
Abstract
Abstract
Objective:
The aim of this research was to determine the types, indications, and operative outcomes of elective hysterectomies at the Lagos University Teaching Hospital (LUTH), in Lagos, South West, Nigeria.
Design:
This was a descriptive retrospective study of hysterectomies performed at LUTH from January 1, 2008, to December 3, 2012.
Materials and Methods:
Case notes of patients undergoing elective hysterectomy were retrieved from the hospital's records department, and relevant information was extracted. Collation and analysis of data were performed, using the Epi Info statistical software package, version 7.2.
Results:
Hysterectomies accounted for 9.4% of all gynecologic surgical procedures. The mean age and parity of the studied women was 49.9 ± 7.7 years and 3.74 ± 1.57, respectively. Total abdominal hysterectomy and bilateral salpingo-oophorectomy (TAH/BSO) was the most commonly performed (50.8%), and vaginal hysterectomy (VH) (14.5%) was the least performed. There was a rising trend in the number of TAH/BSOs (7%) and radical hysterectomies (RHs; 25%), with a 40% reduction in the number of VHs performed over the study period. General anesthesia was most commonly preferred anesthetic technique (66.7%), while uterine fibroids were the most common indication for hysterectomy. The mean units of blood transfused were 2.2 ± 1.5 units, and the mean days of postoperative admission was 8.0 ± 4.9 days.
Conclusions:
There is an urgent need to fortify postgraduate specialist training as a way to improve the skills of future gynecologists so they can perform procedures such as VH to improve the overall outcome for Nigerian women undergoing hysterectomy. (J GYNECOL SURG 33:193)
Introduction
H
The hysterectomy rate in Lagos, South West, Nigeria, was 9.3%, 4 while rates of 8.5%, 5 and 16.4% 6 were reported from Ilorin and Calabar, respectively. In developed countries, the rates are far higher. In the United Kingdom, 20% of women would have had hysterectomies by 55 years of age. 1 Rates of 5.4 and 3.7 per 1000 have been quoted for the United States 1 and Italy, 3 respectively. Uterine fibroid and menstrual disorders are the two most common indications for hysterectomy in both developing and developed countries.1,3,7 Other indications include benign gynecologic conditions—such as symptomatic adenomyosis and chronic pelvic pain refractory to conservative management—as well as gynecologic cancers—such as cervical, ovarian, and endometrial cancers.1,4,7
The routes of surgery for hysterectomy could be abdominal, vaginal or laparoscopic.1,2 Vaginal hysterectomy (VH) is mostly indicated in cases of pelvic organ prolapse and for other indications when pelvic adhesions are not suspected or expected.1,3,7 The rate of VH is higher in developed countries because of their lower overall rates of pelvic adhesions from infections and the higher skill levels available for the procedure.5–7 The abdominal route is usually preferred when there is an associated need for adnexectomy in the setting of gynecologic cancers. 1 Endoscopic equipment needed for laparoscopic hysterectomy is expensive and is not readily available in most developing countries. Hysterectomy can be total when the cervix is removed or supracervical when the cervix is retained.1,3 The advantage often cited for doing a total hysterectomy is the removal of a potential focus for cervical cancer.1,3 However, even when total hysterectomy is indicated, the presence of dense pelvic adhesions may sometimes preclude this approach.
The most common complication of hysterectomy is infection. Even with the most careful patient selection and application of very good surgical techniques the rate is not <10%.1,5,7 Hemorrhage occurs in 0.2%–2% of cases. 8 Other complications specific to the procedures include ureteric and bladder injuries.5–7 Bowel injuries occur infrequently and heal well following primary repair when preoperative bowel preparations were made. 1 The mortality rate is 0.1%–0.2%.1,7 The mortality rate is influenced by the age of the patient. It is also increased when surgery is performed for cancer and obstetric complications. 7
The last review of hysterectomies in the Lagos University Teaching Hospital (LUTH) in Lagos, South West, Nigeria, was carried out in 2003. 5 The current study was therefore performed to find out the type distribution, current indications, and perioperative complications of elective hysterectomies in LUTH over a 4-year period, between January 2008 and December 2012.
Materials and Methods
This study was a descriptive retrospective review of women who had elective hysterectomies done at the LUTH between January 1, 2008, and December 31, 2012. LUTH has more than 1000 beds and is a teaching hospital located in the Central Lagos metropolis in South West, Nigeria. The hospital immediate environ is inhabited by civil servants, students, traders, and artisans. LUTH also provides services to patients from the neighboring southwestern states. This hospital is the largest in the state and offers mainly clinical services such as obstetrics and gynecologic services. 9
The registration numbers of all women who had hysterectomies during the period under review were obtained from the modular theater and ward registers and the patients' case notes were subsequently retrieved from the medical records department. Relevant information—such as sociodemographic characteristics, type of hysterectomy, anesthetic technique, indications, and perioperative events—were obtained using a structured proforma. Data were collated and analyzed using Epi Info statistical software package (version 7.2; United States Centers for Disease Control and Prevention), and results were then presented as frequencies and percentages, using tables and charts.
Ethical approval was obtained from the hospital's Health Research and Ethics Committee before commencement of the study.
Results
A total of 181 elective hysterectomies were carried out during the study period of a total of 1923 gynecological surgical procedures, giving a rate of 9.4% (or 94/1000 women) in this study. However, only 165 case notes were successfully retrieved and analyzed.
As shown in Table 1, the age range of the studied women was 27–76 years, while the mean age was 49.9 ± 7.7 years. The majority of the women had parity between 3 and 4 (30.9%) with a mean parity of 3.74 ± 1.57. Total abdominal hysterectomy and bilateral salpingo-oophorectomy (TAH/BSO) was the most commonly performed operation (50.8%), while VH was the least performed (14.5%) of all the types of hysterectomies (Table 2). There were no cases of laparoscopic hysterectomy during the review period.
TAH, total abdominal hysterectomy; BSO, bilateral salpingo-oophorectomy; VH, vaginal hysterectomy; RH, radical hysterectomy.
Figure 1 shows the change in trends of the types of hysterectomies performed between 2008 and 2012 with a rising trend observed in the number of TAH/BSOs (7%) and radical hysterectomies (RHs; 25%) over the study period. There was also a 40% reduction in the number of VHs performed over the same period. General anesthesia was the most commonly preferred anesthetic technique (66.7%) in all the hysterectomies performed during the period under review. Uterine fibroids were the most common indication for hysterectomy, accounting for 44.2% of all the audited cases, while choriocarcinoma was the least indicated reason for the procedure (1.8%).
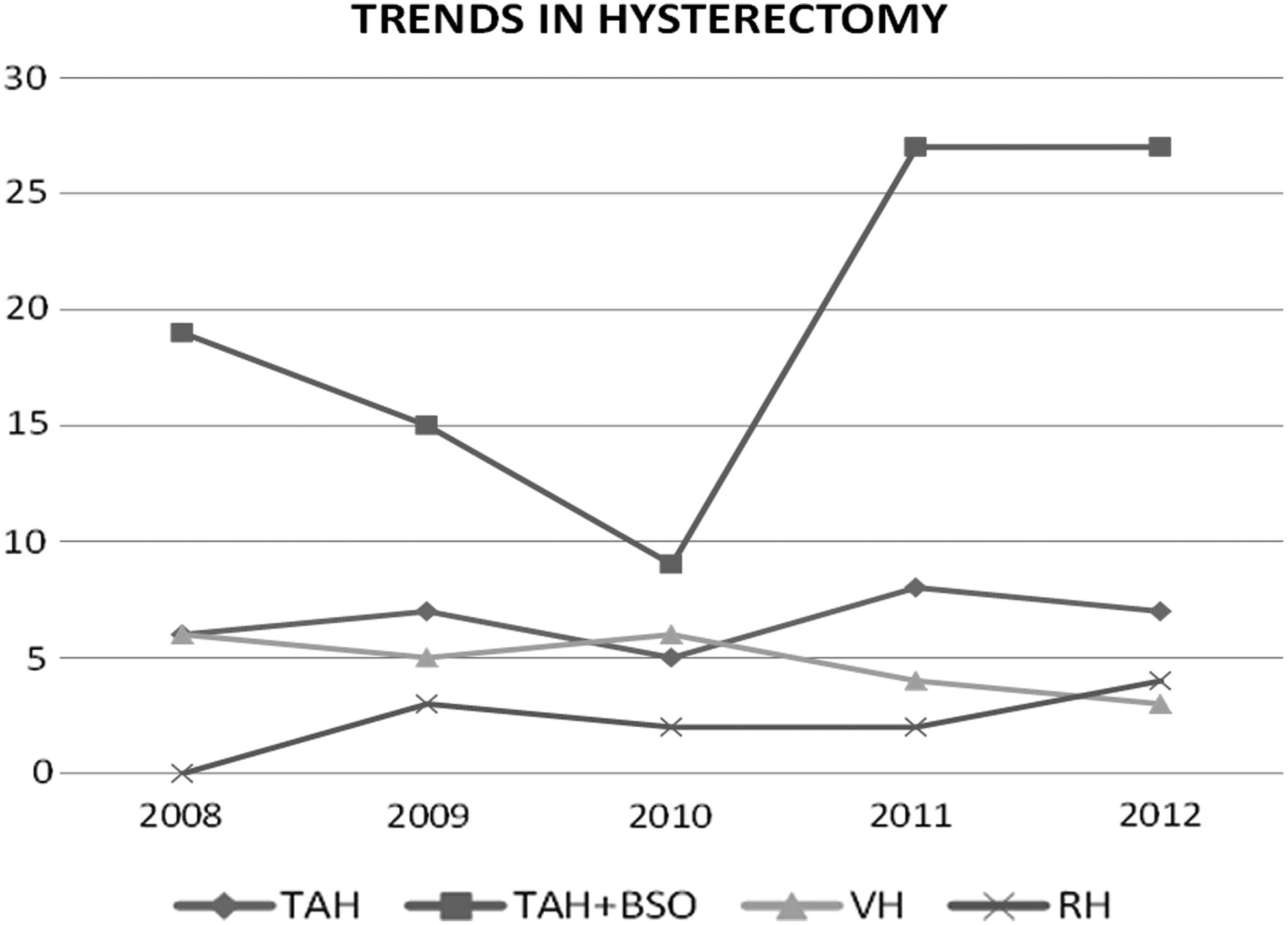
Trends in the various types of hysterectomies (2008–2012). TAH, total abdominal hysterectomy; BSO, bilateral salpingo-oophorectomy; VH, vaginal hysterectomy; RH, radical hysterectomy.
As shown in Table 3, the mean blood units transfused to the studied women perioperatively during the period of review was 2.2 ± 1.5 units. Women who had RH had the most number of units transfused. The mean days of postoperative admission was 8.0 ± 4.9 days after hysterectomy with only 5 (3.0%) of the women spending a minimum of 15 days in the hospital due to one operative complication or another. Two (2) deaths were recorded during the review period, giving a mortality rate of 0.12% (or 12.1/1000 women).
Discussion
The reported rate of hysterectomy in this study was 9.4%, and this was similar to the rates of 8.5%, 9.3%, and 10.2% reported in Ilorin, 5 Lagos, 4 and Ibadan, 10 respectively. It is however much lower than the rates of 16.4% and 25.9% reported in Nnewi 6 and Awka, 11 respectively. The disparities in rates may be due to regional differences in culture, as women of southeastern Nigerian origins may find hysterectomy more acceptable than women from other regions of Nigeria. It may also be due to a lower threshold for performing hysterectomy among physicians in the southeastern part of the country. The rates reported all over Nigeria are far higher than the 5.4 and 3.7 per 1000 women reported in North America1,12 and Europe,3,13 respectively, and this is largely due to the increasing recourse to conservative methods such as endometrial ablation and insertion of the LNG-IUD as alternatives to hysterectomy for treating benign gynecologic conditions in these countries. 7
The mean age of 49.9 ± 7.7 years recorded for the women in this study was similar to that in other studies performed within and outside Nigeria, where the average age for these women was in the forties.1,2,5,11,14 This may be due to the increased acceptability of hysterectomy in this age group of women who are more likely to have completed their families. This is corroborated by the findings from this present study (with a mean parity of 3.74 ± 1.57) and other previous studies4–6,11 wherein the majority of the women studied were found to have higher parity. This can also be explained further by the cultural importance attached to childbearing in our environment, as women with children are more willing to choose hysterectomy for the treatment of their gynecologic conditions. The finding that a large proportion (50%) of the women in this study belonged to the Yoruba ethnic group could be attributed to the fact that the study was done in Lagos, which is located in the South West part of Nigeria, where the Yoruba ethnic group is predominant. 15
The rising trend observed in the number of TAH/BSOs and RHs in this study could be an indication of the increased incidence of gynecologic malignancies seen in the current environment or could be a result of the improvement in the number of radical surgical procedures being performed in the gynecologic oncology unit of the study center. Nonetheless, VH still had the lowest percent (14.5%) of all the hysterectomies performed during this period just as had occurred in previous local studies.4,14 This could be explained by the relative lack of skilled surgeons with adequate experience in performing the procedure, compared to the developed countries.5–7 The abdominal route is therefore usually preferred in most cases in the current settings. The 40% reduction in the number of VHs performed over this study period with a corresponding increase in the number of hysterectomies performed through the abdominal route corroborated further the increasing dearth in the number of gynecologists skilled in VH. This could be an indication of the fall in the standard of postgraduate specialist training in Nigeria. However, these reduced trends were also noted in studies performed in Taiwan 16 and Saudi Arabia. 17
The largest proportion (66.7%) of the hysterectomies performed during the period under review was through general anesthesia. This is not surprising, as the majority of the surgeries were via the abdominal route. General anesthesia is still regarded as the standard anesthetic technique for major abdominal procedures, 18 although regional anesthesia is now known to be associated with faster postoperative recovery and reduced postoperative complications, such as pain, postoperative nausea and vomiting, and drowsiness. 19 Symptomatic uterine fibroids were the most common clinical indication for gynecologic hysterectomy in this study, a finding that was similar to those from previous Nigerian studies in Lagos, 4 Ilorin, 5 Nnewi, 6 and Awka. 11 Choriocarcinoma is the least indicated reason for hysterectomy in this study, as chemotherapy is the cornerstone of its treatment while optimal treatment results can occasionally depend on the addition of hysterectomy in a few selected circumstances or in cases with life-threatening hemorrhage. 20
The mean units of blood transfused perioperatively in this study (2.2 ± 1.5 units) was similar to that reported in Ilorin. 5 Women who had RH had the most number of units transfused. This can be explained by the extensive tissue dissection and increased operation time associated with the procedure. The mean days of hospital stay of 8.0 ± 4.9 days recorded was also similar to what was reported in the Awka study 11 but was lower than the 10.15 ± 4.8 days observed in Ilorin. 5 The mean days in the current study, however, is much higher than the 4.48 ± 1.67 days quoted from an Iranian study. 21 This finding can be explained by the large proportion of the women reviewed in this study (85.5%) —just like other similar studies in Nigeria4, 5,11—who had hysterectomies via the abdominal route, which is known to be associated with higher perioperative complications and longer hospital stay compared to VH.18,22,23
The mortality rate of 0.12% reported from the current study was quite similar to the figures reported by Wright et al., 24 although their study only looked at women who underwent abdominal hysterectomy. However, the mortality rate in the current study was significantly higher than rates reported from most Western countries 25 that looked at overall mortality from all types of hysterectomies as was done in the current study. Thus, this suggests that hysterectomy-related mortality from the Lagos center may be unduly high, most likely as a result of the fewer number of vaginal and laparoscopic hysterectomies performed, compared to the trends seen in most of the Western countries.
The limitation in this study was the poor medical recordkeeping system in the hospital (study setting), which affected accurate data collection, as some case notes could not be retrieved for the study.
Conclusions
The current study demonstrated that the rate, common indications, and pattern of perioperative complications for elective hysterectomy has remained largely unchanged over the last decade in Nigeria. However, there was a reported reduction in the annual rate of VH. Therefore, there is an urgent need to fortify the current postgraduate specialist-training curriculum as a way to improve the skills of future gynecologists so that they can perform less-complicated surgical procedures, such as VH to reduce morbidities and improve the overall outcome for Nigerian women.
Footnotes
Acknowledgments
The authors appreciate the assistance given by all the medical records staff of the LUTH and the resident doctors of the LUTH's Department of Obstetrics and Gynaecology.
Author Disclosure Statement
The authors declare no conflicts of interest in carrying out this study.