
Abstract
Abstract
Background:
Placental chorangioma is a rare benign placental lesion associated with a multitude of fetomaternal or neonatal complications. Though it is the most common benign condition of the placenta, a chorangioma measuring >5 cm is very rare and leads to various clinically significant consequences.
Case:
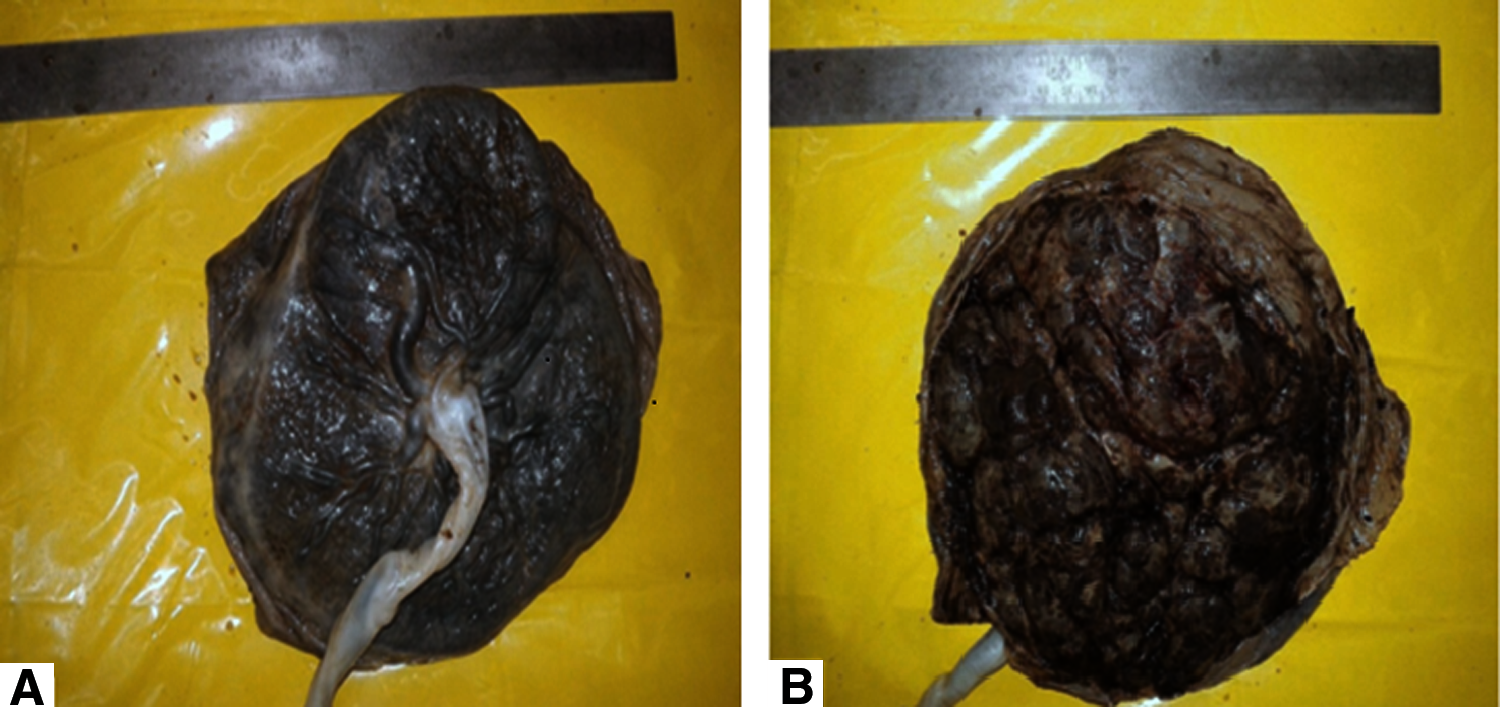
This article presents the case of a 34-year-old multiparous woman, with no significant medical or obstetric history and with an unremarkable clinical status, who was diagnosed with a chorangioma (≈ 12 cm) at 32 weeks of pregnancy by ultrasonography and kept for observation for the rest of the gestation. A few weeks later, she had premature labor and delivered a male child uneventfully via a normal vaginal delivery. The delivered placenta had a well-defined lobular mass on the fetal surface, measuring 12 cm in its greatest diameter and located near the insertion of the umbilical cord. The placenta was intact and complete, and the outer surface of the mass was congested with prominent vascular markings.
Results:
On microscopy, multiple sections from the mass were examined showing numerous dilated vascular channels surrounded by placental stroma and pools of blood seen in few cavernous spaces. Sections from the umbilical cord were unremarkable. The histology results, therefore, confirmed the diagnosis of a chorangioma.
Conclusions:
Despite the clinically significant size of the chorangioma, prematurity was the only complication seen in this case. Still, these lesions should be viewed with caution, as location and vascularity are now increasingly identified as crucial factors in prognosis. Therefore, careful examination of the placenta, timely antenatal diagnosis, and early intervention should be given due emphasis, so that associated morbidity and mortality to both the fetus and the mother can be prevented. (J GYNECOL SURG 33:30)
Introduction
P
Being the most common primary placental neoplasm, chorangioma is seen in 1% of all pregnancies if the placentas are examined thoroughly but in most of the cases is <5 cm in size and is nonsignificant.1,6,7 On the contrary, tumors >5 cm are rare, as in the current case, with prevalence varying from 1 in 3500 to 1 in 9000, and are often associated with a number of complications, thus, emphasizing these tumors' clinical significance.2,8 The complications seen can be either fetomaternal (polyhydramnios, antepartum hemorrhage, preecclampsia, prematurity, nonimmune hydrops, growth restriction, intrauterine fetal death) or neonatal (cardiomegaly, edema, hypoalbuminemia, anemia, thrombocytopenia).1,3,4,9,10 Scarce documentation and limited experience, especially with regard to large chorangiomas, motivated the current authors to write this case report.
Case
A 34-year-old female (G2, P1, L1) with no significant past or present medical or obstetric history, was diagnosed with a large placental chorangioma (≈12 cm) via ultrasonography at 32 weeks of gestation. Imaging also revealed breech presentation and she was kept for observation for the rest of the gestation period. However, spontaneous labor commenced a few weeks later and she delivered a live baby at 35 weeks of gestation with a breech presentation uneventfully via a normal vaginal delivery. The newborn weighed 2.1 kg and showed a few signs of distress, such as grunting, nasal flaring, and tachypnea, which were ameliorated immediately with prompt resuscitation. The mother and her baby were discharged on the fifth day post delivery after the newborn was found to be normal on subsequent examinations. The delivered placenta measured 21 × 17 × 3.5 cm and weighed 484g. There was a well-defined lobular mass on the fetal surface measuring 12 cm in the greatest diameter and located near the insertion of the umbilical cord (Fig. 1A, B). The length of the umbilical cord was ∼25 cm. The placenta was intact and complete, and the outer surface of the mass was congested with prominent vascular markings. On serial sections, the cut surface of the mass was dark red tan to gray/white.
Results
On microscopy, multiple sections from the mass were examined showing numerous dilated vascular channels surrounded by placental stroma and pools of blood seen in a few cavernous spaces (Fig. 2). Sections from umbilical cord were unremarkable. The histology results, therefore, confirmed the diagnosis of chorangioma.
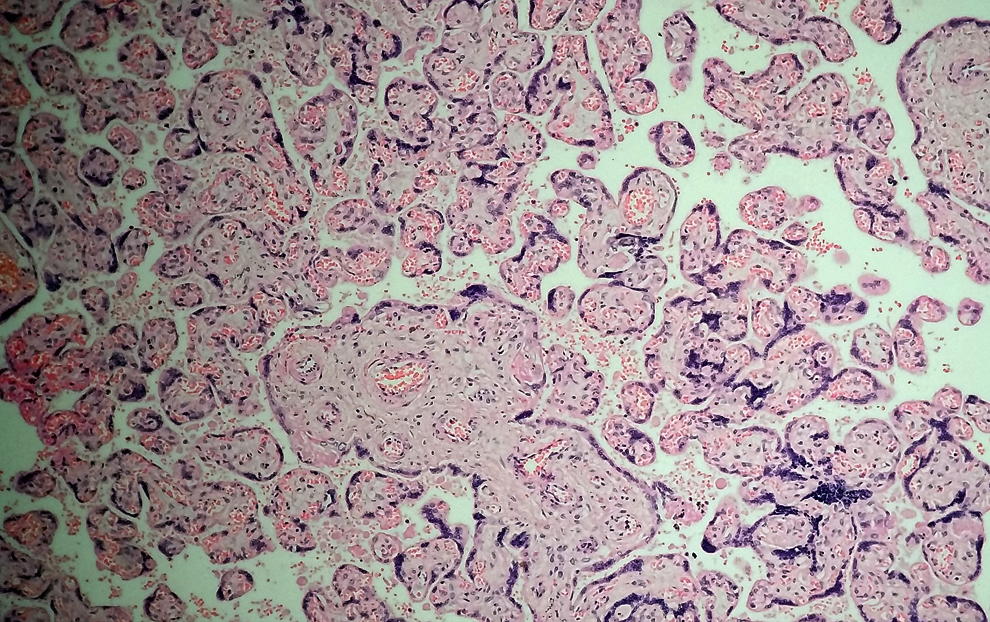
Histologic appearance of the chorangioma showing numerous capillaries surrounded by placental stroma. (10 × hematoxylin and eosin stain) Color images available online at www.liebertpub.com/gyn
Discussion
In the current case, the singlet pregnancy of this 34-year-old multiparous woman with a significantly large placental chorangioma had prematurity as the only adverse effect of the aforesaid placental pathology. As already stated, chorangiomas with size >5 cm are associated with significant complications and the chances of developing complications are directly related to the tumor size. 11 In the current case, the tumor measured ≈12 cm in the greatest diameter, which made it both interesting and unique, as, except for prematurity, no clinically significant complications were seen. With regard to this case, the current authors postulate that prematurity was probably the result of the large volume of the placental chorangioma occupying a significant amount of intrauterine volume and therefore leading to the induction of early uterine contractions that culminated in the premature delivery. However, the absence of other reported complications seen with chorangiomas of this size cannot be explained.
Chorangioma is a benign entity occurring in the placenta of a pregnant woman. This tumor is usually seen more often in Caucasian women than in females of other races and is more common with multiple gestations. 7 There is an apparent dichotomy in its classification between a true neoplasm and a hamartoma, with the majority of researchers considering chorangioma to be a malformation rather than a true neoplasm. Certain environmental factors, such as high altitude, hypoxic stimulus (evident by the presence of fetal nucleated red blood cells in circulation), and vascular growth factors, have been suggested as possible associations with this tumor's occurrence. 7
Chorangioma is often confused with chorangiosis and chorangiomatosis, wherein the former means a diffuse increase in the number of villous capillaries while the latter is characterized by multiple lesions in the placenta with an increased number of villous capillaries permeating the normal villous structures instead of forming an expansile mass.12,13 A chorangioma is often found as a round, homogenous well-demarcated mass, usually on the fetal surface of the placenta (with a few cases reported on the maternal surface as well), usually measuring <5 cm in diameter and being clinically insignificant. Of clinical importance are the cases measuring >5 cm in diameter, as the outcome of pregnancy with chorangioma is greatly dependent on the size of the mass rather than its histologic or immunohistochemical characteristics.
According to histolopathology, chorangioma comprises a benign proliferative network of vessels accompanying connective tissue and an abundant stromal component (Fig. 3). The amount of vascular and stromal components are variable, depending upon the dominant histologic type. 7 The vascular component may comprise either capillaries or sinusoids. Based on histology, the tumor can be defined as capillary, cavernous, endotheliomatous, fibrosing, and fibromatous, but such differentiation is not of clinical concern, as the prognosis rests largely on the size of the tumor. 14 In the present case the tumor was of the capillary type.

Histologic appearance of chorangioma showing numerous red blood cell–filled capillaries (40 × hematoxylin and eosin stain). Color images available online at www.liebertpub.com/gyn
A few case reports in the literature identify an “atypical cellular variant” of chorangioma comprised of markedly abnormal nuclei and high mitotic activity and cellularity, with proliferating malignant trophoblasts interspersed among proliferating capillaries and large areas of necrosis appearing similar to a chorangiosarcoma. However, the absence of invasion and metastasis clearly precludes the possibility of malignant clinical behavior.15,16 Other prognostic factors now presumed to be additionally important in deciding the outcome are vascularity and location of the tumor.5,17 Increased vascularity leads to greater shunting of blood to the physiologic dead space of the tumor, weaning the fetus of a significant amount of nutrient and air exchange and perhaps manifesting as intrauterine growth restriction and fetal demise. Likewise, location is also critical in deciding the pregnancy outcome, as, in certain reported cases, chorangiomas as small as 2 cm located at the outer edge of the placenta have been associated with complications.
In addition to histopathology, which provides a definitive diagnosis of chorangioma, other modalities either supporting or confirming the diagnosis are ultrasonography (particularly color Doppler), fetal magnetic resonance imaging, and immunohistochemistry. Doppler sonography is particularly helpful in differentiating chorangioma from other placental pathologies. 18 Also, immunohistochemistry provides both an authoritative judgment with regard to the diagnosis and provides a clue to the disputed origin or categorization of a chorangioma. This tumor often shows positivity for CK 18 (indicating origin from the chorionic plate and anchoring villi), 19 CD 31, CD 34, Factor VIII, and GLUT 1. Placental chorangioma may also be associated with elevated levels of alpha fetoprotein levels in the maternal blood. 20 The literature also has a few documented cases of recurrent chorangiomas, with little known about the etiology of these recurrences. 21
Conclusions
Chorangioma, though the most common primary tumor of the placenta, often occurs in a size insignificant for its clinical outcome; yet, these lesions should be viewed with caution, as location and vascularity are now increasingly identified as crucial factors in prognosis. Therefore, careful examination of the placenta, timely antenatal diagnosis and early intervention should be given due emphasis, so that associated morbidity and mortality to both the fetus and the mother can be prevented.
Footnotes
Acknowledgment
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Author Disclosure Statement
No financial conflicts exist.