
Abstract
Abstract
Objectives:
The aim of this research was to assess the efficacy of fractional CO2 laser energy for treating vaginal atrophy and lichen sclerosus.
Materials and
Results:
In the vaginal atrophy cohort, 22/23 women who previously complained of dryness and discomfort had these symptoms alleviated and vaginal microscopic exam showed significant changes in color, elasticity, and wetness following 3 courses of CO2 laser fractional treatment; additionally 20/23 women had elimination of urinary frequency and urgency, 18/21 women had alleviation of dyspareunia. In the lichen sclerosus cohort 24/27 patients who had laser treatment reported cessation of itching and pain/discomfort; and 26/27 women demonstrated visible improvement of skin color, elasticity, vascularity following 3-4 laser treatments. All examinations were performed with the operating microscope.
Conclusions:
The fractional CO2 laser beam is useful for treating vaginal atrophy and lichen sclerosus. This new technique represents a significant divergence from estrogenic-, steroid- and corticosteroid-bulwark dependence. All treatments were performed in an office setting and were associated with either no pain or, at the most, minimal and temporary discomfort. This new use of the CO2 laser is an excellent alternative for managing these two troublesome problems, particularly in postmenopausal women. (J GYNECOL SURG 32:309)
Introduction
V
Within the last 2 years, a new type of CO2 laser delivery system, utilizing special superpulse gating with very short duty cycles and penetration depths of 200 μ, has been used to treat vaginal atrophy via a specially designed vaginal applicator. Published data from Italy4,5 and from two unpublished studies in the United States have reported reversals of vaginal atrophy (rejuvenation) and significant reduction of symptoms. Biopsy of the pre-treatment vagina and the post-treatment vaginal wall has shown objective increase in squamous-cell thickness and dermal regeneration.
Lichen sclerosus (also known as sclerosis) is classified as a vulvar dystrophy and is characterized by atrophy of the vulva, hyperkeratosis, and scarring. The symptoms are intense itching, dryness, irritation, and tearing of the vulvar skin. The signs include scar formation, white blanching of the tissues, adhesion formation, and secondary ulceration. 6 The cause of lichen sclerosus is unknown, and the usual treatment consists of nonspecific topical steroids. Yet, subdermal Decadron® injection has been shown to be a reasonable alternative to topical steroids. 7 Topical steroids, over a period of time, will worsen the atrophy already created by the lichen sclerosus. Studies of biopsy materials from women afflicted with lichen sclerosus have revealed a generalized reduction of dermal vascularity and elasticity.
Significance
This study was performed independently but was in conjunction with two other unpublished U.S. studies to determine if the published data from Italy could be reproduced in the United States.
Study objectives
The CO2 laser that was used in the current study is a U.S. Food and Drug Administration (FDA)–approved, class 2 device.
The study described herein explored applications of the laser—not the device itself. The goals of this project were:
• To assess the efficacy of fractional CO2 laser for treating vaginal atrophy and lichen sclerosus • To assess any change in severity of vaginal symptoms and signs associated with vaginal atrophy • To assess the relief of symptoms of lichen sclerosus following laser treatment to the vagina/vulva • To assess improvement in vaginal/vulvar symptoms using a visual analogue scale (VAS) • To assess signs of vaginal atrophy reduction using the Vaginal Health Index Scale and by checking vaginal-wall elasticity • To assess sexual function and QoL • To assess patient satisfaction (with a 5-point Likert scale) • To assess vulvar improvement by microscopic evaluation • To assess vulvar elasticity via clinical examination and a rating analogue scale • To assess reduction is fissure formation and fusion of vulvar tissues.
Materials and Methods
Study population
Inclusion criteria were postmenopausal women who had been diagnosed via microscopic evaluation with vaginal atrophy and who were symptomatic, and women who had been diagnosed by biopsy with lichen sclerosus and who were symptomatic.
Exclusion criteria were women who had received medications that could interfere with treatment 2 weeks pre-treatment or during treatment cycles/follow-up and women who had active genital infections or vaginal/vulvar neoplasia.
Study design
Originally, 10 women with diagnosed vaginal atrophy and 5 women diagnosed with biopsy-proven lichen sclerosus were selected to be enrolled into the trial and treated. The entire investigation was approved by the St. Helena Hospital Institutional Review Board (IRB). The principal investigator was required to take and complete the National Institutes of Health course on “protecting human research participants” successfully and was awarded certificate # 1744262 after completing the course. The study was approved to continue, and subsequently, 23 women were treated in a vaginal atrophy group and 27 were treated in a lichen sclerosus group (i.e., a total of 50 women).
The treatment consisted of CO2 laser exposure of 20–30 Watts, a dwell time of 1000 microseconds, dot spacing of 1000 micrometers, and a treatment time of 10 minutes. All treatments fell into the category of “standard of care.” Treatment cycles included 3 laser applications at monthly intervals. Follow-ups occurred at 6 months and 12 months in addition to monthly × 4 follow-ups. The CO2 laser equipment was provided by Cynosure, Westford, MA, and was manufactured by DEKA, Florence, Italy, under the trade name Monalisa Touch® SmartXide V2LR. (Fig. 1).

The Monalisa Touch® SmartXide V2LR CO2 laser with a vaginal probe attached to an articulated arm.
The treatment protocol for vaginal atrophy used a specially designed vaginal probe (Fig. 2) that was inserted into the full length of the vagina and could be felt by the patient as an abdominal sensation. The probe device was designed with a terminal and angulated mirror to reflect the laser beam to the vaginal wall. When the laser foot switch control was pressed, the laser fired and targeted the vaginal wall. Each time the laser discharged, the probe was rotated. After 20+ firings, the probe had completed a 360° rotation. The probe was then pulled caudally ∼1 cm, and the above process was repeated. Repetitively, after 8–10 rotary cycles, the lower vagina was reached and the treatment was stopped (i.e., the entire vagina was, in fact, probed). The specifications for treatment were 30 Watts, a 1000-microsecond pulse duration, and a 1000-micrometer pulse width.

Detail of vaginal probe, with the angulated terminal mirror to facilitate treatment of the entire circumference of the vagina. The scan pattern is visible in the mirror.
Patients were evaluated for symptoms based on face-to-face interviews and were scored objectively according to findings of colposcopic (microscopic) examinations prior to each treatment cycle and 1 month following the third treatment (Fig. 3).

The author's office is equipped with an operating microscope with a video camera attached to the beam splitter. This allows the patient to view her examination with the same optical field as the gynecologist.
The vaginal score index consisted of 5 measures: elasticity; fluid volume; pH; epithelial integrity; and moisture. (Each parameter was graded 1–5, with 5 being highest; a total score of >15 is considered to be atrophy).
All symptoms for vaginal atrophy/lichen sclerosus were measured via a 10-point VAS, with 0 being no symptoms and 10 very severe and barely tolerable symptoms.
After each laser application, degree of discomfort encountered during the treatment was documented based on a 10-point VAS (0 = no pain; 10 = pain as bad as it could be).
The treatment of vulvar lichen sclerosus utilized a hand-held forked probe that facilitated an accurate focal length of the delivered laser beam (Fig. 4). The laser was scanned via a boxlike pattern (Fig. 5) in order to encompass the entirety of involved vulva tissue. Settings for the vulvar laser treatment were: Watts, 20; time, 1000 microseconds; and width 1000 μ (Fig. 6).

The forked probe facilitates applying a focused laser beam to the vulvar tissue for lichen sclerosus treatment.
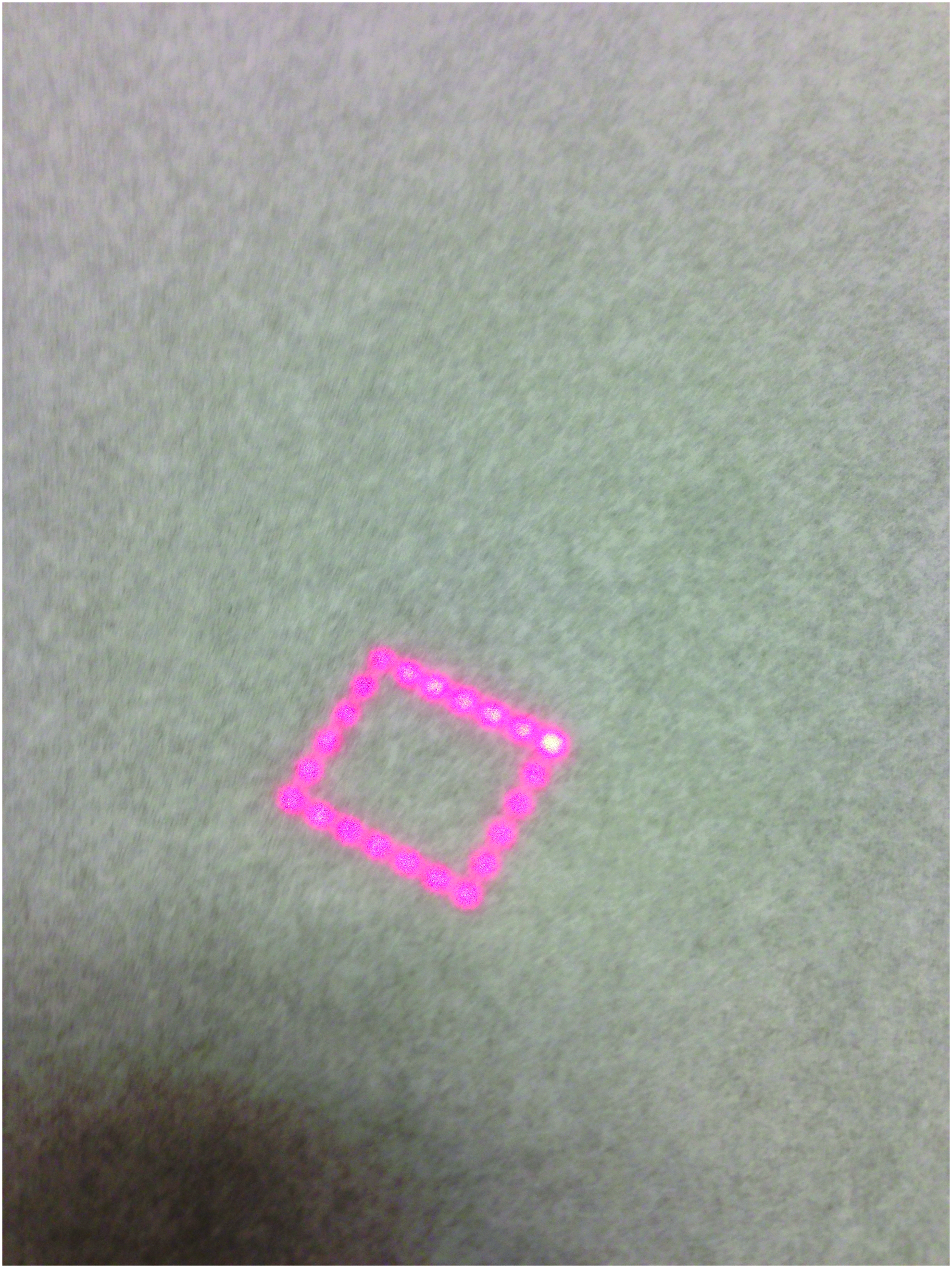
Box scanning pattern utilized for both vaginal and vulvar laser treatment.
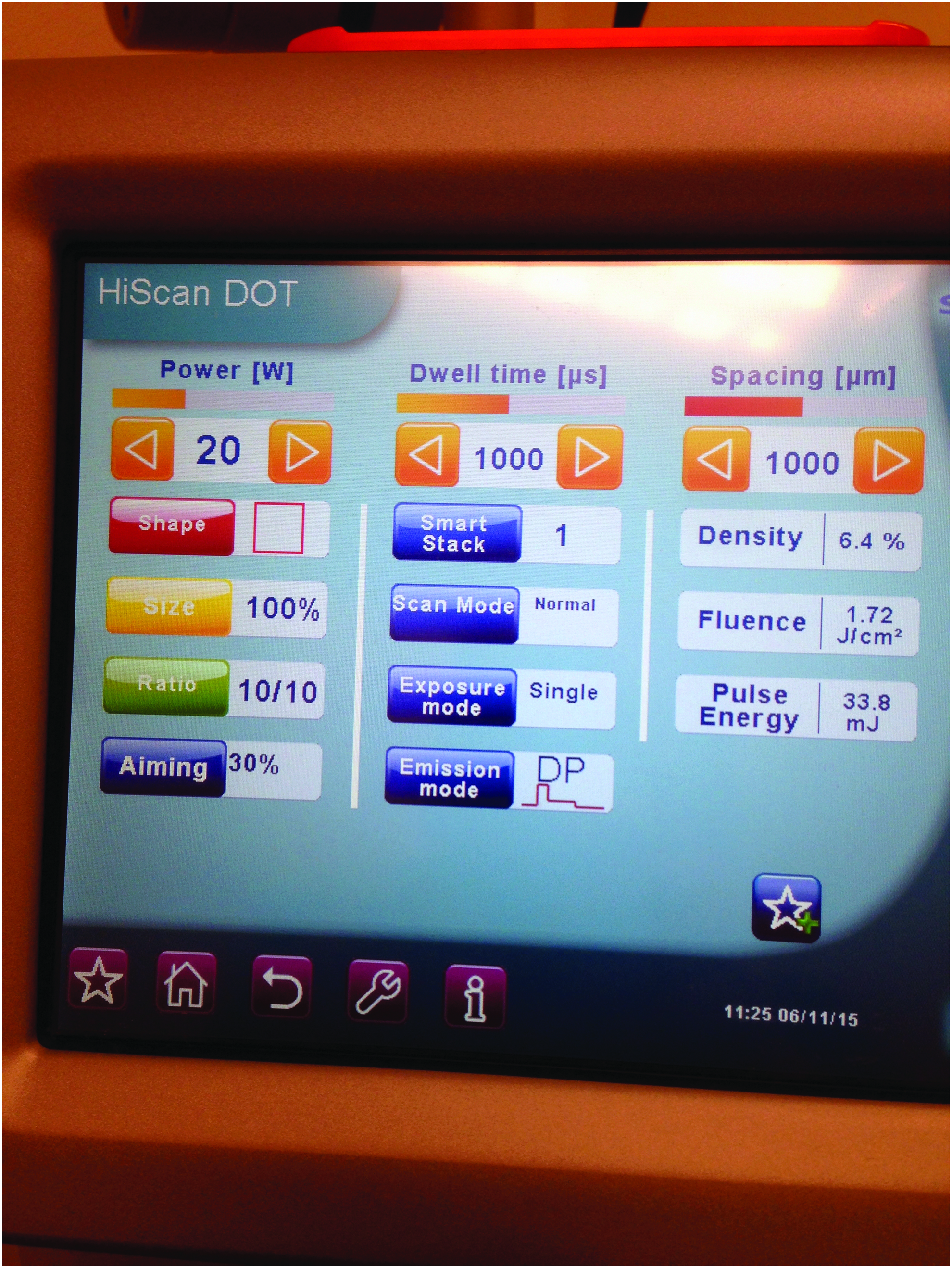
Specs for lichen sclerosus CO2 laser treatment are: power, 20 Watts; time on tissue/emission, 1000 microseconds; and interval, 1000 micrometers.
All patients with lichen sclerosus had universally undergone pre-laser biopsy, which established the correct diagnosis (this is routine for any patient suspected of having lichen sclerosis).
Data and data collection
All data were collected onto each patient's permanent electronic medical record and secured by Adventist Health Care.
Reporting data did not identify individual patients in any way and the principal investigator controlled all access to identities of the study patients. No specific patient identification was utilized relative to the results of this study.
Results
Vaginal atrophy group
The mean age of the 23 women who participated in the vaginal atrophy portion of the study was 67. The mean parity was 2. Each patient underwent a complete pre-treatment history and physical examination. The examination included a microscopic mapping of the vagina as well as the vulva. The vagina was graded based on five of six vaginal indices (Tables 1, 2, and 3). In this group, 23/23 patients complained of vaginal dryness and irritation, as well as discomfort during coitus. Two women had had no sexual encounters for 8–10 years because of progressive introital strictures; 5/23 women complained of continuous vaginal burning; 10/23 women complained of urinary frequency, urgency, and/or incontinence; 19/23 complained of intermittent hot flashes; and 5/23 women had histories of breast cancer. In this breast-cancer subgroup, 4 patients had been advised to avoid any estrogenic intake by their oncologists. These patients had heard of a laser “rejuvenation” study and were referred for participation by their own gynecologists. Prior to each of the 3 laser treatment sessions, microscopic examination of the vagina was repeated and observations were recorded and graded.
Scoring: 1–5, with 1 being thin, dry, poor elasticity, with subepithelial bleeding; and with 5 being a mature thick-walled vagina with excellent stretch characteristics and showing moisture as well as a rugal pattern.
Scoring: 1–5, with 1 being thin, dry, poor elasticity, with subepithelial bleeding; and with 5 being a mature thick-walled vagina with excellent stretch characteristics and showing moisture as well as a rugal pattern.
Scoring: 1–5, with 1 being thin, dry, poor elasticity, with subepithelial bleeding; and with 5 being a mature thick-walled vagina with excellent stretch characteristics and showing moisture as well as a rugal pattern.
Six weeks after the completion of the third treatment, a fourth microscopic examination was performed (Fig. 3). The most consistent changes observed after the first 2 treatment sessions, and following the third treatment session in each patient of this group, were: (1) A notably pinker color of the vaginal walls; (2) increased moisture within the vagina; and (3) more-pliable vaginal walls, particularly at the anterior–lateral and posterior–lateral sulci. No definite epithelial thickening was observed and no increase in the rugal pattern was observed. No change in sensitivity to touch was identified.
No patient undergoing vaginal laser scanning reported any discomfort during or following each treatment session. Every study participant was asked specific questions about untoward side-effects of the laser treatment, particularly those relating to discomfort. In addition, no anesthetic or analgesic agents were administered to any of the women during this study. The patients did describe a not-uncomfortable vibration-sensation within their vaginas concurrent with each laser discharge. No patient received any hormonal preparations locally or systemically. Three women in this cohort underwent a fourth treatment because of symptom recurrence; the average time interval between treatments 3 and 4 was four months.
Based on a scale of 1–5, in which 1 is the worst and 5 is the best, evaluation of the pre-treatment mean scores totaled 8.5 (atrophy). In contrast, post-treatment mean scores totaled >15. In this group, 22/23 patients reported that their vaginal dryness and discomfort had disappeared entirely. Urinary urge/frequency was not present in 20/23 patients, and dyspareunia was significantly diminished or eliminated in 18/23 women.
Lichen sclerosus
As noted above, all patients with suspected lichen sclerosus had pre-treatment biopsies to confirm the diagnosis of lichen sclerosus. Patients were subdivided based on severity of disease as follows: severe (Fig. 7), 17 patients; moderate, 8 patients; mild/moderate, 2 patients (Table 4). Severe cases encompassed >66% of the vulva; moderate cases involved >50% of the vulva; and mild/moderate cases <50% of the vulvar surface. At least 3 treatment courses were given for all 27 women at intervals of 4–6 weeks. Laser power was set at 20 Watts with 1000-microsecond pulsing. Treatment was delivered via a specially focused hand piece incorporating a boxlike scanning configuration (Fig. 8). Five women required a fourth treatment because of recurrent symptoms of itching. No patient as of this writing has undergone more than four treatments (Table 5). No patient experienced progression of disease (Table 6).

This patient has severe lichen sclerosus and accompanying severe itching and pain.

Treatment in progress. Note the labial pallor which is typical for lichen sclerosus.
Treatment settings were at 20 Watts; 1 millisecond.
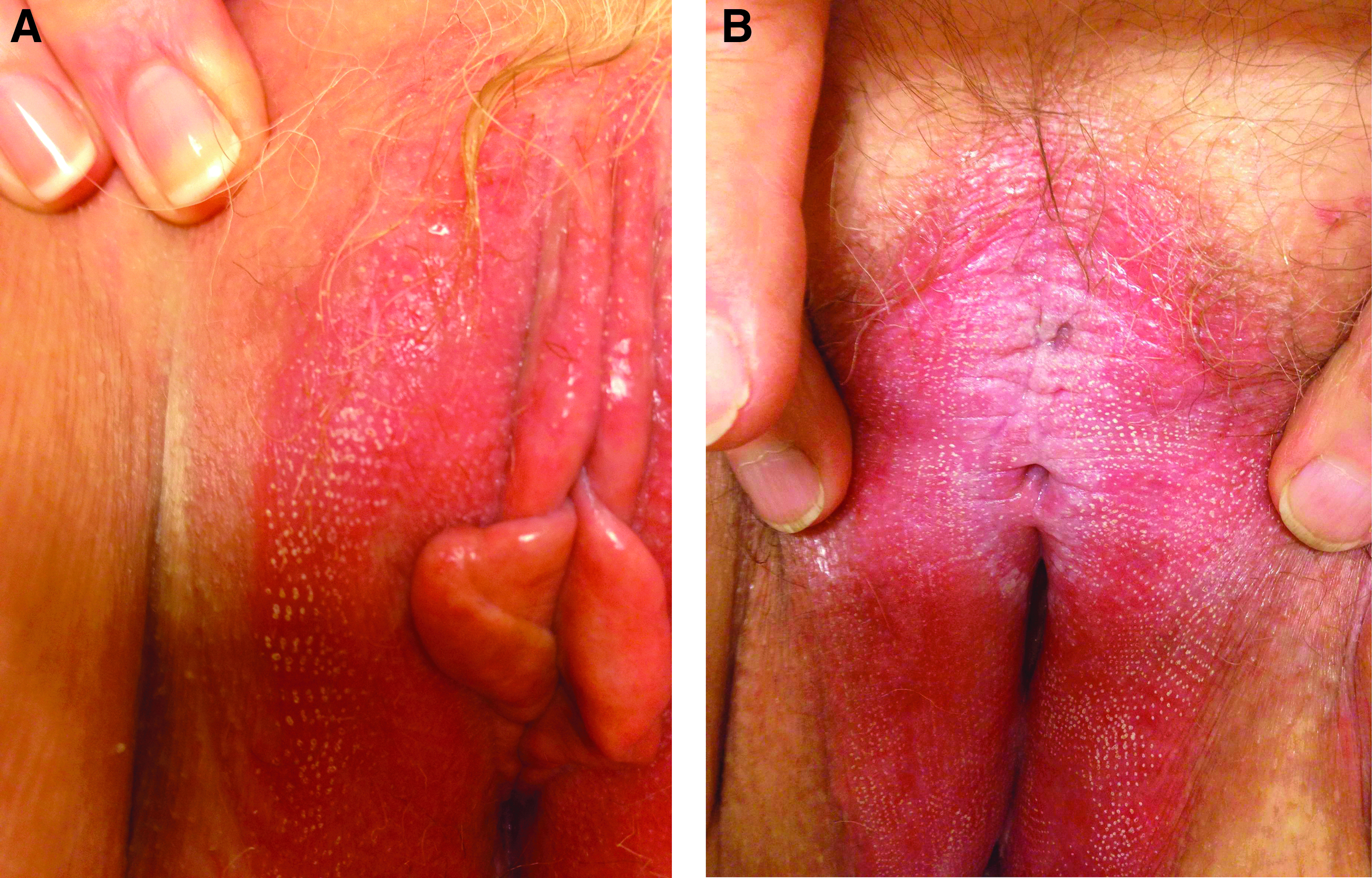
Visible improvement of the vulvar skin was seen in 26/27 patients, while 24/27 women have had no further itching or any sort of vulvar discomfort or pain. Visual examination pre- and postoperatively utilized an operating microscope (Table 6). These examinations were performed prior to the first treatment and prior to all subsequent treatments as well as during post-treatment follow-up examinations. Following the first treatment, the vulvar skin of each patient had a pinker color and was more pliable. Signs of inflammation disappeared and ulceration that was previously present disappeared as did fissure formation. Previously observed scarring was unchanged as were areas of previously observed pallor.
During treatment, at each firing of the laser, small holes were visible on the vulvar skin in a pattern coincident with the boxlike pattern preset on the laser hand-piece (Fig. 9A). All women undergoing vulvar laser treatment required topical local anesthesia. Even after eutectic mixture of local anesthetics (EMLA) cream applied 60 minutes prior to the treatment, further topical 2% lidocaine gel was required to diminish pain sensation, which was described as needle-like and which was associated with each laser discharge. The immediate post-treatment routine consisted of: topical nystatin/triamcinolone cream applied to the vulva 3 times per day for 48 hours; once daily cleansing of the vulva with Hibiclens® liquid for 48 hours; and application of an ice pack for 15 minutes, 3 times per day for 24 hours post-treatment (Table 7).
Discussion
The effects of menopause on QoL for symptomatic women have been studied widely and published in the medical literature. Atrophy of the vagina produces a variety of symptoms and, as a subset of menopausal conditions, has been the subject of an extensive literature.8–15 Given that the vagina is a key component to sexual relations, its health and function create interest not only in affected females but also among their male partners. 16 Reduced to the lowest common denominator, atrophy is a physiologic response to the normal aging process and will be affected adversely by disuse. When age-related atrophy is coupled to cessation of coitus, the epithelial and stromal reductions will result in diminished capacity and ultimately to structural shrinkage precluding penile insertion.
Although a wide range of therapeutic measures have been reported for treating vaginal atrophy, the mainstay of management relies on systemic and/or local estrogenic preparations. The safety of systemic estrogens has been questioned because of the adverse actions of these drugs on the endometrium, breast, and cardiovascular system concurrent with salutary actions on the vagina. Topical estrogenic drugs have been the preferred route of delivery by gynecologists based on perceptions that local, concentrated estrogen can and will reverse atrophy, while, at the same time, would not be absorbed into the systemic circulation. Recent data, however, refute these beliefs about absorption of these agents.17–19 Furthermore, administering the topical estrogen is messy, imprecise, and costly. Estrogen delivery via rings requires the ring device to be inserted and worn.20–22 The latter presents the problem of a foreign object that remains within the woman's body and an object that likely no males would ever tolerate.
Oncologists have more-or-less the opposite opinions of gynecologists regarding the safety of administering any estrogenic preparation to patients who have breast cancer (i.e., estrogen is potentially detrimental to the patient's chances of survival and should not be administered).23–27 As a result of this controversy, numerous nonestrogenic remedies for treating vaginal atrophy have been reported in the medical literature. These range from simple lubricants to androgenic steroids and homeopathic preparations.28–33
Very recently, laser devices have been reported as beneficial alternatives to topical estrogen—as well as other topical preparations—by producing a heating action on the vaginal cellular structures that, in turn, reverses the effects of aging (i.e., atrophy).34–37 The data reported herein supports the thesis that subablative laser energy acts to reverse some of the adverse effects of vaginal atrophy. The current does not speculate or theorize in this report that the laser action creates collagen deposition. Given that the visually seen actions of the CO2 laser create multiple tiny holes in the vaginal wall in addition to heating the vaginal subepithelial tissues—neovascularity would more than likely be the most logical explanation for the lasting benefits of laser treatment. The additional benefit of the laser device is that it is a mechanical tool rather than a drug.
Lichen sclerosus is a disorder that affects the vulva among other locations in the human body. The disease is characterized by creation of inflammation and ultimately serious scar formation leading to shrinkage/atrophy of the targeted tissue. In women, the vulva is the principal targeted tissue. 7 The actions of lichen sclerosus are associated with intense itching, principally during bedtime hours. What is more serious is the association of lichen sclerosus with the development of invasive squamous-cell carcinoma, which is curiously not related to the actions of the human papilloma virus. The cause of lichen sclerosus is unknown, although speculation favors an autoimmune origin.
Lichen sclerosus may be suspected in a patient based on visual clinical observation together with clinical symptomatology. However, the diagnosis can only be made by biopsy and pathologic confirmation. The pathologic criteria for diagnosis include the following: epithelial atrophy (e.g., reduction of cell thickness from 20 cells to <8 cells; disruption of the basal-cell layer; collagenation of the underlying dermis; reduction of vascularity; lack of rete pegs and coincident dermal papillae; and hyperkeratosis.
For the most part, lichen sclerosus treatment has not evolved beyond topical steroids. The minimal strides in managing lichen sclerosus have focused mainly on the development by the pharmaceutical industry of increasingly potent topical corticosteroid preparations. The most frequently utilized topical drug is clobetasol propionate. 38 The problem with topical steroid drugs, particularly chronic, long-term usage, is the propensity for the topical medication to worsen the atrophy and create an increased risk for skin infection. Further variations related to the number of applications per day and amount of drug applied creates inexactitude. To overcome the aforesaid problems, an alternative technique of bimonthly subdermal Decadron injections has been reported. The advantages of these injections are; (1) delivery of the steroid directly to the dermis; (2) known dosage of delivered drug to the target tissue; (3) treatment administered every 2 months rather than daily, and (4) a lowered risk of instigated atrophy. 39
This study generated data showing that the CO2 laser is a clear mechanical alternative to estrogenic drugs for treating vaginal atrophy. The study also provided indisputable evidence, for the first time, illustrating the application of CO2 laser subablative heating and minipuncture penetration of afflicted vulvar skin as a bona-fide treatment for ameliorating lichen sclerosus and its accompanying pruritus (Fig. 9). The question that this study failed to answer relates to the frequency and interval beyond the 3 treatment routines that were arbitrarily set at the initiation of the project. As of this writing, 6/27 (22%) patients in the lichen sclerosus arm of the study have undergone a fourth laser treatment.
Conclusions
The CO2 laser has been approved for treating various conditions by the FDA. Literature dating back to the 1970s have demonstrated advantages for the CO2 laser wave length with respect to safety as well as precision vaporization and cutting. Only recently, have data been published addressing the use of this laser for subablative warming of tissue and fine controlled shallow drilling based on very-short pulse intervals and very-small pulse widths. Although pulsing techniques are not new, the methodology and sophisticated gating are unique and recent developments. Thus, new applications for an otherwise older laser have yet to be approved by the FDA; hence, the genesis of the current investigation as IRB-sanctioned research.
The study herein demonstrated that a specially designed and uniquely delivered CO2 laser system is capable of treating vaginal atrophy effectively. It offers a suitable alternative to systemic or local estrogen therapy. Similarly, the CO2 laser system is a better alternative for managing lichen sclerosis, compared to routine, topical steroid applications onto the vulvar skin with their attendant serious side-effects.
The shortcomings of this study include: small numbers of participants (i.e., a total of 50 patients); reported arbitrary wattage and gating specifications; unknown, definitive treatment intervals; and number of treatment repetitions.
Footnotes
Author Disclosure Statement
No financial conflicts exist.