
Abstract
Abstract
Background:
Juvenile granulosa cell tumors (JGCTs) are very rare and have the potential to be malignant. These tumors are often detected as an incidental finding in young girls prior to puberty. Timely diagnosis is often delayed secondary to lack of specific tumor markers or imaging characteristics.
Case:
A 20-year-old woman, gravida 1, para 0, at 22 weeks and 6 days of gestation, presented to labor and delivery triage complaining of severe left lower quadrant pain. The patient was found to have a large pelvic mass that led to ovarian torsion. Surgical resection was remarkable for JGCT.
Results:
Final pathology was remarkable for a 1157-g JGCT of the ovary measuring 19 × 16 × 9 cm with hemorrhagic necrosis consistent with torsion. The remaining hospital course was uneventful, and the patient was discharged to go home on postoperative day 3 in good condition with a viable pregnancy.
Conclusions:
The current authors' case is the only reported case of a JGCT presenting as a cause for ovarian torsion in a pregnant patient. These tumors are often aggressive requiring proper surgical resection and follow-up. When evaluating pregnant patients with adnexal masses requiring surgical intervention, JGCT should be part of the differential diagnosis.
Introduction
P
Granulosa cell tumors (GCTs) of the ovary are extremely rare neoplasms of the ovarian stromal cells. The incidence of GCTs is 0.2 per 100,000 women, representing only 2%–5% of all ovarian malignancies. 3 GCTs are further divided into adult (AGCT) and juvenile (JGCT) types based on clinical and histopathologic characteristics. JGCTs account for 5% of all GCTs and occur almost exclusively in the first 3 decades of life making a GCT an extremely rare cause of ovarian torsion.
This article presents a rare case of a JGCT discovered in a 20-year-old pregnant woman who presented with an ovarian torsion at 22 weeks of gestation.
Case
A 20-year-old woman, gravida 1, para 0, at 22 weeks and 6 days of gestation, presented to labor and delivery triage complaining of severe left lower-quadrant (LLQ) pain that had begun earlier that day. She described the pain as sharp in character and intermittent. She reported having normal bowel function with no correlation to her pain. A review of her systems was remarkable for new onset of constant debilitating LLQ pain that was worst with movement. On physical examination, she had tenderness to deep palpation in the LLQ, with no guarding, rigidity, or rebound tenderness. The mass was palpable above the uterus. She was not contracting and her cervix was closed and noneffaced. The fetal tracing was reassuring. Transvaginal ultrasound showed an enlarged left ovary measuring 13 × 10 cm with multiple cystic areas. Color and power Doppler imaging showed an absence of internal flow within the left ovary consistent with torsion.
The decision was made to proceed with an exploratory laparotomy for suspected left ovarian torsion. Intraoperative findings included hemoperitoneum with ∼100 mL of blood and a large, dusky, bleeding, edematous torsed left adnexal mass (Fig. 1). There was no identifiable normal ovarian tissue. The remainder of the pelvic anatomy including the right ovary was grossly normal in appearance. The left adnexal mass was torsed. A left salpingo-oophorectomy with pelvic washings was performed and the tissue was submitted for pathology testing. The complete mass was submitted intact with no intraoperative complications.
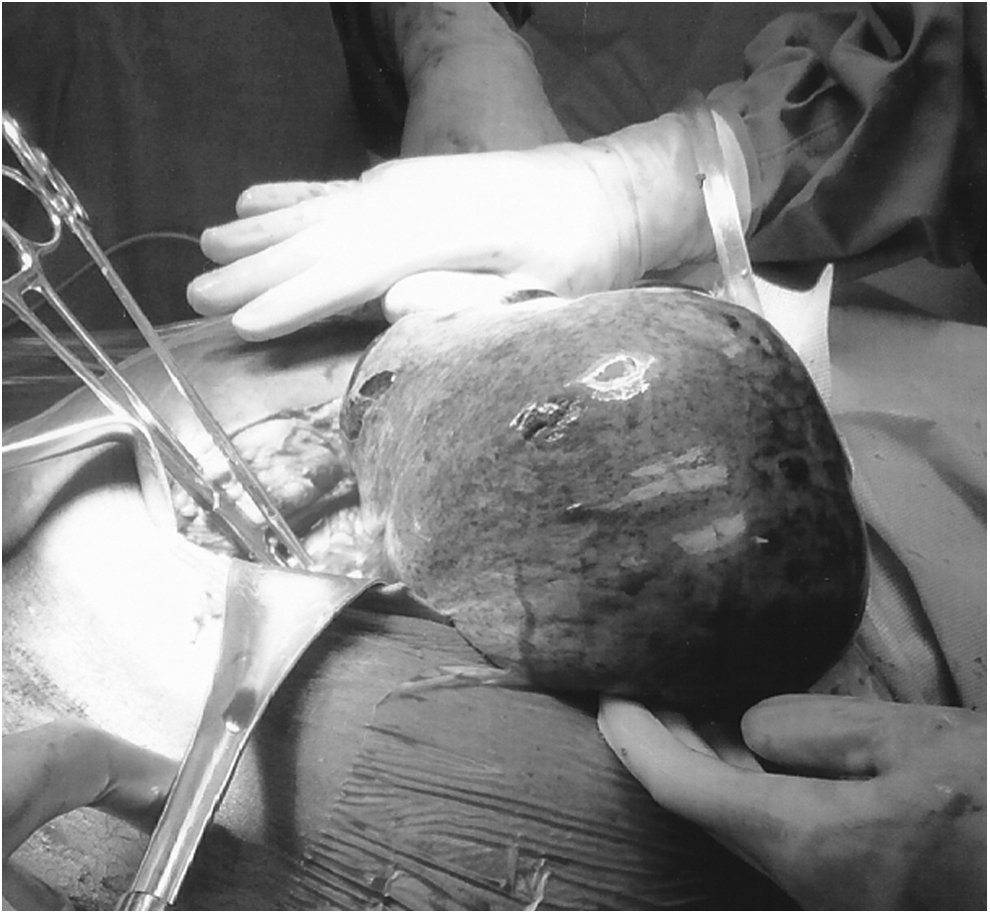
Torsed juvenile granulosa cell tumor.
Results
Final pathology was remarkable for a 1157-g JGCT of the ovary measuring 19 × 16 × 9 cm with hemorrhagic necrosis consistent with torsion. The remaining hospital course was uneventful, and the patient was discharged to go home on postoperative day 3 in good condition with a viable pregnancy.
Discussion
AGCTs are more common and account for 95% of all GCTs. The peak incidence of AGCTs occurs in women ages 45–55, whereas JGCTs most commonly develop in prepubescent girls. 4 Juvenile granulosa cell tumors of the ovary are often very aggressive and are diagnosed within the first 3 decades of life in 97% of cases. In prepubertal cases, the most common clinical presentations include isosexual precocity, as the tumor is estradiol-producing. In the postmenarchal group, the tumor typically may present with abdominal swelling, pain, and/or menstrual irregularities. 5
Retrospective analysis has shown that adnexal masses complicate 0.15% of pregnancies. Of these, ∼50% are mature cystic teratomas, 20% are cystadenomas, 13% are functional tumors, and 13% are malignancies. 6 The incidence of ovarian malignancies presenting in pregnancy is 0.05–0.07 per 1000 pregnancies. Of these, ∼15% are sex cord-stromal tumors. 7 Distinction of these tumors relies heavily on ultrasound characteristics, including septations, echogenicity, and color-flow Doppler imaging. Tumor markers are of little diagnostic value during pregnancy because oncofetal antigens are involved in fetal development and, therefore, were not seen in the current case.
During pregnancy, the optimal management of an asymptomatic adnexal mass <6 cm is conservative. Of note, conservative therapy has been associated with poor outcomes such as torsion. For persistent masses >6 cm, the patient should undergo resection and be counseled about the possibility of malignancy and the need for subsequent staging.6,8 For symptomatic masses, exploratory laparotomy is indicated. In the current case, the emergent nature of surgical intervention preceded the diagnosis of JGCT, which was made with subsequent histopathologic analysis of the resected specimen. For known JGCT, surgery is the primary treatment option, and most are JGCTs are confined to single ovaries that can be safely resected during pregnancy. Optimal timing of resection of asymptomatic tumors is in the second trimester, as this minimizes the risk of spontaneous abortion and preterm labor. 7 It should be noted that it has been shown that termination of pregnancy complicated by ovarian malignancy does not improve maternal survival. 7 The majority of patients present with stage Ia tumors, 9 for which surgical resection alone is effective. In the current case pathology demonstrated an intact capsule, absent ovarian surface involvement; was negative for peritoneal washings; and was negative for carcinoma.
Conclusions
Ovarian masses associated with ovarian torsion occur in ∼15% of pregnancies. 2 GCTs are extremely rare ovarian neoplasms occurring in only 0.2 per 100,000 women. Of note, 10% of GCTs present during pregnancy 4 ; however, to date, only 6 reports in the literature describe JGCTs associated with pregnancy, all of which were detected incidentally either on routine prenatal ultrasound or during cesarean delivery.4,9–12 The current case is the only reported case of JGCT presenting as a cause for ovarian torsion in a pregnant patient. There are no clear definitive methods for diagnosis JGCT prior to surgical intervention. Simple un-torsing of the affected ovary may delay diagnosis further, resulting in negative implications on overall prognosis. When evaluating pregnant patients with adnexal masses requiring surgical intervention JGCT should be part of the differential diagnosis allowing for appropriate counseling preoperatively.
Footnotes
Author Disclosure Statement
None of the authors have corporate or commercial affiliations.