
Abstract
Abstract
Introduction
A
MCTs comprise 10%–20% of all ovarian tumors and are more common in the premenopausal women, with a peak incidence in the third and fourth decade. The overall incidence of coincidental malignancy occurring within an MCT is 0.17%–2.0%. 3 However the incidence of malignancy within an MCT is reportedly higher in women beyond age 50.1,3,5,6
An MCT may be managed conservatively with imaging and serum tumor markers at intervals to avoid surgical morbidity. Coincidental malignancy in an MCT is a rare entity. Given the rarity, management is not standardized, but advanced stages of cancer associated with MCTs have a poor prognosis. The predictive value of age, preoperative imaging, and tumor markers were explored to determine if these help in diagnosing coincidental malignancy associated with MCTs in women age 50 and older. The article presents a retrospective review of 32 cases of MCTs treated at St. George's Healthcare NHS [National Health Service] Trust, in London, UK, over a period of 15 years, and provides a review of the literature. To the best of the current authors' knowledge, this is the largest retrospective review of women age 50 or older with MCTs.
Materials and Methods
This longitudinal retrospective review was conducted on all women age 50 or older with preoperative and final histologic diagnoses of MCTs, who were treated surgically. The patients were identified from the St. George's Healthcare NHS Trust pathology database. The search period was from 2000 to 2014. Inclusion criteria were: women age 50 years or older at the time of their surgery; surgery primarily for gynecologic indications; and histologically confirmed mature cystic teratoma. The local research and development department ratified the study proposal.
For patients who met the inclusion criteria, the electronic and hard-copy patient records were reviewed for demographic, clinical, radiologic, and pathology data, such as, age at surgical intervention, ethnicity, presenting symptoms, radiologic findings, preoperative serum tumor markers (CA-125, CA-19-9, and carcinoembryonic antigen), and mode of surgery. A consultant radiologist with a special interest in gynecologic imaging reviewed the preoperative radiology scans in all patients within the study. The risk of malignancy index (RMI) was calculated from the ultrasound (US) score and serum CA-125 values. 7 The incidence of coincidental malignancy was calculated for the study group.
A literature search was conducted on the Medline® and Embase databases, using the key words
Results
Demographic characteristics
Thirty-two women met the inclusion criteria for the study. The median age was 54, (range: ages 50–83) with 59% between ages 50 and 59. Of the 32 women, 53% were Caucasian, 19% were Afro-Caribbean, 15% were either Asian or mixed race, and 13% did not have ethnicity recorded.
Presenting symptoms
Abdominal pain was the presenting symptom of 18 (56%) women. In 14 (44%) women, MCT was an incidental finding while these patients were undergoing radiologic investigations for nongynecologic clinical problems.
Tumor markers
Preoperative serum tumor markers had been performed on 27 (84%) of the 32 women. Serum CA-125 only was measured in 7 patients, CA-19-9 only was evaluated in 1 patient, and both CA-125 and CA-19-9 were evaluated in 19 patients. CA-125 was within the normal range (0–35 U/mL) in 18 (92%) patients. CA-125 was elevated in 2 women—110 U/mL in a woman with a papillary thyroid cancer within an MCT and 183 U/mL in the second woman with histology of an MCT only. Of the other 2 cases with coincidental malignancy, CA-125 was 5 U/mL in 1 patient and tumor markers were not measured in the other patient as the diameter of the MCT was >5 cm and suspicion of malignancy was considered to be very low. Preoperative CA-19-9 ranged from <1 to 71 U/mL. CA-19-9 was within the normal range (0–37 U/mL) in 16 (85%) patients. The raised CA-19-9 values were 71 U/mL, 60 U/mL, and 43 U/mL, and none of these patients had coincidental malignancy.
Radiologic assessment
Computed tomography (CT) was performed in 10 women, transvaginal US in 8 women, magnetic resonance imaging (MRI) in 1 woman, and both CT and US in 13 women. In 9 (32%) patients, the ovarian tumors measured <5 cm; in 11(39.3%) patients, the ovarian tumors were between 5 and 10 cm; and in 8 (28.6%) patients the ovarian tumors measured >10 cm. In 30/32 (94%) patients, radiologic assessment revealed the presence of fat and/or calcifications within the ovarian tumors; the other 2 (6%) tumors appeared to be cystic with solid components. In 6/32 (19%) of the ovarian tumors, there were cystic areas with solid enhancing components with or without fat and calcifications. In 11 (34%) tumors, a fat-fluid level was identified within the tumor. The CT appearance of a mature cystic teratoma is illustrated in Figure 1. In the 3 patients with coincidental malignancies, the ovarian masses measured 11 cm in 2 patients and 2 cm in the third patient.

Computed tomography appearance of a mature cystic teratoma. In addition to cystic and solid components, the complex pelvic mass (short arrow) contained low-density fat and coarse calcifications typical of a mature cystic teratoma. The long arrow marks the bladder.
Risk of Malignancy Index
Risk of malignancy index (RMI) is calculated as CA-125 ×M × U. CA-125 is the actual value of the serum tumor marker measured in U/mL, and M is the menopausal status of the woman. The score is 3 if the patient is postmenopausal. U is the US score. The US characteristics taken into account are multilocularity, and evidence of solid areas, metastases, ascites, and bilateral lesions. The score is 0 if none of the features are present; the score is 1 if a single feature is present; and the score is 3 if two to five features are present. Women with an RMI of <25 have <3% risk of malignancy; those with an RMI of 25–250 have a 25% risk of malignancy; and those with an RMI >250 have a 75% risk of malignancy. 7
It was possible to calculate RMI in 17 patients. RMI was <25 in 3 (17.64%) patients, between 25 and 250 in 13 (76.47%) patients, and >250 in 2 (11.76%) patients. Of the 3 patients with coincidental malignancy, an RMI could be calculated in only 1—the RMI was 15 and the histologic assessment identified a carcinoid tumor within that patient's MCT.
Surgical management
The mode of surgery was laparotomy in 14 (43%) patients and laparoscopic in 18 (57%) patients. Unilateral salpingo-oophorectomy was performed in 5 patients, bilateral salpingo-oophorectomy was performed in 16 patients, and bilateral or unilateral salpingo-oophorectomy with hysterectomy was performed in 11 patients.
Frozen sections
Frozen section was performed on specimens from 10 women (31%) and confirmed mature cystic teratoma in each case. However, frozen sections were not performed on any of the specimens of women with coincidental malignancies.
Cases with coincidental malignancy
There were 29 cases of MCTs and 3 cases of MCTs with coincidental carcinomas, in which patients, surgery was performed, as imaging was suggestive of MCTs (Table 1). Figure 2 illustrates a typical MCT with a cyst lined by squamous epithelium, with underlying sebaceous glands and adipose tissue.
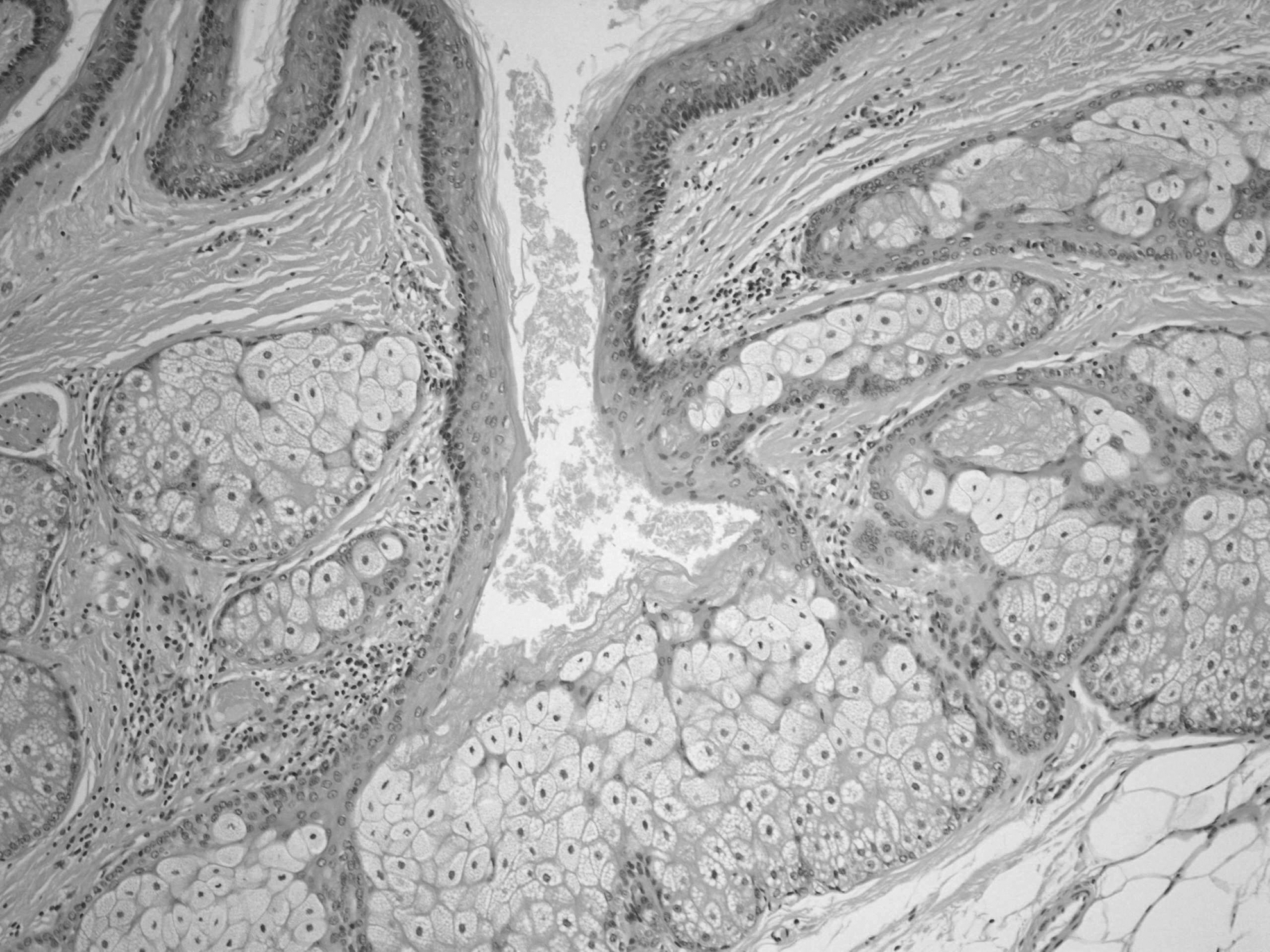
Histologic appearance of a mature cystic teratoma with hematoxylin and eosin stains (× 40 magnification).
Number of patients from total number.
MCT, mature cystic teratoma; CT, computed tomography, RIF, right iliac fossa; N/A, not available; MRI, magnetic resonance imaging; US, ultrasound, METS, metastases; DW, diffusion weighted; SCC, squamous-cell carcinoma; SCC-Ag, squamous-cell carcinoma antigen; CEA, carcinoembryonic antigen.
The first patient with coincidental malignancy was of 63 years of age and was being investigated for abdominal pain. US and CT scans showed an 11-cm ovarian cyst and features suggestive of an MCT. This patient's preoperative CA-125 was 5 U/mL, and her RMI was 45. She had had a previous right salpingo-oophorectomy and underwent a laparoscopic left salpingo-oophorectomy, as suspicion of malignancy was low. Histologic assessment revealed a carcinoid tumor of an insular type arising within the MCT; this was confirmed with immunohistochemical staining for the neuroendocrine markers chromogranin and synaptophysin (Fig. 3).

Histologic appearance of a carcinoid tumor within a mature cystic teratoma with chromogranin immunohistochemistry (× 100 magnification).
The second patient was age 53 and was being investigated for postmenopausal bleeding. A US scan showed an 11-cm complex ovarian cyst. This patient's CA-19-9 and CA-125 were 5 U/mL and 110 U/mL, respectively. An RMI could not be calculated, as the detailed findings of the US scan (performed at a referral hospital) were not available. The result of a CT scan, performed in view of a complex ovarian mass, was reported as an MCT. The patient underwent a laparotomy, involving total abdominal hysterectomy, bilateral salpingo-oophorectomy, omentectomy, and appendectomy. There was no suspicion of malignancy and a frozen section was not performed. Histologic assessment of the tumor showed a papillary carcinoma arising within a focus of struma ovarii in an MCT.
The third patient was 62 years' old and presented with postmenopausal bleeding. A US scan showed bilateral ovarian cysts measuring 2.5 cm on the right and 2 cm on the left, both reported as MCTs, and an endometrial thickness of <5mm. Serum tumor markers were not tested. This patient underwent a laparoscopic bilateral salpingo-oophorectomy. Histology testing showed an MCT on the right ovary and an adult granulosa-cell tumor on the left ovary, as confirmed with positive inhibin and vimentin immunostains. Although the imaging was suggestive of MCT, there was no histologic evidence of MCT in the left ovary.
Discussion
In the current study, 3/32 (9%) women age 50 or older had coincidental malignancy associated with MCTs. The common presentations for the study group were abdominal pain or incidental findings on imaging for other clinical indications. Tumor markers were not diagnostic for coincidental malignancy. Imaging could be used to diagnose MCT, but, in none of the 3 cases, did imaging suggest coincidental malignancy. The reported incidence of a coincidental malignancy within an MCT is reportedly rare with a range of 0.17–2.0. 3 Most MCTs with coincidental malignancy have cyst diameters of ≥10 cm; in 2 of the 3 cases in the current series, the cysts were >10 cm in diameter. The 2 cases were among the 8 patients with cysts larger than 10 cm.
The mean age of coincidental malignancy with MCT was 50.6 years in a study by Rim et al., 5 compared to 52.5 years in a study by Sakuma et al. 8 In the current study, the mean age was 55, although, unlike the previous two studies, the current patient cohort was selected for ages of 50 or older. In the current study, 53% of the patients were Caucasian; few studies describe ethnicity in patients with MCTs. In postmenopausal women, the majority of MCTs are found incidentally or following investigations for nonspecific abdominal pain, as in the current series.1,9–13
An MCT of the ovary has a distinct radiologic appearance characterized by the presence of calcification, fat, and fluid, and these features are the same irrespective of age. Tan et al. concluded that US is a reliable tool for diagnosing an MCT. 14 Currently, imaging can be used to predict the presence of an MCT, but early malignant changes can be subtle and difficult to detect. Takagi et al., demonstrated that fat-suppression MRI has a high sensitivity for identifying somatic malignancies within an MCT 15 ; however, the methodology needs further evaluation. The fat-suppression MRI has been incorporated in the European Society of Urogenital Radiology (ESUR) guidelines for indeterminate adnexal masses to confirm an MCT, but the technique does not necessarily identify somatic malignancy. 16 Dos Santos et al. 17 and others13,18–21 have suggested that cysts of ≥10 cm are likely to have carcinomas arising within them.
In the current series, 2 patients with coincidental malignancy had MCTs measuring 11 cm, and 6 other patients had MCTs of ≥10 cm in diameter. In addition, in patients age 50 or older, 25% of those with MCTs of >10 cm had coincidental malignancy.
Park et al. observed that malignancy within an MCT could be characterized via a CT scan showing nodular formation within the cyst, enhancing the soft-tissue component, and showing an obtuse angle between the soft tissue and the inner wall of the cyst. These researchers detected a statistically significant difference (p < 0.5) using these characteristics to differentiate between a benign MCT and a malignancy within an MCT. 20 A study by Namimoto et al. included the addition of diffusion-weighted (DW) imaging, an emerging technique that has enhanced MRI, enabling better differentiation of benign and malignant lesions in some pathology. 22 However, the utility of DW imaging may be more limited for detecting ovarian pathology.
In the current study, neither preoperative serum tumor markers nor the RMI were helpful for planning surgical management, as suspicion of coincidental malignancy was not suggested. However, not all patients in this series had preoperative serum tumor-marker testing and MRI. There is currently no specific commercially available serum tumor marker in clinical use that reliably distinguishes an MCT from an MCT harboring a somatic malignancy.
A report suggested that elevated serum squamous-cell carcinoma antigen (SCC-Ag) in women with dermoid cysts may indicate squamous-cell carcinoma arising with MCTs. 5 However, none of the tumor markers have been found to be diagnostic for predicting malignancy or correlating with stage of disease, although high levels of SCC-Ag and CA-125 may indicate a worse outcome. 3 Squamous-cell carcinoma is reported to be the most common (> 80%) form of tumor arising within an MCT. 3 Other malignancies described are carcinoid tumors, adenocarcinomas, carcinosarcomas, melanomas, and neuroectodermal tumors.3,23,24 In the current series, the 3 coincidental malignancies had different histologies. Of these, 2 could be considered malignant transformation with somatic malignancies (a papillary carcinoma arising in struma ovarii and a carcinoid tumor), while the third was a synchronous sex-cord stromal tumor (adult granulosa-cell tumor) in the contralateral ovary.
If an MCT is diagnosed on imaging in a woman over age 50, conservative management may be an option. 25 In elderly women or women with poor American Society of Anesthesiologists (ASA) scores, conservative management can avoid surgical and anesthetic morbidity. However, a coincidental malignancy within an MCT may progress to an advanced stage. 26 In a study by Seltzer and Vogel, 2-year disease-free survival for stages I and II was 100%, while the survival was 30% for stage III and 0% for stage IV. 27 Although there is only anecdotal evidence, an MCT with a secondary malignancy may sometimes present with rupture, resulting in an acute abdomen and the need for an emergency surgery.28,29
For an MCT with coincidental malignancy, appropriate surgical cytoreduction improves the patient's outcome. 21 There is no standardized chemotherapy regimen for adjuvant treatment, as there is a wide range of histology types in coincidental malignancies. In a systematic review by Hackenthal et al., alkylating agents are associated with a better outcome than all other chemotherapeutic agents used to treat MCTs with coincidental malignancy. 3
The strength of the current study is the focus on women age 50 or older with preoperative diagnoses of MCTs, with the case review performed before surgical intervention and specialist involvements (radiology and pathology). However, the current study did have shortcomings. This was a retrospective study, there was variation in preoperative imaging modalities, and MRI was not used extensively. CT was performed for large MCTs to estimate disease spread, like any other complex ovarian mass. Finally, not all patients had the same serum tumor markers estimated and the same radiologic investigations.
To the best of the current authors' knowledge, this is the largest study of MCT in this specific age group, with a total of 32 patients. There have been previous smaller studies in postmenopausal women reporting a higher incidence of coincidental malignancy in MCT. In a study by Wei et al., 3 of 20 postmenopausal women with MCTs had coincidental malignancy, with an incidence of 15%. Two patients received adjuvant treatment. Stage at presentation was not mentioned and follow-up was not described. 6 In a study by Gordon et al., 16 of 309 women were postmenopausal and 3 of the 16 postmenopausal women (18.75%) had coincidental malignancy. 2 The researchers concluded that an MCT warrants staging surgery in postmenopausal women owing to the high incidence of coincidental malignancies in this age group. Despite the differences in the incidences, the common recommendation is a surgical intervention in women over 50 years of age with MCTs. The outcomes of all cases of Stage 1 MCT with coincidental malignancy in postmenopausal women in the current literature are summarized in Table 2.
MCT, mature cystic teratoma; RMI, risk of malignancy index; US, ultrasound, CT, computed tomography, TAH, total abdominal hysterectomy; BSO, bilateral salpingo-oophorectomy; R, right; L, left; N/A, not applicable.
Conclusions
There is currently no tool that is diagnostic for predicting coincidental malignancy in an MCT preoperatively; hence it remains a postoperative histologic diagnosis. In the current study, the incidence of a coincidental malignancy, including somatic and synchronous ovarian malignancy associated with MCT, in women age 50 or older with preoperative diagnoses of MCT was 9%. Furthermore, the likelihood of a coincidental malignancy was 25% if the MCT was >10 cm in diameter. In this respect, the mode of surgery, whether a laparoscopic or open approach is used, to deliver the specimen should also be carefully considered. The current authors therefore recommend that surgery should be strongly considered in women older than age 50 who have radiologic suggestion of MCT, and both ovaries and fallopian tubes should be removed.
Footnotes
Author Disclosure Statement
No financial conflicts of interest exist.