
Abstract
Abstract
Objective:
The aim of this article is to describe a hysterectomy technique for managing selected difficult cases of placenta accreta.
Background:
Cesarean hysterectomy for placenta accreta is associated with a significant amount of maternal morbidity. Intraoperative hemorrhage and urinary-tract injury are some of the more-frequent complications encountered. Most women with placenta accreta have undergone at least one prior cesarean delivery, increasing the risk of adhesions and scar tissue.
Results and Conclusions:
The current authors' technique for an extended hysterectomy in selected high-risk cases of placenta accreta/percreta is designed to reduce the risk of hemorrhage and urinary tract injuries. (J GYNECOL SURG 34:133)
Introduction
T
To reduce the likelihood of hemorrhage and urinary tract injury during hysterectomy for placenta accreta, the surgical technique used should include early and thorough mobilization of the bladder, traction of the uterus and countertraction of the anterior soft tissues, and tight control of the pedicles against the uterus. Avoiding any type of placental trauma is quite important, as even minor placental trauma may lead to massive hemorrhage; however, it might not always be possible to avoid such trauma, especially if the placenta is located anteriorly and impinges on the site of the hysterotomy.
Cesarean hysterectomy for a deeply invading placenta is inherently more difficult than other elective cesarean hysterectomies, as it is necessary to maintain a safe margin away from the vascular cervical–placental mass and to protect the urinary tract. As the urinary tract must be mobilized without invading the plane of the placenta,1,4 the operation now assumes features of a modified radical hysterectomy (Fig. 1).
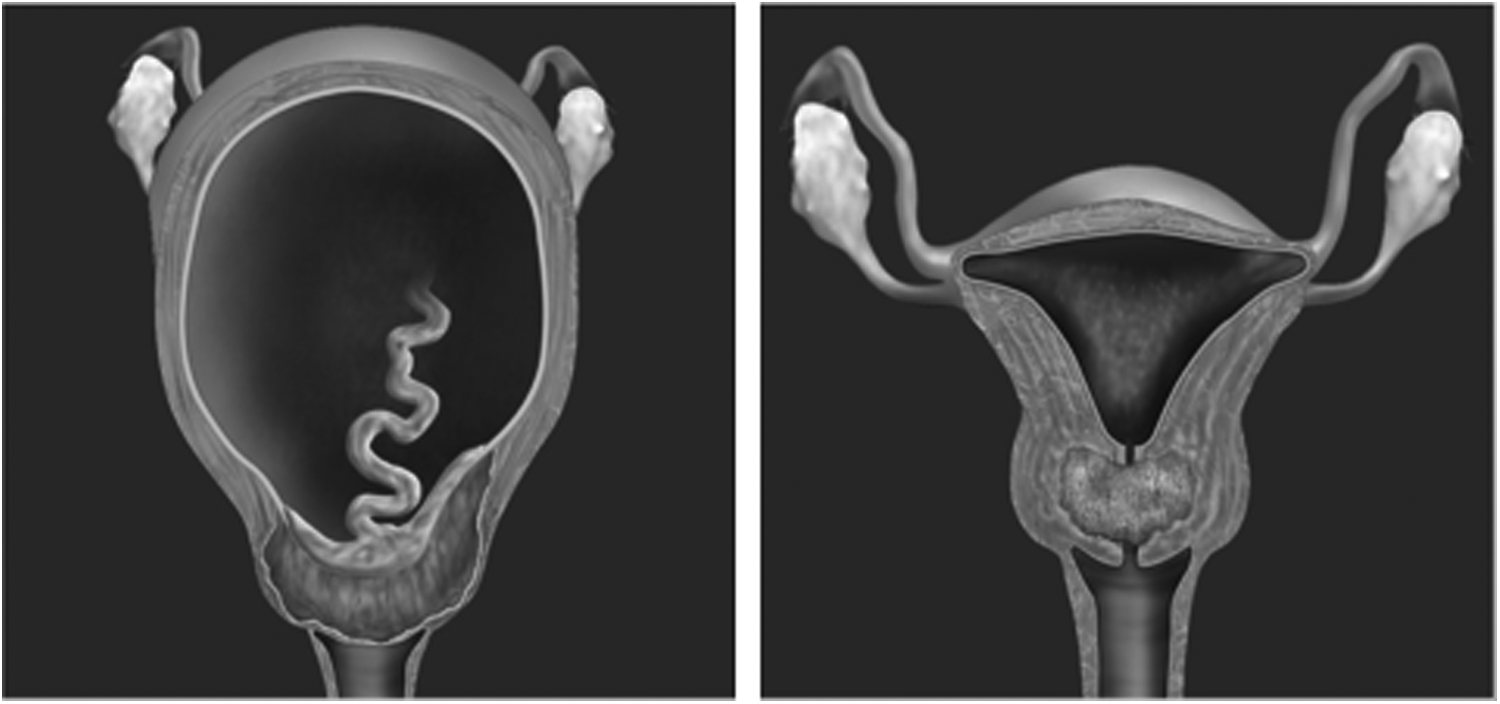
A barrel-shaped cervical cancer (left) and a placenta previa–accreta (right) have similar anatomical configurations and surgical approaches to treatment.
The surgical care of such patients has many critical elements that have been well-described in the literature.5–9 The current authors' protocol for management of suspected placenta accreta is shown in Box 1. This report is confined to the technique of complex hysterectomy for patients with high-risk cases of placenta accreta as described above.
1. Suspected accreta (>1 cesarean section + previa + suspicious sonogram image) —> evaluation/sonography by maternal–fetal medicine (MFM).
2. Team approach and planning pre- and intraoperatively involves MFM, gynecologic oncology, anesthesia, interventional radiology (IR), neonatology, nursing, blood bank, and urology (for selected cases):
3. Elective cesarean section 34–36 weeks (steroids):
• Ureteral stents
• Pre- and intraoperative ultrasound mapping of placenta to avoid it during cesarean section
• Abdominal incision limited to that needed for cesarean section
• Delivery needs to be as atraumatic as possible to avoid placental disruption
• Pitocin after delivery
• Patient decision for definitive treatment, surgically straightforward as determined by imaging and intraoperative findings, or hemorrhage —> leave placenta in place; modified radical hysterectomy (placenta must not be disrupted by manipulation or division of tissues)
• For selected cases (questionable accreta), allow time for placenta to deliver; utilize great caution regarding any attempt at gentle traction (the decision for this may be aided with intraoperative ultrasound in selected cases)
4. For patient who has desire to retain childbearing capacity, understands risks, and has no significant active bleeding —> leave placenta in place, close uterus, and monitor closely a
5. “High-risk” cases include increta/percreta as determined by imaging and/or intraoperative findings that involve the cervix, region of the bladder trigone, and/or extensive portion of bladder; morbid obesity is a relative risk factor; extension of the placenta into the broad ligament is also a relative risk factor that is best assessed intraoperatively in terms of potential operative difficulty:
• Hybrid suite (when available)
• Ureteral stents (positioning for this is suboptimal in the current authors' hybrid suite)
• Balloon-tipped internal iliac artery catheters placed by IR
• Cesarean section as described above
• Anticipated significant surgical difficulty (hemorrhage, urinary tract) and definitive treatment planned —> divide round ligament and isolate and staple utero-ovarian pedicle (fallopian tube, utero-ovarian ligament, vascular anastamosis) bilaterally; this facilitates embolization; then bring IR back in (or move patient back) to perform thorough embolization; balloons might need to be inflated during transition if hemorrhage occurs
• Following embolization, the decision for hysterectomy versus leaving uterus/placenta is made on an individualized basis (surgical difficulty, anticipated urinary-tract morbidity, available surgical team and transfusion capabilities, general patient factors such as reliability and access to care, and hemostasis) b
• If hysterectomy, inflation of balloons may be considered on an individualized basis
• If a high-risk patient has a desire to retain childbearing and there is no hemorrhage after cesarean section, do not staple utero-ovarian pedicle; embolization may still be considered on an individualized basis c
Note: If uterus/placenta is left in place, there is a significant risk for subsequent hemorrhage and/or infection. These patients may have several months of spotting and cramping pain. They should be at pelvic rest during this time. They should not have pelvic examinations or transvaginal sonography without good reason. However, it is not uncommon for these patients to require subsequent hysterectomy for hemorrhage and/or infection, sometimes emergently. Other management options (embolization, uterotonics, dilation and curettage, or hormonal manipulation) must be highly individualized. The role of prophylactic antibiotics in these patients is unknown, but a short course might be considered in certain patients (known sexually transmitted disease, Streptococcus B, etc.). There is not good evidence for utilization of methotrexate in these patients and the current authors do not use it.
Note: If uterus/placenta left in place following embolization, a patient will experience postembolization syndrome (2–3 days of fever, pain, and leukocytosis). This can be confusing, given the concern for infection.
Note: If embolization is not feasible or risk assessment does not appear to warrant it, internal iliac artery catheters with inflation of balloons as needed may be considered as an adjuvant/safeguard. Catheters are placed prior to cesarean section, and balloons are inflated if hemorrhage occurs or for an attempt to reduce blood loss during hysterectomy. These catheters may be left in place for short durations in selected cases when subsequent possible need for embolization is anticipated.
Technique of Complex Hysterectomy
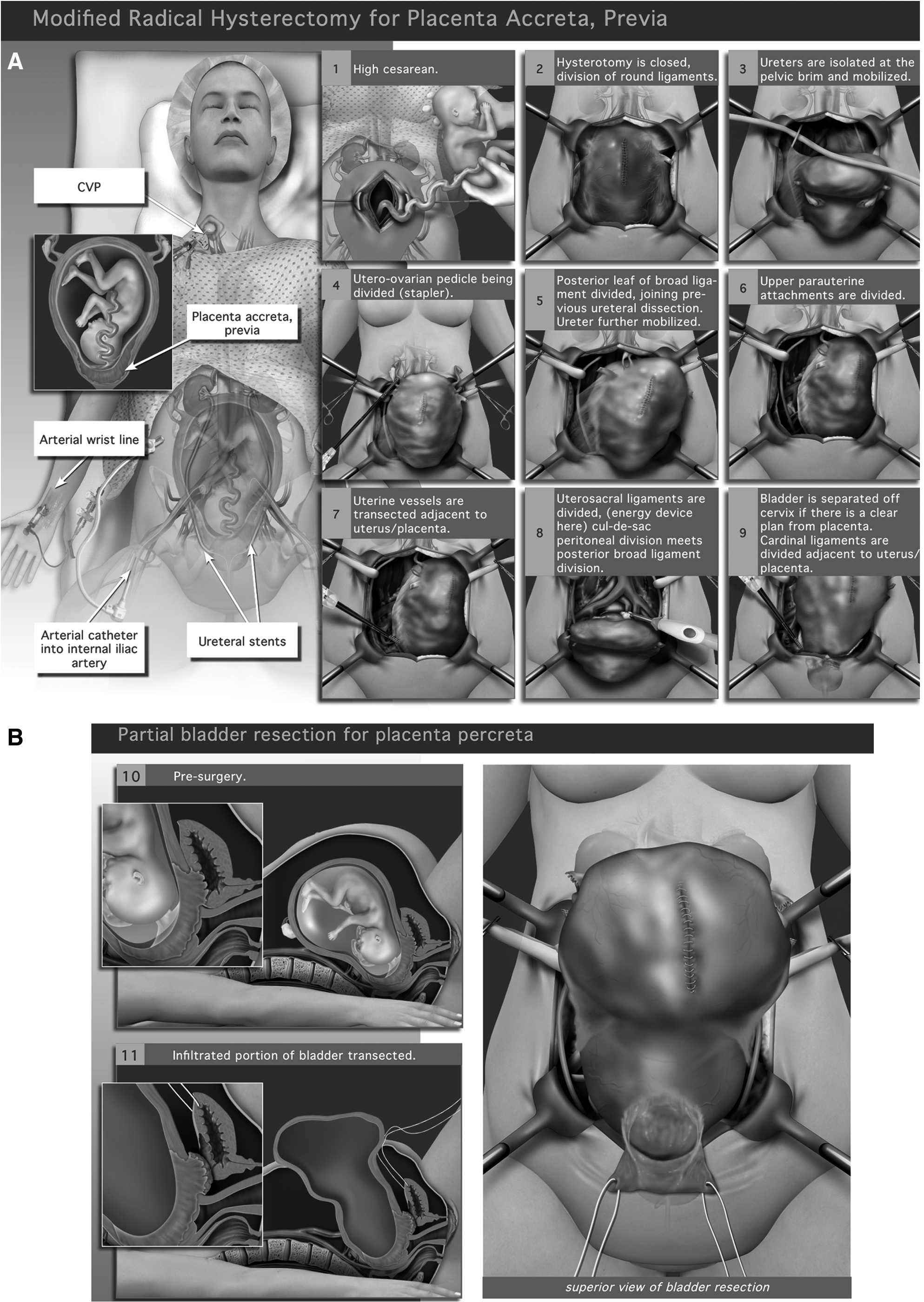
General anesthesia is preferred, due to the potential for rapid hemorrhage requiring prompt surgical control. The patient is placed in a low lithotomy position. This allows ready access to the perineum and an additional surgeon at the operative field (Fig. 2A). The laparotomy incision should be placed to enable a high hysterotomy and subsequent exposure above the enlarged uterus as well as to the deeper regions of the pelvis. Initially, the scarred pelvic portion of the incision is left undissected in order to mitigate damage and placental trauma and to expedite delivery.
Limited data suggest that ureteral stents help avoid ureteral injury in the management of high-risk cases of placenta accreta. 1 It is hazardous to dissect the ureters from the markedly vascular parametria. Although ureteral stents do not always prevent ureteral injury, it is easier to recognize. Furthermore, it has been the current authors' experience that frequent palpation of the stents during hysterectomy precludes the necessity for more extensive dissection. Placement of the stents prior to delivery is more controlled but could require an additional anesthetic. The stents may be placed while the cesarean section is being performed or just after delivery. The bladder is inspected for the presence and location of placental invasion.
It is imperative that the hysterotomy incision avoids the placenta, and this generally requires a fundal incision; its placement may be aided by a preincision ultrasound scan (Fig. 2A1). Delivery of the neonate should be accomplished without manually disturbing the placenta. Manual delivery of the placenta should be avoided (Supplementary Video S1; Supplementary Data are available online at www.liebertpub.com/gyn).
If needed to obtain hemostasis, the uterine incision may be closed with a single layer of #2 polypropylene running-locked suture or approximated with towel clamps that may be used later for traction.
Most women with placenta accreta will have undergone prior cesarean sections, and extensive scarring of the lower uterus segment and adhesions of the anterior cul-de-sac to the abdominal wall are common. Dissecting the retropubic space and skirting lateral to the bladder avoids injury to the bladder and affords the maximum deep pelvic exposure. A self-retaining retractor is then placed, and the sigmoid colon and cecum are mobilized to enable packing that will maximize pelvic exposure.
Great care is taken to maintain tight control of the vascular pedicles, and to avoid any transgression into placental tissue and/or maneuvers such as excessive traction or rocking the uterus anteriorly that could fracture the placenta.
The round ligaments are divided lateral to the utero-ovarian vascular anastomoses and dissected toward the uterus (Fig. 2A–2). The ureters are isolated at the pelvic brim above the uterus and held with vessel loops (Fig. 2A–3). After locating an avascular window under the utero-ovarian ligament, the utero-ovarian pedicle is divided (Fig 2A–4). A vascular stapler may be used, due to the length and highly vascular nature of the pedicle and the proximity of the ovary, as well as for control of back-bleeding. Obviously, familiarity with this device and the various sizes of staple loads is required.
The posterior leaves of the broad ligaments are incised, taking great care to skirt the uterine vasculature. These incisions are extended across the posterior peritoneal reflection to meet the isolated ureters (Fig. 2A-5). The ureters are mobilized laterally carefully until the ureteric tunnels are reached. Typically, long Kelley clamps are placed tightly against the uterine fundus for the purposes of traction and control of back-bleeding.
The anterior leaves of the broad ligament are divided toward the reflection of the bladder. Typically, the broad ligaments are elongated and largely avascular, and can be divided with cautery dissection (Fig. 2A-6). In most cases, the bladder may be mobilized cautiously from the lower uterine segment and cervix. At this juncture, a bladder that is densely adherent or attached immediately over apparent placental tissue can be encountered. In such cases, it is prudent to delay any attempt to separate the bladder until additional uterine devascularization is accomplished and the boundaries of the bladder scar and/or placental invasion are defined better.
When the bladder is dissected out of harm's way, the uterine vessels are then divided against the uterus (Fig. 2A-7). Again, the use of a vascular stapler could have some advantages over the standard clamp-and-ligature technique. Due to the markedly expanded lower uterine segment, the ureters will be in close proximity (the stented ureter can usually be palpated). For this reason and for hemostatic control, it is important to keep the stapler or clamp tightly against the uterus—but in the “extra fascial plane” so as to avoid disruption of the placenta. A useful maneuver to accomplish all of these goals is (with slight upward and contralateral traction on the uterus) to grasp the lateral tissue to be divided with the thumb and forefinger, pinching immediately adjacent to the uterus so that all of the urinary tract–bearing tissue is pulled laterally and the pedicle is made “tight.” At the same time, the tips of these fingers push the stapler (or clamp) firmly against the uterus, adjusting the angle as appropriate. Division of the cardinal ligament is similarly carried to the cervicovaginal junction (Fig. 2A-8). It is often helpful to divide the uterosacral ligaments seperately to isolate and devascularize the uterus (Fig. 2A–9) more completely. Delineation by pressure with a sponge stick in the vagina is useful.
The cervicovaginal junction is then transected and the vaginal cuff is closed hemostatically with a running-lock suture or with a roticulating stapler that fires an absorbable load of staples across the vagina.
Following removal of the uterus, a substantial volume of “raw” pelvic floor remains and might contribute to postoperative hemorrhage. At least partial reperitonealization (over hemostatic agents if deemed necessary) that incorporates vascular pedicles cautiously and the closed vaginal cuff may help prevent this event. A closed suction drain is placed at the discretion of the surgeon.
Placenta Percreta with Bladder Invasion
Placenta percreta with bladder invasion deserves special comment. This condition might be suspected preoperatively (based on imaging and, occasionally, hematuria) and/or intraoperatively (cystoscopy and/or gross invasion of placenta into the bladder muscularis). When the diagnosis is suspected and the placenta appears to be encroaching on the bladder muscularis, the surgeon should assume that placenta percreta is present. In selected cases (e.g., anticipated loss of a large portion of the bladder, unusual surgical difficulty) consideration is given to leaving the placenta in place. 10 Attempts to separate the bladder from the uterus and cervix in this instance (even in the absence of overt bladder invasion) could result in massive hemorrhage.
Placenta percreta usually involves the lower uterine segment and the mid-posterior dome of the bladder (Fig. 2B-10). It is important to devascularize as much of the uterus as possible before approaching this region and to avoid traction or any other type of trauma to this region until it is planned. It is almost always possible to open an avascular space (medial to the umbilical ligaments) bilaterally that separates the bladder from the parametrial and paracervical tissues. To a limited extent, the ureters will be mobilized laterally with this maneuver but will still potentially be in harm's way (especially distally). Following development of these spaces, the uterine vessel pedicles are stapled just lateral to the uterine–placental mass. The uterosacral ligaments are defined and divided (a bipolar energy device works well here) just outside the margin of the cervix–placental mass as described above. If ureteral stents are in place and the surgeon can develop the space between the paracervical tissues and the urinary tract confidently, then these ligaments are stapled as well. Blunt digital dissection of the bladder from cervix caudal to the area of adherence is often possible, 4 and transection of the vaginal fornix at this point can be considered (with a stapler if it can be isolated or, alternatively, approached through the posterior vaginal wall).
Because the surgeon is able to get more distal in the progress of the hysterectomy, approaching the adherent urinary tract becomes safer and defined better. Surgical management of the adherent, vascular region of the urinary tract can then proceed as indicated by the gross findings and judgment of the surgeon (i.e., separation versus resection). If there is loss of a clear plane of separation between a deeply invading placenta and the bladder, the surgeon must err on the side of leaving detrusor muscle or a full thickness disc of bladder transected to the uterine specimen.
Next, the surgeon should approach the unscarred spaces on either side (or potentially caudal to) of the region of bladder involvement, transect the distal paracervical tissues, and enter into the bladder immediately cephalad to the invaded (or densely adherent) portion (Fig 2B-11a,b). The surgeon is then in a position to resect only the well-delineated (and usually disc-shaped) segment of involved bladder (Fig. 2B-11b). The cesarean hysterectomy is then completed, followed by repair of the bladder.
Footnotes
Author Disclosure Statement
The authors have no conflicts of interest to report.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.