
Abstract
Abstract
Background:
Primary vaginal small-cell neuroendocrine carcinoma (VSC) is extremely rare and is associated with a poor prognosis. Treatment of VSC differs by institute, and optimal treatment strategies remain unclear.
Case:
A 54-year-old woman, who had a surgical history of hysterectomy due to myoma at the age of 37, was diagnosed as having VSC carcinoma. Her staging was designated as AJCC [American Joint Committee on Cancer] pathologic stage III (T1 N1 M0). Concurrent chemoradiation therapy (CCRT) with interstitial irradiation was selected for the treatment.
Results:
After CCRT, she did not show any evidence of recurrence.
Conclusions:
CCRT with interstitial irradiation was effective for treating VSC carcinoma in an advanced stage.
Introduction
V
Case
A 54-year-old woman who had a surgical history of hysterectomy, due to a myoma she had at age 37, visited a nearby hospital due to abnormal vaginal bleeding, where she underwent loop electrosurgical excision procedure (LEEP) coagulation for hemostasis. Two months after the LEEP coagulation, she visited the Juntendo University Faculty of Medicine, Tokyo, Japan, due to recurrence of her vaginal bleeding. On examination, a 1.5-cm mass was observed and removed for biopsy. Hematoxylin and eosin (H&E) stained sections showed the tumor was composed of packed, small round cells with scanty cytoplasm and indistinct cell borders; the cells were arranged in small nests or formed cords (Fig. 1A and B). Immunohistochemical analysis results were negative for chromogranin A, synaptophysin, and thyroid transcription factor-1; strongly diffusely positive for CD56 and cytokeratin 7 (CK7); and weakly positive for p16 (Fig. 1C–E). The tumor was diagnosed as a small-cell carcinoma based on this histology.
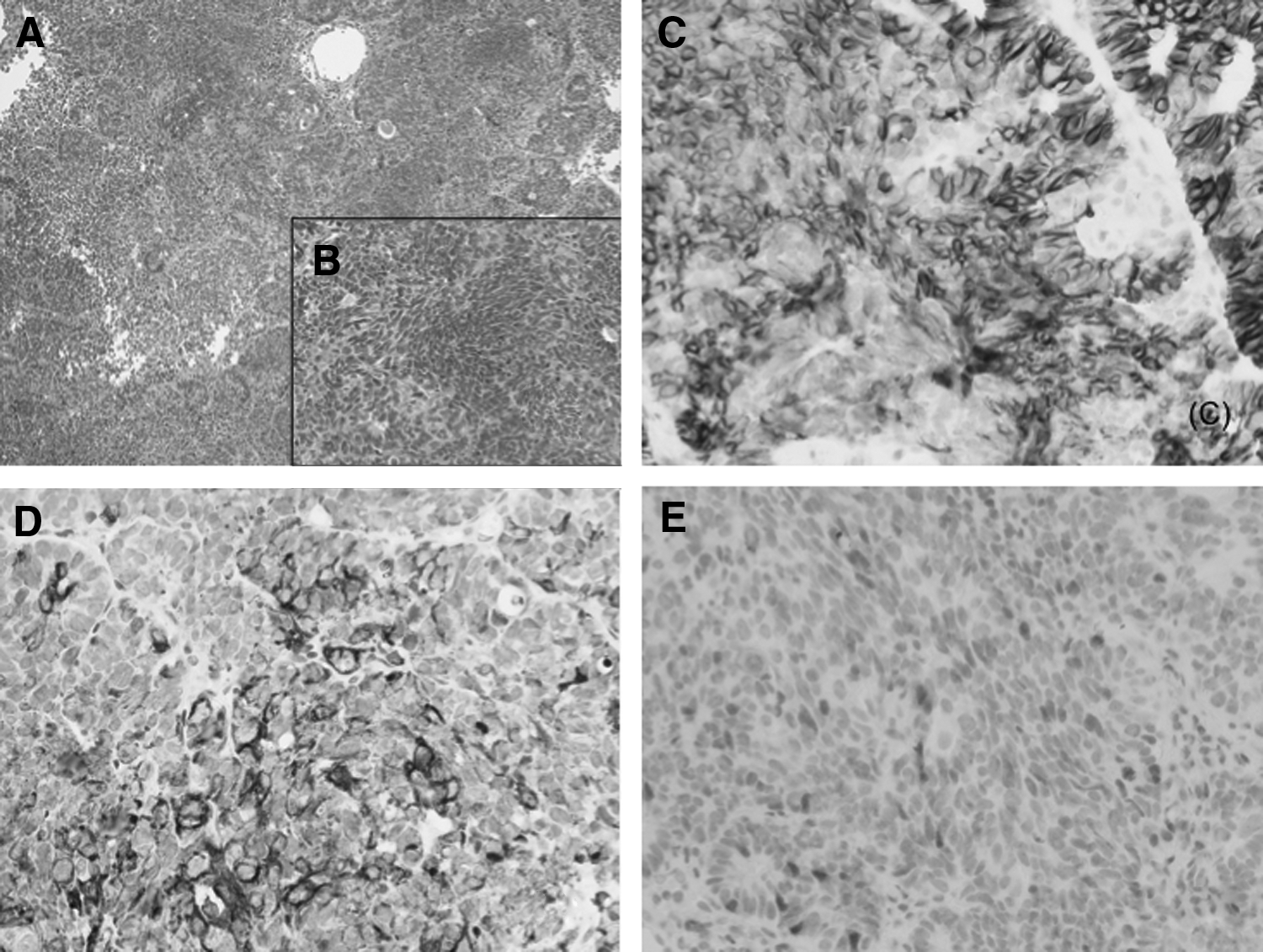
Pathologic findings.
Magnetic resonance imaging showed a 1.5-cm mass at the vaginal stump (Fig. 2A). Positron emission tomography showed fluorodeoxyglucose accumulation in the same area (SUVmax 21.9) and in the left external iliac lymph nodes (SUVmax 2.4) (Fig. 2B and C). The tumor markers carcinoembryonic antigen, cancer antigen–125, squamous-cell carcinoma antigen, and neuron-specific enolase were negative. The tumor was determined to be stage III (cT1N1M0), and CCRT with interstitial irradiation was selected for treatment. Extended-field radiation therapy (RT) and brachytherapy were delivered with chemotherapy (40 mg/m2 of cisplatin [CDDP] every week for 5 cycles).

Tumor appearance.
Results
The patient did not show any evidence of recurrence 12 months after the CCRT.
Discussion
CCRT with interstitial irradiation was effective in the current patient, who had advanced-stage VCS. Primary VCS is extremely rare, with only 24 cases reported in the English literature (Table 1).1–16 Of these 24 patients, 5 (20.8%) showed no evidence of disease (NED), although only 1 of these 5 patients experienced long-term survival. Furthermore, only 3 (60%) of 5 patients with stage I disease showed NED. These results indicate that VCS is associated with an extremely poor prognosis.
TNM, tumor, node, metastasis; RT, radiation therapy; CT, chemotherapy; BT, brachytherapy; CCRT, concurrent chemoradiation therapy.
Of the 24 cases of VGS cited in the literature, 6 underwent CCRT, 4 of which showed complete responses; furthermore, 2 cases had NED. In 4 cases, chemotherapy consisted of combination cisplatin and etoposide; 1 patient received cisplatin alone; and 1 patient received combination carboplatin and etoposide. Of the 6 patients who received CCRT, 4 received combination external RT and brachytherapy, 2 of whom had NED. Of the 2 cases who received surgery alone, all died due to disease, suggesting that poor tumor control is achieved by surgery alone, so combination treatment with surgery, chemotherapy, and/or RT is recommended. All 5 patients who lived for >12 months received combination RT and chemotherapy. In the present case, CCRT was selected; it consisted of weekly CDDP, external RT, and interstitial brachytherapy, to enhance local tumor reduction.
Kanayama et al. reported that, for primary vaginal cancer, external-beam RT with brachytherapy (interstitial or intracavitary) should be used as definitive RT regardless of International Federation of Gynecology and Obstetrics stage. 17 With respect to RT for treating vaginal cancer, the American Brachytherapy Society consensus guidelines include recommendations for interstitial brachytherapy in patients with vaginal cancer. 18 These guidelines recommend that patients with bulky disease (∼ > 0.5 cm thick) should be considered for treatment with interstitial brachytherapy. The criteria for interstitial brachytherapy for vaginal cancer are established by each institution due to the technical difficulty of this treatment. In the present case, during CCRT, the swollen pelvic lymph node disappeared due to external RT and the vaginal tumor disappeared due to interstitial brachytherapy.
Conclusions
Although the current patient has not shown any evidence of recurrence 12 months after CCRT, it is necessary to be aware that the length of follow-up does not predict long-term survival, according to the literature review presented here. To the current authors' knowledge, this is the first report about the efficacy of CCRT using interstitial brachytherapy for primary VSC: CCRT (daily CDDP plus external RT) and interstitial irradiation were effective for this patient who had advanced-stage VSC.
Footnotes
Author Disclosure Statement
The authors declare that there are no conflicts of interest.