
Abstract
Abstract
Introduction
D
In Western countries the incidence of diverticular disease is 10% until age 40, 30% for the ages of 60–70, and 70% for patients older than 75. 2 The majority of patients with diverticulosis are asymptomatic. Yet, 20% of these patients will develop symptoms; while, among patients who develop diverticulitis, only 25% will present with complications, such as obstruction, perforation, stricture, abscess, or fistula. 3
Colo-vaginal fistulas are considered to be an uncommon phenomenon that is difficult to diagnose and treat; in addition, symptoms can even be embarrassing for patients, who are usually elderly women who have undergone total hysterectomy.4–8
Case
A 69-year-old female patient was referred by a gynecologist to the surgical ambulatory of the current authors' department because she had a malodorant fecal discharge from her vagina and a possible diagnosis of colo-vaginal fistula.
According to this patient's medical history, she had diverticular disease and had recurrent episodes of abdominal pain, for which she used an oral medication at home. Only one previous hospitalization for acute diverticulitis was recorded in her history. Notably, also in her history was the fact that she had undergone total hysterectomy.
This patient was admitted to the hospital and underwent complete laboratory tests and computed tomography (CT) of her abdomen. A full blood count revealed a white blood cell count of 9.550/μL; a hematocrit of 32.40%; a hemoglobin level of 9.95 g/dL; and a platelet count of 253.000/μL. In the coagulation tests, her prothrombin time was 12.2 seconds and her international normalized ratio was 1.07. Biochemistry test results were normal, while urinalysis, obtained after bladder catheterization, revealed no pathologic findings. CT scanning of the upper and lower abdomen and of the retroperitoneal space revealed diverticulaes of the descending and sigmoid colon and the presence of a colo-vaginal fistula, without signs of intra-abdominal inflammation (Figs. 1 and 2).

Sigmoid in close contact with the cuff of the uterus.
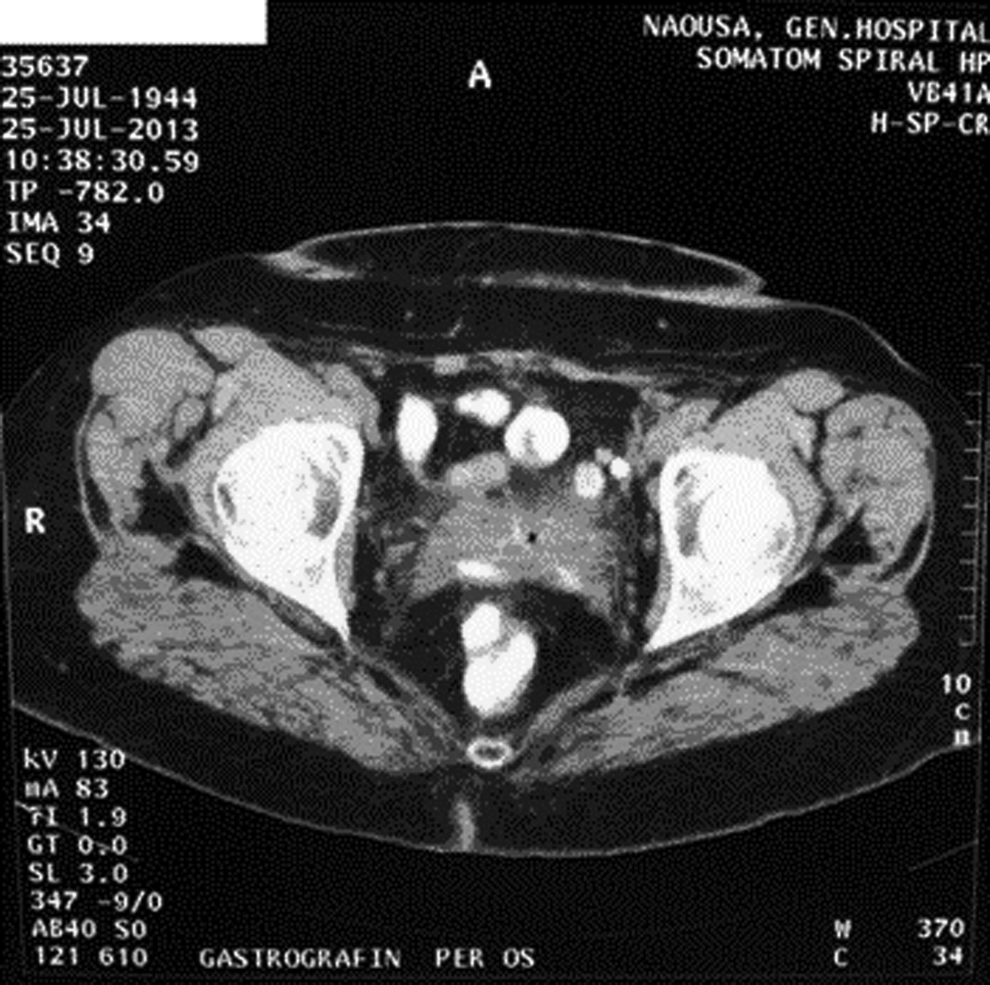
Linear formation with high densities in the wall of the uterine cuff—communication with the sigmoid
In the context of the differential diagnosis, the patient underwent a colonoscopy, which revealed the presence of diverticulaes in the entire length of the colon, especially in the descending and in the sigmoid colon without any pathologic lesions.
Because this patient's disease was benign and the absence of emergency conditions, she was released from the hospital and was scheduled for surgical intervention 6 weeks later. During this waiting period, she was prescribed antibiotic prophylaxis and instructed to maintain a low-fiber diet. She was also followed on an outpatient basis.
The surgical operation was performed as scheduled. It included one-stage removal of the sigmoid colon and the primary anastomosis (Fig. 3). The vaginal opening of the fistula was sutured.

Surgical specimen of sigmoid colon. The catheter with the rounded head indicates part of the fistula.
Results
This patient's postoperative course was uneventful and she was discharged from hospital on the eighth postoperative day. At a 1-year follow-up, the patient was noted to be free of symptoms.
Discussion
Colo-vaginal fistulas are a relatively uncommon complication of chronic and recurrent diverticulitis.9,10 Until March 1988, only 70 cases had been described worldwide.
In particular, formation of fistulas as a complication occurs in only 2% of cases, and, of these, only 20% involve communication between the colon and vagina.11,12 According to the mechanism described by Whiteway and Morson, 13 inflammation that persists at the vaginal cuff after hysterectomy creates adhesions to the proximal sigmoid colon. Adhesions combined with repeated episodes of diverticulitis in this region of the colon, lead to formation of a colo-vaginal fistula.
Another theory interprets fistula formation as a result of inflammation or even an abscess in the area of the sigmoid colon resulting in adhesions with the cuff of the vagina. 14
Patients, who, in most cases, are elderly women having undergone hysterectomies, visit their doctors with symptoms that affect social life and cause embarrassment. According to studies conducted by the Cleveland Clinic 15 and Reeves et al., 6 the main symptoms are malodorant fluid excretion from the vagina, flatulence, stools coming out of the vagina, possibly blood, and abdominal pain mainly on the left lateral ventricle and fever.
However, Colcock suggests that patients with recurrent diverticular disease who have previously undergone hysterectomy do not show other symptoms beyond persistent shedding of brown malodorant discharge from their vaginas. 16
Diagnosis of colo-vaginal fistula is a challenge and can escape physician's attention. Barium enema endoscopy primarily (mainly sigmoidoscopy), intravaginal ultrasound testing, colposcopy using a Foley catheter as had been described by Adachi and Gold, 17 magnetic resonance imaging, and CT scans are useful tools that—combined with clinical suspicion—can help in the diagnosis of colo-vaginal fistulas.5,18,19
It is worth noting, that the first two methods—namely barium enema and sigmoidoscopy—cannot be applied in cases of acute diverticular disease. 19
With respect to differential diagnosis, physicians should be aware of other causes of colo-vaginal fistulas, such as trauma and sexual assault 20 ; idiopathic bowel diseases 21 particularly Crohn's disease 22 ; or malignancies, such as cancer, localized in the colon, urethra, cervix or vagina. Moreover, colo-vaginal fistulas can be secondary to radiation therapy for malignant diseases of this area, 23 after surgeries on the colon or vagina, 24 and after bacterial infections in immunosuppressed (HIV) patients and rarely in tuberculosis.25–27
Treatment is exclusively surgical and includes very good preparation with antibiotics to prevent infections and inflammations up to 3–6 months before the surgery, given that physical symptoms are not particularly persistent and the patient's condition permits that approach.24,27 Three methods of surgical restoration of colo-vaginal fistulas have been described. The first and most widespread is the excision of the diseased portion of the bowel with the primary anastomosis. The vaginal opening of the fistula can be closed with simple sutures or left open without complications. 28 Another method of treatment is Hartmann's procedure.24,27 Finally, colo-vaginal fistulas can be restored performing the surgery in three steps; although, all the studies have shown that this method is superior to the others and efforts were made to reduce the number of restoration steps. 28
According to large studies conducted by Woods et al. from 1960 to 1986, 15 Vasilevsky et al. from 1975 to 1995, 28 and Hjern et al. from 1992 from 2004, 9 resection of the diseased portion of the bowel and primary anastomosis is the treatment of choice because this approach has shown to produce statistically nonsignificant morbidity, and mortality and complication rates with this technique is very low.
The current patient was a 69-year-old female, with a malodorant vaginal discharge and no other associated symptoms. She had a history of a total hysterectomy and repeated episodes of diverticulitis. Following imaging and endoscopic testing, she was diagnosed with a colo-vaginal fistula. She received antibiotic therapy and subsequently underwent surgery, which consisted in removal of the sigmoid colon and primary anastomosis. The vaginal opening of the fistula was left open without complications. She had an uneventful postoperative course and at her 1-year follow-up, she was free of symptoms.
Conclusions
Colo-vaginal fistulas may not be very common complications in chronic and recurrent diverticulitis but should be suspected, especially in older women who have undergone hysterectomies. Although these fistulas are benign, treating them is imperative, because they can cause of infections and affect patients' quality of life. What is equally important is to differentiate these fistulas from other conditions—mainly malignancies—as the symptoms are nonspecific. Treatment is surgical, and the proposed method involves resection of the diseased portion of the colon and primary anastomosis. The vaginal opening of the fistula can be left open without complications.
Footnotes
Disclosure Statement
No competing financial interests exist