
Abstract
Abstract
Introduction
C
Case
A multiparous woman in her mid-40s, with multiple medical comorbidities including a body mass index of 48, was referred to the gynecologic oncology service of the Rutgers–New Jersey Medical School, for an adenocarcinoma that was identified on routine cervical cytology. The cytology was human papilloma virus 16/18–negative, raising a concern that this patient might have a primary endometrial rather than a cervical carcinoma. Her gynecologic history was significant for irregular menses, and there was no known family history of malignancies.
On examination, a 3.0-cm exophytic lesion was seen replacing the cervix. An office cervical biopsy showed a carcinosarcoma of endometrial versus cervical origin. A p16 immunostain was positive, and her carcinoembryonic antigen was focally positive, favoring a cervical primary lesion, and the tumor stained for AE1/3, epithelial membrane antigen, and CK7, and focally for vimentin in spindle-cell areas. Chromogranin and synaptophysin testing yielded negative results. This patient was unable to tolerate endometrial sampling to determine the origin of this malignancy better. She underwent a positron emission tomography scan, which revealed heterogeneous uptake in the mid- and left-endocervix with no uptake in the uterus and no evidence of metastatic disease.
The patient underwent a robotic-assisted radical hysterectomy and pelvic lymph node dissection for stage IB1 cervical carcinosarcoma.
Results
This patient's postoperative course was complicated by ileus, which resolved spontaneously.
Pathology
Gross examination showed an exophytic cervical lesion (Fig. 1). Histologic evaluation showed a carcinosarcoma of the cervix (2.0 × 1.0 cm in the greatest dimension) with <1 mm invasion. The tumor was biphasic, with focal chondroid differentiation (Fig. 2). The epithelial areas stained for CK 5/6, p63, and p40 with some lesser staining of the spindle areas, which, in turn, were strongly positive for vimentin (Fig 3). No lymphovascular invasion was noted. Additional findings included weakly proliferative endometrium, an endometrial polyp, adenomyosis, and unremarkable bilateral fallopian tubes and ovaries. The lymph nodes were negative.
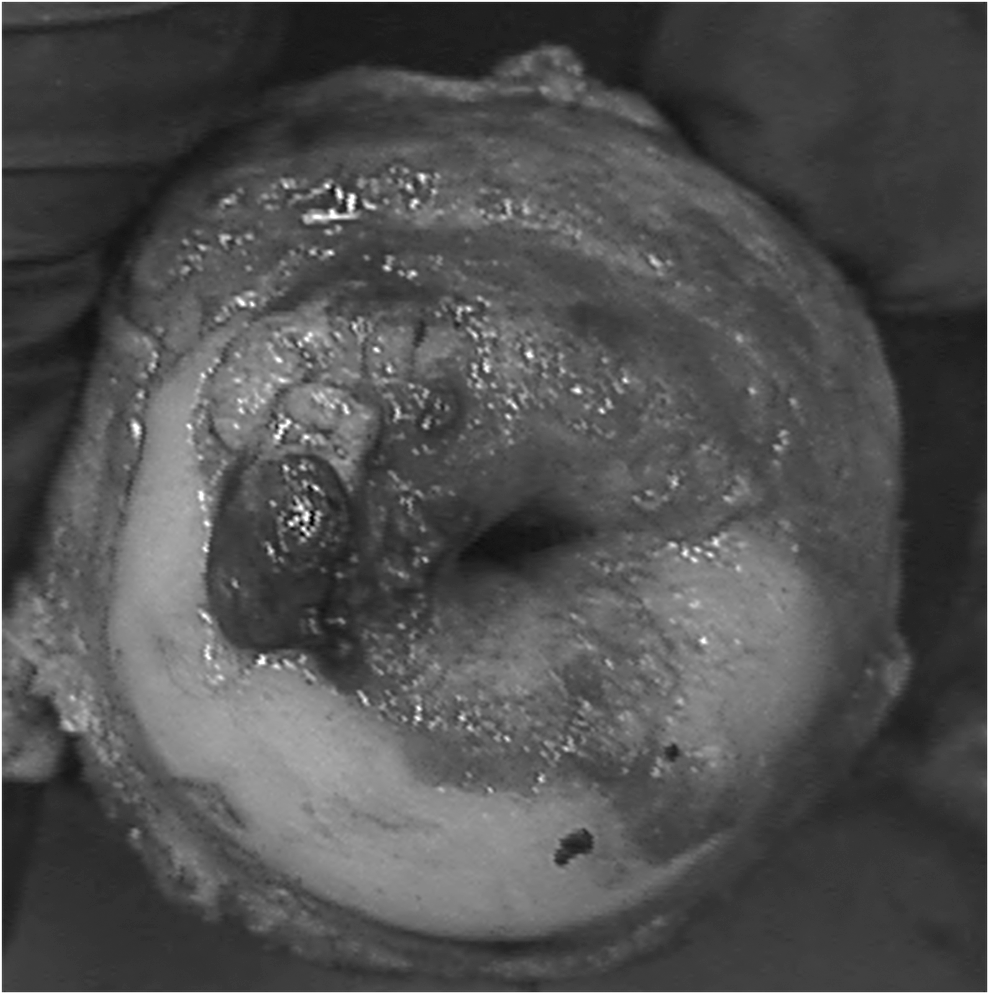
Radical hysterectomy specimen shows exophytic lesion.
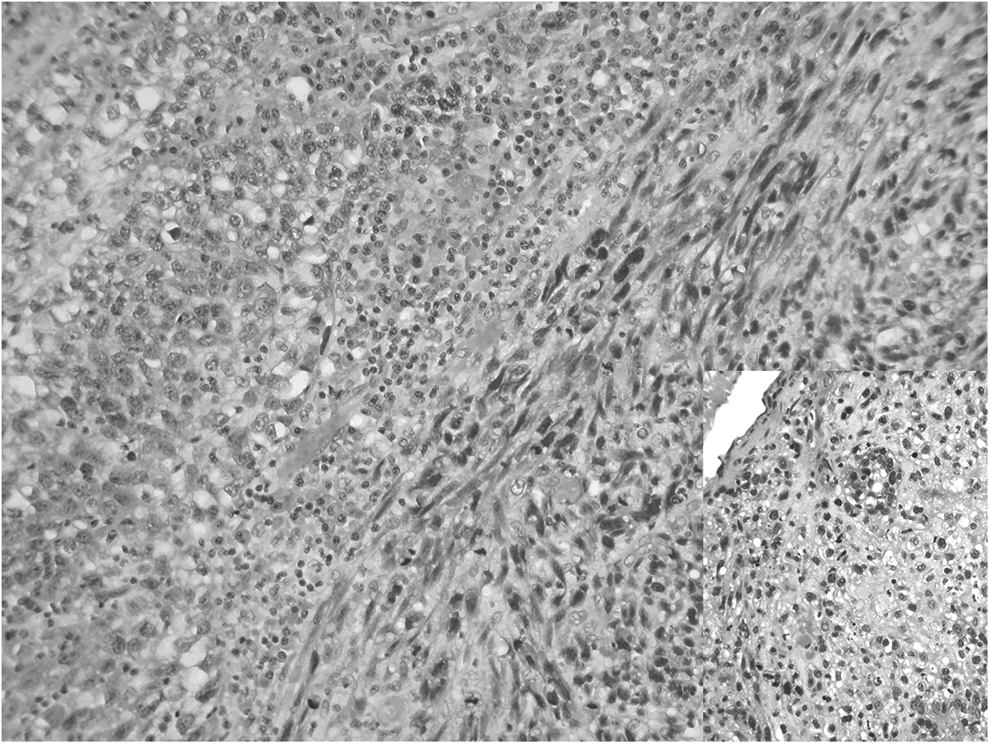
The biphasic tumor showed epithelioid and spindle-cell areas, with focal chondroid differentiation (inset, lower right).
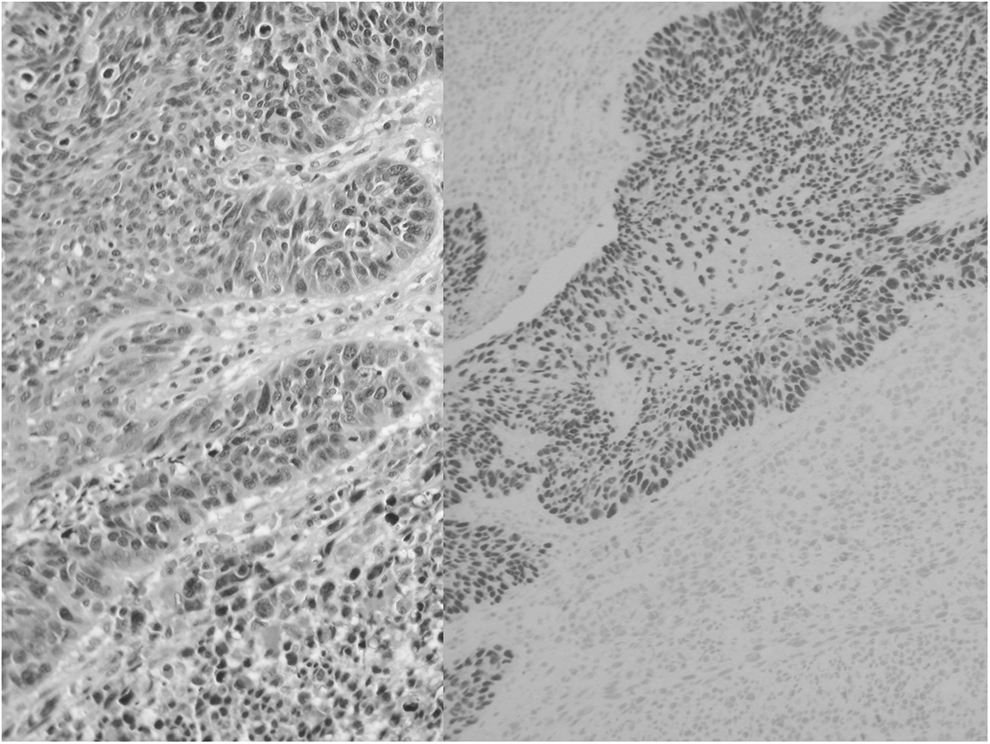
P40 stained the epithelial component (right) but not the mesenchymal component of the tumor.
Discussion
Carcinosarcoma of the uterine cervix is extremely rare. There were ∼35 reported cases as of 2008, representing <0.5% of cervical cancers. 2 Reported cases have occurred in predominantly postmenopausal women, with a median age at diagnosis between 62 and 69 and an age range of 12–87. 2 The most common presenting symptom is vaginal bleeding and usually a detectable exophytic mass is seen on the cervix. 3 Other symptoms can include pain, passage of tissue, or a palpable mass. 2 A cervical smear can yield abnormal results. Because of histologic similarity, the differential diagnosis includes sarcomatoid carcinoma. The principal characteristic feature of a carcinosarcoma is the mixture of carcinomatous and sarcomatous components that remain distinct from each other, whereas, in sarcomatoid carcinoma, both components have a tendency to merge. Both neoplasms are thought to be the result of metaplastic carcinoma and might indeed be part of the same spectrum. 4
Conclusions
Uterine carcinosarcoma with spread to the cervix needs to be ruled out in cases of cervical involvement. In addition to the positive p16 immunostain in the current case, the negative endometrium was confirmatory. Because of the rarity of cervical carcinosarcoma, there are no specific treatment protocols. Prognosis appears to be better than for the uterine counterpart, possibly because of early presentation, 2 but the disease can be very aggressive. The best prognosis appears to be with complete excision, with possible adjuvant chemotherapy and/or radiation added by some clinicians. 5
Footnotes
Author Disclosure Statement
No competing financial conflicts exist.