
Abstract
Abstract
Introduction
V
Latzko repair is one such transvaginal, reconstructive surgical method, first described in 1914, which lost its status even among gynecologists. 3 It is a minimally invasive surgery with short operative time, a small learning curve, minimal blood loss, low postoperative morbidity, ashort convalescence period, and a high success rate. With the advent of more sophisticated surgeries, these simple transvaginal surgeries have had a downturn. Given that the current authors find this simpler vaginal approach of Latzko repair still relevant today, this article reports their experience with the Latzko operation over the last 1½ years.
Materials and Methods
Patients and methods
Eight patients with posthysterectomy vault VVF had repairs using the Latzko operation. The surgeries were performed from November 2013 to May 2015 in the gynecology department of the current authors' center (the University College of Medical Sciences and Guru Tegh Bahadur Hospital, in Shadhara, New Delhi), a tertiary-care hospital of Northern India. Each woman had a preoperative evaluation comprised of a history along with general, abdominal, and genital examinations to assess accessibility to fistula repair, tissue quality, and mobility. Cystoscopic evaluation was performed to visualize the fistula and to determine the number, location, and proximity to ureteric orifices in each patient. Examination findings, surgical details, and available follow-ups were recorded. This is a descriptive case series of 8 patients who underwent Latzko repair. A retrospective analysis was performed of these patients' data by evaluating the available records.
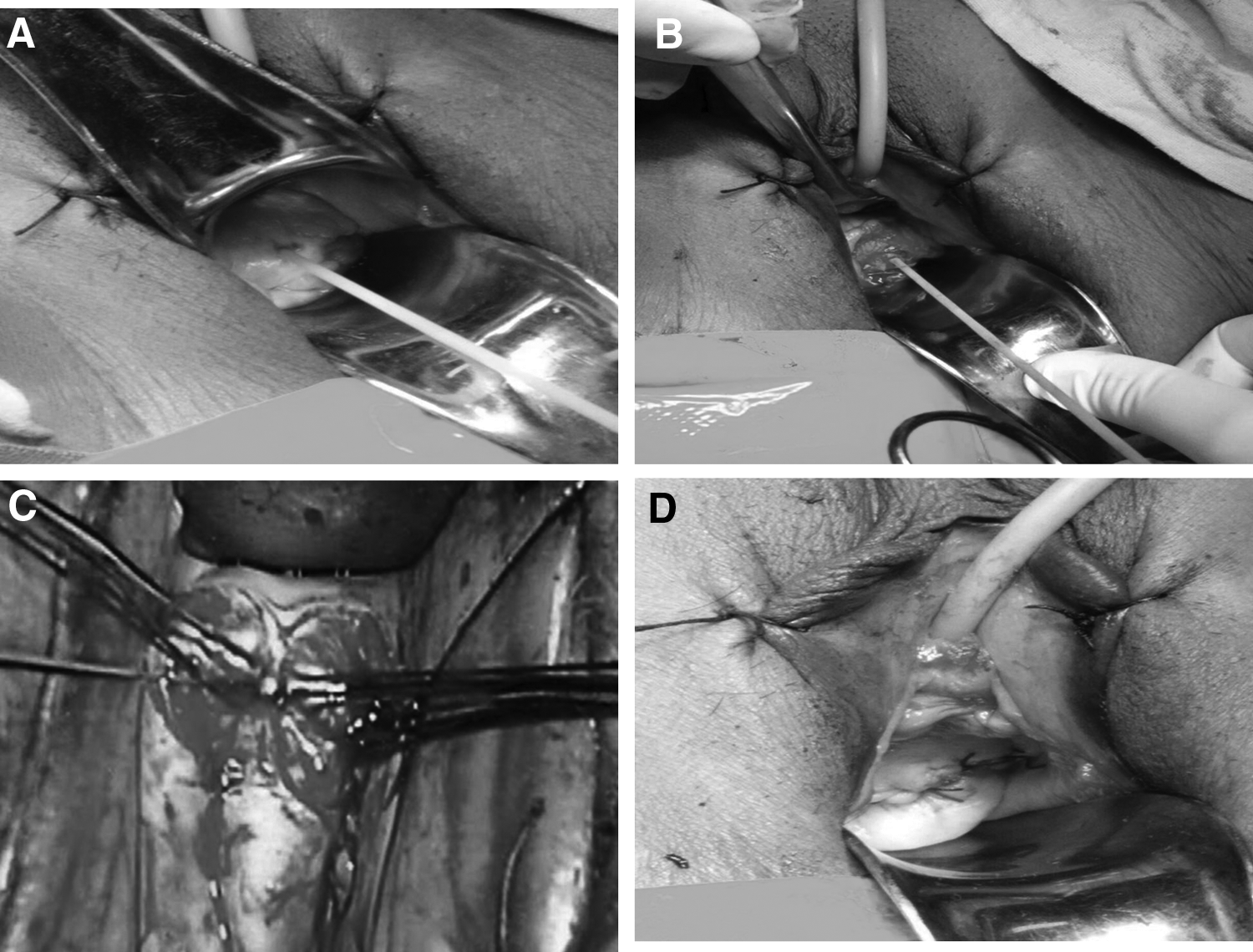
Surgical steps
After providing two sterile urine-culture specimens, each patient underwent Latzko repair. The patient was placed in the lithotomy position. A Foley catheter was placed in the fistula opening, and the bulb was inflated within the bladder lumen (Fig. 1A). This allowed the fistula to be drawn downward to make it more accessible. The fistula was then circumcised at a distance of 1.5–2 cm from the fistulous opening (Fig. 1B). The circumcised area was removed up to the edge of the fistula opening. The anterior and posterior vaginal walls, which had been denuded of the epithelial layer, were approximated with interrupted absorbable sutures (3-0 vicryl). This first layer was further imbricated and strengthened by a second layer of interrupted suture (2-0 vicryl). No sutures were placed within the bladder (Fig. 1C). A third layer of interrupted sutures were used to close the vaginal mucosa (Fig. 1D). Water seal was checked by instillation of dye. The bladder was drained with a Foley catheter for ∼14 days. Success of the procedure was defined as the absence of urinary incontinence after the removal of the catheter.
Results
The characteristics of the 8 women who underwent Latzko repair are given in Table 1. The mean age of the patients was 41.7 years (range: 25–60 years). Four (50%) patients were perimenopausal. In 6 patients (75%), fistula formation occurred following abdominal hysterectomy. One of these patients had underwent a previous Cesarean section; her bladder was injured and repaired during hysterectomy. The fistula developed despite urethral drainage for 14 days. Two patients developed fistulae after vaginal hysterectomy. All of the hysterectomies were for benign indications.
SD, standard deviation, b/w, between.
The mean duration between initial surgery and incontinence was 11 days (range: 3–30 days). Six patients (75%) presented with urinary incontinence within 10 days of index surgery. One patient did not leak until 15 days after primary surgery. In this patient, the fistula was not visible on speculum examination, but a small 2-mm fistula was evident on cystoscopy. Another patient developed fistula symptoms after 30 days of hysterectomy.
All fistulas were simple, ≤1cm in diameter, and supratrigonal in location. The mean size of the fistulas was 5 mm (range: 2–10 mm). One patient (12.5%) was referred to the current authors after a previous failed repair of her VVF. A vaginal approach for repair was used, which was not specified further. In this patient, two 5 mm fistulas were seen on cystoscopy. All patients were catheterized for a minimum of 12 weeks following the diagnosis of fistula after primary surgery (i.e., hysterectomy). By this time, tissue condition becomes ideal for optimal surgical cure. The mean duration between fistula diagnosis and Latzko repair was 37 months (range: 4–96 months). Two of the 8 patients (25%) had repair after 4 months of incontinence. Three (37.5%) patients did not request surgical treatment until 7–8 years posthysterectomy.
Surgical details and follow-up for the Latzko procedure are given in Table 2. The mean operative duration was 60 minutes (range: 45–90 minutes). Surgery was performed by the same surgeon (A.S.) or under her supervision. The longest surgery was performed in 90 minutes. No intraoperative complications were noted. No leakage was observed on a dye test performed immediately after Latzko repair. The sole postoperative complication was a urinary-tract infection (UTI) in 1 patient, which was treated with oral antibiotics. The mean postoperative hospital stay was 2 weeks (range: 8–17 weeks) although patients who undergo this procedure can be discharged on day 5. As these patients came from distant places to the tertiary-care center, these patients did not want to be discharged before removal of the catheter. All patients were able to void postoperatively after the removal of the catheter (100% success rate).
SD, standard deviation.
Two patients were followed up for 8 and 6 months. No recurrence was noted in them. These 2 patients resumed normal vaginal intercourse after 8 weeks of abstinence, which had been advised. Six patients were followed up for 3–4 months and had no complaints of leakage. However, they had not resumed sexual activity according to their personal preferences. Table 3 compares the results of this current study with those of previous published reports on Latzko repair. The success rate of the Latzko operation in the current series was similar (100%) to others (92%–100%).
Everett HS, Mattingly RF. Vesicovaginal fistula. Am J Obstet Gynecol 1956;72:712.
Falk HC, Kurman M. Repair of vesicovaginal fistula. Review of 140 cases. J Urol 1963;89:226.
Rader ES. Post-hysterectomy vesicovaginal fistula: treatment by partial colpocleisis. J Urol 1975;114:389.
Ansquer Y, Mellier G, Santulli P et al. Latzko operation for vault vesicovaginal fistula. Acta Obstet Gynecol Scand 2006;85:1248.
Discussion
VVF, if diagnosed immediately after surgery, may be treated conservatively by prolonged catheterization. VVF may be repaired by transvaginal, transabdominal, or laparoscopic approaches, depending upon characteristics of the fistula and the surgeon's preferences. The best approach is the one in which the surgeon is most experienced. Surgeons favor the transabdominal approach for fistulas that are multiple, recurrent, in close proximity to ureteric orifices. The abdominal approach has a reproducible and durable success rate of 94%–100%. 4 However, morbidity associated with the abdominal technique has led to urologists preferring a laparoscopic approach over the last 3 decades. It is a minimally invasive procedure with benefits of immense magnification, reduced need for analgesia, shorter hospital stay, quicker recovery, and better cosmesis. But technical complexity, a steep learning curve, and difficult suturing pose major limitations to use of the laparoscopic approach.
Subsequently, there has been the development of robotic assistance for the laparoscopic approach, which improves coordination, and makes dissection and suturing much simpler. However, the cost of procuring a robotic system is a major hindrance to its routine application.
With the advent of these newer technologies, vaginal surgeries do not figure in the armamentarium of urologists. But the vaginal approach uses a true natural orifice—a scarless approach. It avoids the need for laparotomy, and has shorter recovery, minimal blood loss, low postoperative bladder irritability, and zero operative complications such as trocar-induced bowel and vessel injuries. Results are comparable to those of the abdominal approach. Thus, the vaginal route is favored by gynaecologists.
The success of the procedure is attributable to the fact that the anterior and posterior vaginal walls are in contact with one another; so, when the epithelium around a fistula is removed, the resulting raw surfaces of the two walls can be approximated without tension, caused by the distensibility of vaginal walls. 5 Fistulas of any size, with good tissue quality and supratrigonally located are ideal fistulas for Latzko repair. Even fistulas in proximity to ureters can be repaired. However, evaluation for ureteric reimplantation is necessary, if the fistula margin is <5 mm from the ureter. This procedure has a short learning curve.
The fistula sizes ranged in the current series from 2 mm to 10 mm. Compared to a transvesical repair, the Latzko procedure offers the advantage that it does not narrow the bladder and thus does not jeopardize the ureters, even with large fistulas. Tancer, however, reported a patient with a grade 2 hydroureter diagnosed 16 weeks after a Latzko procedure; this hydroureter was managed successfully with a retrograde stent for 6 weeks. 6 Fewer complications, however, have yet been reported after Latzko's procedure. In his pioneering publication, Latzko reported bladder lithiasis in 2 patients. 5 In the current series, the only postoperative complication noted was a UTI in 1 patient, which was managed by single course of antibiotics.
In 1 of the patients in the current series, there was a prior failed surgical attempt of VVF repair vaginally. Latzko repair was attempted and de-epithelialization was carried out on the left side of the vaginal vault and centered on the persistent fistula. This second attempt was successful. Similarly, Tancer reported 9 initial failures among 107 first Latzko attempts, which were all successfully managed by a repeat Latzko operation. 6 Kaser observed 3 failures among 38 patients, of which 2 were cured with a second Latzko and 1 was cured after a third Latzko procedure. 7 This shows that past history of Latzko repair is not a contraindication and does not preclude the success of the subsequent Latzko operation.
Conclusions
The key points of successful Latzko repair are correct plane of dissection, appropriate removal of scar tissue, adequate vascularity, avoiding tension on the suture line and the imbricating suture line. Double catheterization (i.e., urethral and suprapubic catheterization) is not necessary. The limitations of this study were its retrospective study design, small sample size because of the rarity of this event, lack of long-term follow-up, and heterogeneity of inclusive fistula characteristics. Long term follow-up of these women with Latzko repair is required. However, Latzko repair is a simple, purely transvaginal technique for managing posthysterectomy vault VVF. The current results confirm this repair's efficacy and safety. The current authors' message to gynecologic surgeons is: “Don't cede your ground to urologists; fistulas are our domain. Go gynecologists, and recapture your domain!”
Footnotes
Acknowledgment
The authors acknowledge Dr. Richa Sharma, associate professor, Department of Obstetrics and Gynaecology, University College of Medical Sciences and Guru Tegh Bahadur Hospital, Delhi, India for her support in collecting the data.
Author Disclosure Statement
The authors, Abha Sharma, Nilanchali Singh, Amita Suneja, Yashika Motwani and Kiran Guleria, share no actual or potential conflicts of interest.