
Abstract
Abstract
Introduction
L
As laparoscopic procedures increase in number, the use of robotic-assisted laparoscopy continues to increase as well. With emerging robotic technology, new developments, such as the robotic endoscopic stapler, may continue to improve the efficiency with which the robot can be used. This instrument may prove to be beneficial, as there will be no need to convert from a robotic procedure to conventional laparoscopy or a need to utilize an assistant performing conventional laparoscopy through the assistant port.
Materials and Methods
The EndoWrist Stapler 45 (Intuitive Surgical, Sunnyvale, CA) was approved by the U.S. Food and Drug Administration in October of 2012 for use with the DaVinci Si System. This is a reusable, wristed, stapling instrument that delivers six rows of staples and has a blade that transects the tissue down the middle of the staple line (Fig. 1). 4 There are two single-use reloads available. The blue reload (shown in black and white in Fig. 1) is 3.5 mm in length and 1.5 mm in height with 66 total staples in 6 rows, and it is used predominantly in procedures involving the bowel. The green reload is 4.3 mm in length and 2.0 mm in height with 44 total staples in 4 rows, and it is used predominantly in procedures involving the omentum and adipose tissue. 4
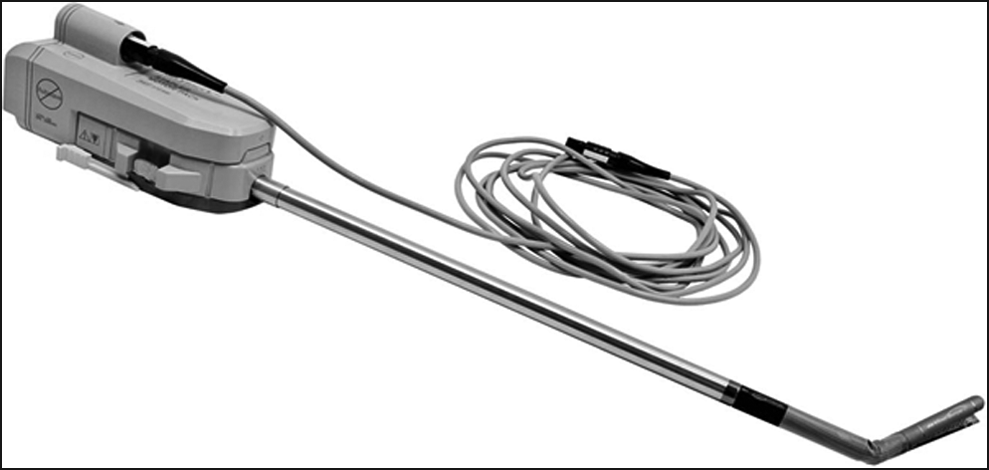
The Endowrist Stapler 45 is shown. The motor pack and power supply cord are connected. The jaw is shown open and articulating which can be used to ensure precise placement at the base of the appendix. Intuitive Surgical, Inc. Stock Photo: EndoWrist Stapler 45. Used with permission.
Ten patients from November 2013 to December 2013 underwent coincidental appendectomy at the time of robotic laparoscopy, during which the EndoWrist Stapler 45 with blue reloads was used. Surgical and pathologic outcomes were evaluated.
Informed consent for the surgical procedure was obtained from each patient at the time of that patient's preoperative visit. The decision to perform a coincidental appendectomy was made using the American Congress of Obstetricians and Gynecologists' current recommendations outlined in Committee Opinion Number 323 entitled “Elective Coincidental Appendectomy.” 2 If the patient fell into one of the groups with noted benefit, coincidental appendectomy was performed. Coincidental appendectomy was not performed if the patient a desire for had future childbearing.
In each of the cases, the gynecologic procedure was completed using three robotic arms. Robotic 8-mm ports were routinely placed in the umbilical site and right lower quadrant site. The left lower quadrant site utilized one of two options—the initial procedure was completed using a standard 8-mm robotic port with a subsequent change to a 13-mm port or a 13-mm port with a reducer was used.
If decision was made to perform an appendectomy, the mesoappendix and the mesoappendiceal vessels were dissected and secured using the harmonic scalpel. The stapler device was loaded with a blue reload, and the instrument was engaged on the robotic arm. The appendix was manipulated using the fenestrated bipolar to allow adequate visualization of the base. The stapler was then placed across the base of the appendix. The site of closure was inspected to ensure proper placement and to ensure that there was no unwanted tissue included in the jaw. The clamp sequence, followed by the firing sequence, was completed per the manufacturer's instructions. Once firing was complete, unclamping occurred automatically.
The appendix was maintained in the bipolar grasper while an Endocatch bag was introduced and then used for removal. Finally, the staple line along the appendiceal stump was carefully inspected for hemostasis.
Results
A total of 10 patients underwent coincidental appendectomy in which the EndoWrist Stapler 45 was used. All appendectomies were completed in conjunction with gynecologic surgery. There were 8 (80%) patients who underwent concomitant total robotic hysterectomy; 1 (10%) patient who underwent robotic supracervical hysterectomy; and 1 (10%) patient who underwent robotic operative laparoscopy. Primary indications for surgery included 6 (60%) patients with endometriosis, 3 (30%) with chronic pelvic pain, and 1 (10%) with chronic pelvic pain and fibroid growths.
Pathology was identified in 5 (50%) appendix specimens. Pathologic findings were: 2 (20%) fibrous obliteration, 1 (10%) endometriosis, 1 (10%) sessile polyp, and 1 (10%) focal, acute inflammation. No pathologic alteration was identified in 5 (50%) of the specimens.
No complications were identified. Intraoperatively, there were no cases of bleeding from the staple line or conversion to any other method, including conventional laparoscopy or laparotomy, to complete the procedures. There were no immediate postoperative complications encountered, including bleeding, infection, readmission, or reoperation. All patients were discharged within 24 hours of procedure completion. Patients were evaluated at 3- and 6 week post-operative visits, which are the standard follow-up visits requested by the primary surgeon, and no complications were identified.
Discussion
The benefit of coincidental appendectomy has been demonstrated in many patient subsets, especially those with endometriosis, endometriomas, and chronic pelvic pain. It is in these patients that the highest incidence of abnormal histopathology has been found.5,6 With the availability of a robotic stapler, coincidental appendectomy can be completed safely and efficiently by the console surgeon without conversion to standard laparoscopy.
With these benefits, appendectomy is a procedure that a general obstetrician–gynecologist may request privileges to perform. For surgeons who are immediately out of residency, privileges are granted based on verification of competency by the program director at the individual's institute of training. 7 If an already-practicing physician or a recently graduated physician was not trained but desires to perform appendectomies, privileges are granted per institutional standards. Generally, education about the procedure is completed, and an institutionally set number of proctored cases are completed with a surgeon who is experienced in performing appendectomies.
Conclusions
Preliminary cases of robotic-assisted laparoscopic coincidental appendectomies show that there are no intraoperative or postoperative complications, and the use of the robotic stapler may facilitate efficiency. Larger series of patients will be needed to determine the role of this new instrument better.
Footnotes
Disclosure Statement
Andrea Benton, MD, and Kristin Riley, MD, declare that they have no conflict of interest. Gerald Harkins, MD, is a surgical proctor for Intuitive Surgical and Ethicon.