
Abstract
Abstract
Background:
Pregnancy in the rudimentary horn of a unicornuate uterus is an extremely rare obstetric complication and usually results in rupture in the second trimester, with an acute clinical presentation. The authors present a rare case of a ruptured rudimentary horn pregnancy (RHP) without classical hemoperitoneum.
Case:
A 22-year-old primigravida at 21 weeks gestation was referred as a case of intrauterine fetal death. Magnetic resonance imaging indicated a possible rudimentary horn rupture.
Results:
Intraoperatively, it was noted that there was a ruptured right RHP with a macerated fetus, and 100 cc of clotted blood was contained in a pseudosac formed by the surrounding viscera and peritoneum. After surgical intervention, the patient had an uneventful postoperative period.
Conclusion:
A ruptured RHP can occur unexpectedly with stable hemodynamics. (J GYNECOL SURG 34:43)
Introduction
P
Case
A 22-year-old female primigravida at 21 weeks of gestation was referred to the authors' obstetric unit as a case of intrauterine fetal death that was diagnosed on ultrasound (US) after one day of spotting. At admission, the patient's pulse was 98 beats per minute and her blood pressure was 110/60 mm Hg; she had no pallor. Her abdomen was soft and uterine height corresponded to 20 weeks of gestation with an absent fetal-heart sound. A vaginal examination revealed a closed cervical os, and although the uterus appeared to be retroverted, the fetal bulk was felt anteriorly. An US test raised the suspicion of an extrauterine pregnancy and a magnetic resonance imaging (MRI) scan was performed for confirmation. The MRI indicated a possible rudimentary horn rupture. However, this indication was doubtful as, on one hand, the uterine musculature of the rudimentary horn was deficient around the fetus, suggesting a rupture, while, on the other hand, there was no hemoperitoneum, which classically accompanies a ruptured RHP. In addition, the fetus was in a well-defined amniotic sac (Figs. 1 and 2). A decision to perform a laparotomy was made, and the mystery surrounding this case unfolded.
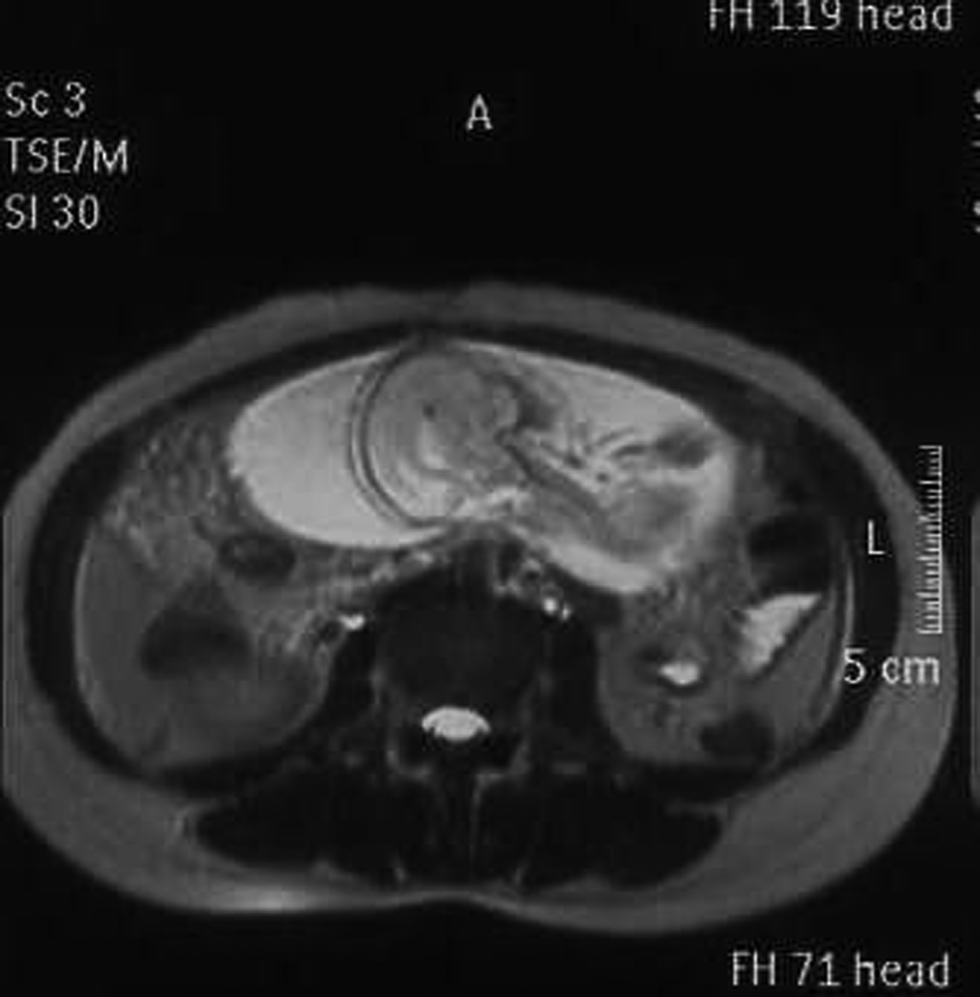
Horizontal view of magnetic resonance imaging of a rudimentary horn pregnancy with the fetus in a well-defined amniotic sac without hemoperitoneum.
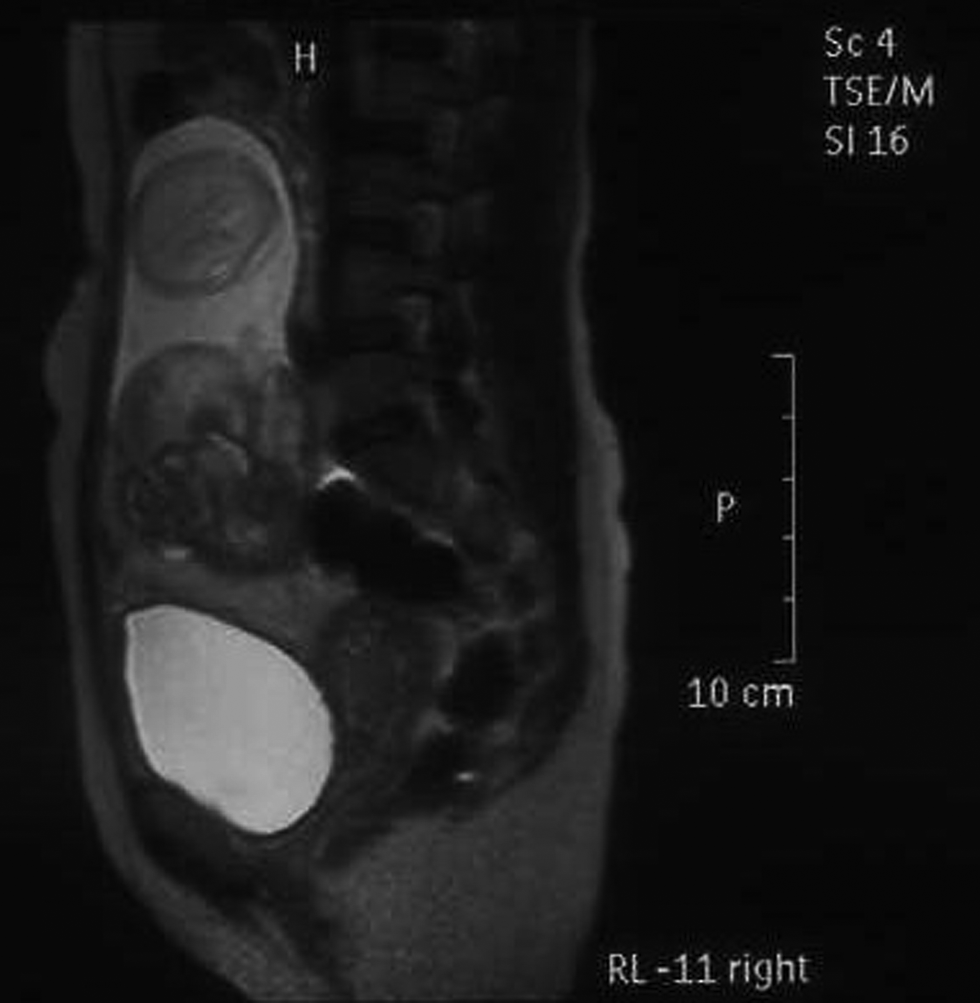
Vertical view of magnetic resonance imaging of a rudimentary horn pregnancy with the fetus in a well-defined amniotic sac without hemoperitoneum.
Results
Intraoperatively, it was noted that there was a ruptured right RHP (Fig. 3), but the classic hemoperitoneum was missing. A macerated fetus and only 100 cc clotted blood were contained in a pseudosac formed by the surrounding viscera and peritoneum (Fig. 4). Excision of the rudimentary horn, along with the attached placenta and fetus, and ipsilateral salpingectomy were performed. The patient's postoperative period was uneventful.

Intraoperative view of right-sided ruptured horn along with the fetus and placenta.

Fetoplacental unit encysted with surrounding viscera.
Discussion
Rudimentary horn with a unicornuate uterus results from failure of complete development of one of the Müllerian ducts and incomplete fusion with the contralateral side. The incidence of Müllerian-duct malformations in the general population is estimated to be 4.3%, while that of unicornuate uteri is ∼0.4%. 2 The most likely mechanism of a pregnancy in a noncommunicating rudimentary horn is transperitoneal migration of the spermatozoa. Fifty percent of the pregnancies rupture, usually in the second trimester, while 30% go to term with a 0%–13% fetal salvage rate. 1 This poor obstetric outcome could be due to the abnormal shape of the uterus, insufficient muscular mass of the uterus, abnormal vasculature, cervical incompetence, and reduced uterine volume and inability to expand. Various studies have reported live birth rates ranging from 29% to 61%.3–5
Ruptured RHP results in massive hemorrhage, and the mortality rate is 5%. 6 However, in the current case, despite the rupture, the clinical presentation was not of hypovolemic shock due to the encystment of the ruptured horn and fetoplacental unit by the surrounding viscera. A similar presentation of a ruptured RHP was encountered by Shergill et al. 7 Hemodynamic stability in such cases can lead to a diagnostic dilemma and a delay, thereby increasing morbidity and mortality. Herein lies the importance of diagnostic imaging modalities. Sonographic diagnostic criteria, suggested by Tsafrir et al., are the presence of a pseudopattern with an asymmetrical bicornuate uterus, no visual continuity between the cervical canal and the lumen of the pregnant horn, and the presence of myometrial tissue surrounding the gestational sac. 8 However, the sensitivity of US is only 26%, and it decreases as the pregnancy advances. 9 Tubal pregnancy, cornual pregnancy, intrauterine pregnancy, and abdominal pregnancy are common sonographic misdiagnosis. 10 In the current case US was also inconclusive and MRI clinched the diagnosis. MRI is also useful for excluding any abnormal placentation, as chances of placental adherence are increased due to poorly developed musculature and scant decidualization. Over last few years, cases of pregnancies in rudimentary horns have been managed laparoscopically. 11 Prerupture diagnosis is indeed challenging but, when possible, medical management with methotrexate is an option, although surgical excision of the horn is still recommended. 12
Conclusion
A ruptured RHP could present unexpectedly with stable hemodynamics.
Footnotes
Author Disclosure Statement
No funding was provided for the preparation of this article. There are no conflicts of interest.