 2011) were compared with those of the 41 patients in the C-LSH/TLH group (October 2008 to October 2009). Most of the patients had surgery for symptomatic uterine leiomyoma causing prolonged heavy vaginal bleeding and dysmenorrhea. Patients were evaluated preoperatively for eligibility of a laparoscopic approach based on the size and mobility of the uterus. No patients were denied a laparoscopic approach based on prior surgical history. Criteria did not vary by year. Four patients were found to be ineligible for a laparoscopic approach in the C-LSH/TLH group, and 3 patients were found ineligible in the LESS group.
Surgical procedure
As noted, all surgeries were performed by the senior author (J.W.) who was assisted by a resident. For LESS, the abdominal entry was performed utilizing a single 1.5–2.0-cm vertical intraumbilical incision according to the open Hassan technique. A multichannel single-port system was introduced. Three different port systems were used based on the suitability of the clinical situation and the surgeon's preference—SILS Port Multiple Instrument Access Port (Covidien, Mansfield, MA), GelPOINT (Applied Medical, Rancho Santa Margarita, CA), SSL (Ethicon Endo-Surgery, Cincinnati, Ohio). A bariatric-length, 5-mm, straight 30° laparoscope was used. Dissection, hemostasis, and tissue transection were achieved using the Harmonic Ace+Sheers (Ethicon Endo-Surgery) and the Kleppinger Bipolar Forceps (Superior Surgical, Pottstown, PA). No articulating or curved instruments were utilized. Cervical transection was performed using the LiNA Gold Loop (LiNA, Norcross, GA).
During the surgery, the straight laparoscope was always positioned immediately parallel to and adjacent to the harmonic scalpel or bipolar forceps. For supracervical hysterectomy, morcellation was performed through the umbilicus with a #15 scalpel (Fig. 1) or laparoscopically using a Karl Storz 10-mm morcellator (El Segundo, CA) with transcervical visualization. 10 For TLH, the specimen was retrieved through the vagina. When appropriate, the current authors prefer to perform a supracervical hysterectomy rather than a total hysterectomy because of the lower risk of urinary-tract injury, as well as the potential for shorter operative time and lower risk of morbidity.11,12

Extracorporeal morcellation. Traction on the uterus applied through umbilical incision. Morcellation performed with a #15 blade.
Conventional laparoscopic surgery was performed with four ports for access. Standard laparoscopic instruments were used, and a similar technique was utilized. Each specimen was morcellated through a 12-mm accessory port. All patients were followed and examined for possible complications within 2 weeks and then 6 weeks from discharge.
Outcomes
The primary outcomes were operative time (time of incision to skin closure). Secondary outcomes included estimated blood loss (EBL), number of conversions to laparotomy, surgical complications, and utilization of accessory ports during LESS.
Statistics
Assuming a clinically significant difference in terms of length of surgery on the order of 30 minutes and an estimated standard deviation (SD) of 45 minutes, a sample size of 36 patients per group was calculated to be necessary to provide a 80% power to detect an effect size of 0.67, with α=0.05. Descriptive statistics were analyzed as mean±SD in the case of normally distributed variables, median (minimum, maximum) in the case of skewed variables, and frequency (%) in the case of categorical variables. Group differences were compared using the Student's t-test or a one way analysis of variance in the case of normally distributed outcomes, the Mann-Whitney–U test in the case of skewed outcomes and the χ2 or Fisher's exact test in the case of categorical outcomes. A two-tailed p<0.05 was considered to be significant. Statistical analysis was performed using SPSS 20.0. (SPSS, Chicago, IL).
Results
Forty one patients underwent C-LSH/TLH, and 37 patients had a LESS approach to hysterectomy. No statistical difference were found for mean age (p=0.354), body mass index (p=0.937), or number of previous abdominal surgeries (p=1.0) between the two groups. The median weight of the uterine specimens, as reported by pathology, was significantly higher in the LESS group (161 g [range: 47–733g]) than in the in C-LSH/TLH (99 g [range: 53–350g]) at p<0.001 (Table 1).
Mean±standard deviation (minimum, maximum).
Median (minimum, maximum).
C-LSH/TLH, conventional laparoscopic supracervical hysterectomy or total hysterectomy; LESS, laparoendoscopic single-site surgery; BMI, body mass index.
As shown in Table 2, there was no significant difference between groups in the proportion of patients requiring adhesiolysis (p=0.61) or in EBL (p=0.13. Overall the operative times did not differ significantly between the groups with a mean of 122±29 minutes in C-LSH/TLH group and 129±40 minutes in the LESS group (p=0.39). The actual mean difference in operative times was far less than what was considered to be clinically meaningful. Comparing the length of the first 19 LESS cases with the last 18 LESS cases it was found that the operative time for the first group was significantly longer (142±38 minutes) then the operative time for the last group (116±41 minutes; p=0.03). When operative time for the first 19 LESS cases was compared to the C-LSH/TLH, the p-value was 0.04. When operative time for the last 18 LESS cases was compared to the C-LSH/TLH, the p-value was 0.53.
Frequency (minimum, maximum).
Median (minimum, maximum).
Mean±standard deviation (minimum, maximum).
p-Value comparing length of cases 1–19 with cases 20–37.
C-LSH/TLH, conventional laparoscopic supracervical hysterectomy or total hysterectomy; LESS, laparoendoscopic single-site surgery; EBL, estimated blood loss, min, minutes.
Each group had one conversion to laparotomy. In the C-LSH/TLH group the conversion was required because of the presence of extensive adhesions and technical difficulties. In the LESS group, a minilaparotomy was performed to repair a bladder and bowel injury in a patient with two prior cesarean sections and severe anterior abdominal-wall adhesions. Another patient in the LESS group had significant blood loss requiring one packed red blood cells transfusion. All of the patients, except for the 3 mentioned above, were discharged within 24 hours after their procedures. No other intraoperative complications were noted.
Fourteen (39%) cases in the LESS group required placement of at least one additional trocar. Comparing the early LESS group with the late LESS group it was found that, in the first 19 cases 8 (42%) patients were operated on with an additional trocar, while, in the last 18 cases, 6 (33%) patients had an additional trocar (p=0.67). Only 5-mm trocars were used for accessory ports. In 1 case, one additional trocar was placed in the left lower quadrant. In 10 of 14 cases 2 additional trocars were placed—one on the left and one on the right side in the lower quadrants medial to the anterior superior iliac spines. In 3 cases, 3 additional trocars were placed. Cases in which placement of additional trocars was required were more complex—the patients tended to have larger uteri (p=0.09), more blood loss (p<0.001), and longer operative times (p<0.001; Table 3).
Mean±standard deviation.
median (minimum, maximum).
LESS, laparoendoscopic single-site surgery; min, minutes.
Discussion
Main findings
The operative time did not differ significantly between a C-LSH/TLH group (122±29 minutes) and LESS group (129±40 minutes). In the current series there was only one conversion to laparotomy and one transfusion among the 37 women in the LESS group. This compared favorably with the one conversion in the 41 women undergoing conventional laparoscopic hysterectomy. There was no statistical difference in proportion of patients requiring adhesiolysis and in blood loss between the groups.
Strengths and limitations
Study limitations include the retrospective design and relatively limited number of patients. Strengths of the study include the fact that this was a single-surgeon experience (thus eliminating selection bias) and the fact that a standard minimally invasive approach was used for each group. No patients were excluded based on prior surgical history.
Interpretation
The proven benefits of the LESS approach include better cosmesis associated with the hidden umbilical scar and the elimination of any morbidity associated with the use of accessory ports.1–4,6 The anatomical rationale for performing surgery through the umbilicus is that it is the thinnest area on the anterior abdominal wall and contains few blood vessels and nerves. 9 This, theoretically, could lead to a lower risk of bleeding and to lower pain scores; however this approach could also impair wound healing, leading to an increased risk of postoperative herniation. However initial studies have suggested that this risk is low. 13 Future randomized studies with long-term follow-up can address these issues.
The average reported operative time for a LESS hysterectomy was consistent with the time provided by other researchers.2,3,5,7 However, two studies6,9 reported a mean operative time for LESS hysterectomy of 52.0 and 89.1 minutes, respectively, which is significantly shorter than the time in the current study and the times reported by other researchers. Regarding LESS, it was found that in the current study that operative times gradually decreased, when the first 19 LESS cases were compared to the last 18 LESS cases. More data are necessary to evaluate the learning curve associated with the LESS approach better.
In 14 (39%) cases of the LESS group at least one additional trocar was placed. Although this level is high, compared to what has been reported in the literature (5.9%–12%)6,7 the percentage in the current study represents the initial experience of a single surgeon with an unselected population. Once the first LESS hysterectomy was performed, every case that was deemed appropriate for a laparoscopic approach was initiated as a single incision case and included in the LESS study group. The current authors believe that, although this allowed, the single-surgeon gain significant initial experience with LESS, the learning curve associated with adoption of the LESS approach contributed significantly to the higher rate of additional trocar placement that was noted. Currently, the current authors' rate of additional trocar placement is <5%. The decision to place an additional port was based on patient-specific anatomical concerns (pelvic adhesive disease, uterine size, leiomyoma location). The most common reason was to obtain better access to the uterine vessels.
Some unexpected benefits of a single-incision approach were discovered during the performance of these surgeries. It was found that the LESS umbilical incision allowed for extracorporeal morcellation (Fig. 1). By applying traction on the uterine corpus and repeatedly incising the myometrium with a #15 scalpel, the fundus was morcellated easily by hand through the umbilicus. This approach eliminated the need for a morcellator, thereby enhancing the safety of the procedure and saving costs.
However the LESS approach approach does not eliminate a risk of dissemination of undiagnosed malignancy and should not be recommended as a procedure that does so. In light of recent discoveries regarding the risks of morcellation the current authors have modified the technique. The uterus is placed in an endobag, and the bag is exteriorized through the umbilicus. Morcellation is carried out as before, entirely within the bag, preventing any intra-abdominal dissemination of specimen fragments.
The LESS approach also appeared to decrease the operative time, particularly for patients with larger uteri. Notably, the operative times for C-LSH/TLH and LESS were similar, despite the significantly higher weights of the surgical specimens in the LESS group. This suggests that the LESS approach with transumbilical morcellation may be a more efficient form of minimally invasive hysterectomy. Starting a case with a LESS umbilical incision might be advantageous even if the uterus is large and additional trocars might be necessary.
One of the potential limitations of the LESS approach to hysterectomy is the difficulty in exposing the uterine vessels. The fact that all instruments are introduced from the umbilicus can make it difficult to gain access to the uterine artery and vein. With C-LSH/TLH the uterine vessels are ligated easily via the lateral ports. It was found that placing a single-tooth tenaculum to manipulate the uterus “from above” (Fig. 2), rather than placing a transcervical intrauterine manipulator, allowed for greater uterine mobility and created an angle appropriate for ligating the uterine vessels. As a result, the current authors abandoned the use of intrauterine manipulator quickly, thus providing additional cost savings. Problems with visualization can also be overcome with a flexible or angled laparoscope. In the current authors' opinion surgical innovation will continue to enable the adoption of LESS.
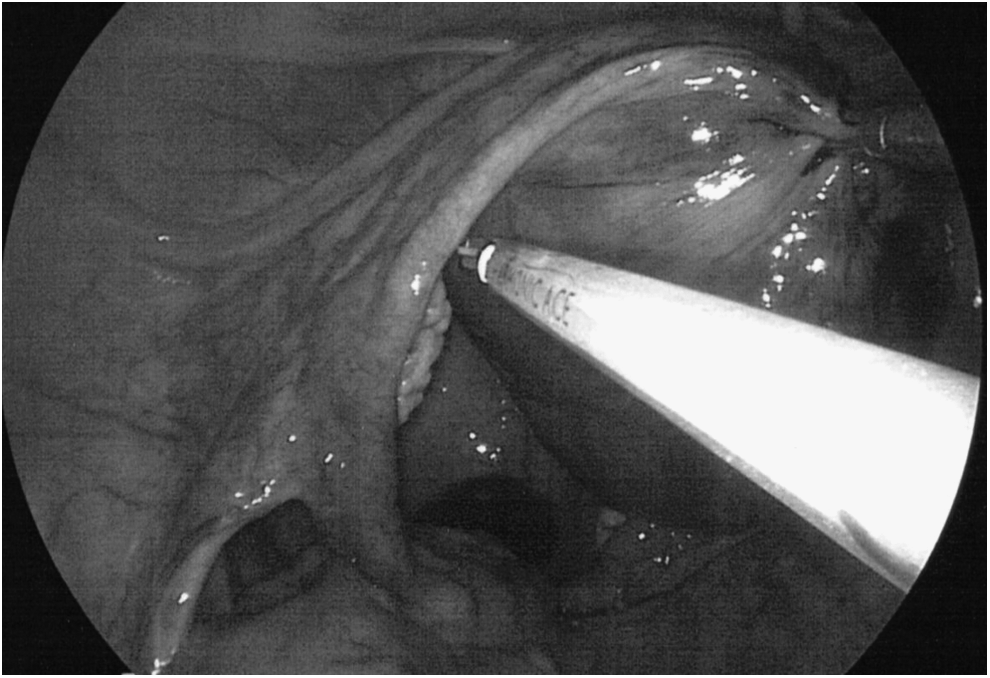
Angulation of the uterus. Angulation with a single-tooth tenaculum allows exposure of the lower uterine segment and access to the vessels.
The current authors have used this technique for 5 years with senior residents as first assistants. It has been found that these residents incorporate LESS into their practices upon graduation.
Conclusions
The data from this study suggests that conversion to the universal LESS approach for minimally invasive hysterectomies is certainly feasible. In addition, the larger umbilical incision has several advantages. It allows for extracorporeal morcellation, which shortens operative time, enhances patient safety, and might allow for easier removal of larger uteri. Eliminating the need for a morcellator and a uterine manipulator also decreases the cost of hysterectomy using the LESS approach. Although future studies on this technique are necessary, LESS may represent a more cosmetic, more cost-effective, and more efficient alternative to multiport laparoscopic hysterectomy.
Footnotes
Acknowledgments
The authors extend thanks to Howard Minkoff, MD (SUNY Downstate, Maimonides Medical Center) for reviewing an article and providing valuable critical comments. No funding and no compensation were provided.
Disclosure Statement
The authors report no conflicts of interest.