
Abstract
Abstract
Objectives:
Ovarian carcinosarcomas are rare and aggressive ovarian malignancies. The objective of this study was to examine the current authors' experiences with optimal cytoreductive surgery (CRS) and platinum-based chemotherapy for managing ovarian carcinosarcomas.
Materials and Methods:
A retrospective study was carried out on 20 patients who had ovarian carcinosarcoma (OCS) and who underwent primary surgery at the Rajiv Gandhi Cancer Institute and Research Centre, in Delhi, India, from January 2004 till December 2016.
Results:
Complete cytoreduction to no gross residual disease was achieved in 14 patients, 10 patients had heterologous histologies with sarcomatous components, and 13 patients had advanced stage (stages III and IV) disease. Fifteen patients received platinum-based adjuvant chemotherapy. Follow-up periods ranged from 15 days to 82 months. After primary surgery, 9 patients developed recurrences and 4 had progressive disease. Ten patients died of disease during the follow-up period. The 3-year disease-free survival was 33%, and the 3-year overall survival (OS) was 40.52%. Homologous histology with sarcomatous components and optimal CRS were associated with significant improvements in OS, in a univariate analysis. However, in a multivariate analysis, only optimal surgery retained significance.
Conclusions:
Radical surgery resulting in no visible disease, followed by platinum-based chemotherapy appears to improve outcomes and survival in patients with OCS.
Introduction
Ovarian carcinosarcoma (OCS) is a rare and aggressive variant of ovarian cancer, accounting for 1%–4% of all ovarian malignancies.1,2 Patients are usually diagnosed at ages 50–70. About 75% patients present at International Federation of Gynecology and Obstetrics (FIGO) stages III or IV.2,3 Prognosis is poor, with a median overall survival (OS) time ranging from 8 to 32 months.2,4–6 The treatment of OCS is largely based on small retrospective studies or extrapolations from research on epithelial ovarian cancer (EOC), which has identified the benefit of aggressive surgical cytoreduction and platinum-based chemotherapy. The aim of the current study was to identify clinicopathologic features of OCS that could predict the survival outcome, with special emphasis on the role of optimal cytoreductive surgery (CRS).
Materials and Methods
After obtaining institutional review board approval, the records of all patients treated for OCS, from January 2004 to December 2016—at the Rajiv Gandhi Cancer Institute and Research Centre, in Delhi, India—were reviewed. All pathology reviews were performed by the gynecologic pathologists at this institute at the time of the patients' initial treatments. The patients' demographic characteristics, symptoms, intraoperative findings, histopathologic reports, surgical optimal or suboptimal debulking status, chemotherapeutic regimens administered, and survival lengths were all reviewed. Patients were restaged according to the FIGO 2014 staging system for ovarian cancer. Disease-free survival (DFS) was calculated from date of primary surgery to date of recurrence or last follow-up. Four patients had progressive disease after suboptimal surgery and were not included in calculating DFS. Only patients with a follow-up period of more than 6 months were included in DFS analysis, thus excluding 1 patient with a follow-up period of 6 months. All 20 patients were included in calculating OS. OS was calculated from the date of primary surgery to the date of death or last follow-up. Survival curves were generated by the Kaplan–Meier method and compared with a log-rank test. A p-value of <0.05 was considered to be significant.
Results
The mean age of the patients was 52.9 ± 12.3 years (range: 28–68 years). Seven patients were nulliparous, and 13 patients were postmenopausal. The presenting symptoms were: abdominal pain (8 patients); abdominal distension (6 patients); postmenopausal bleeding (2 patients); abdominal mass (2 patients); and fever (1 patient). One patient's cancer was incidentally detected during her caesarean section. Preoperative cancer antigen (CA)–125 levels were elevated in 17 patients. The median CA-125 level was 201 U/mL (range: 11–2850 U/mL). Preoperative tissue diagnoses of ovarian carcinosarcomas were already made in 8 patients by biopsy from pelvic masses (3 patients), exploratory laparotomies followed by omental/ovarian biopsies (4 patients), and by a total abdominal hysterectomy and bilateral salpingo-oophorectomy (TAH+B/L SPO; 1 patient). The slides were reviewed by a gynecologic pathologist and diagnosis was confirmed at the institute. Two patients received neoadjuvant chemotherapy (NACT) at another facility; 1 patient had 3 cycles of paclitaxel, ifosfamide & cisplatin (TIP); and another patient had 3 cycles of paclitaxel and carboplatin (PC).
All 20 patients underwent surgical staging and debulking at the institute. TAH+B/L SPO was performed in 18 patients, and 2 patients underwent fertility-sparing surgery (B/L SPO in 1 patient and left SPO and right ovarian biopsy in 1 patient). Other surgical procedures performed were: B/L pelvic-lymph node dissection (16 patients); omentectomy (18 patients); appendectomy (8 patients); removal of enlarged retroperitoneal lymph nodes (8 patients); and collection of fluid for cytology testing (15 patients). The following procedures were performed to achieve complete debulking: peritonectomy (4 patients); removal of deposits on sigmoid and rectum (4 patients); large-bowel resection anastomosis (2); inguinal-node dissection (1 patient); and removal of a segment of involved ileum with the pelvic mass followed by ileo–ileal anastomosis and loop ileostomy (1 patient).
Optimal debulking was achieved in 15 patients (complete cytoreduction in 14 patients and the largest residual tumor <1 cm in 1 patient). Four patients with stage IIIC and 1 patient with stage IV disease had residual disease >1 cm at the completion of primary surgery.
On histopathology testing, the epithelial components were: high-grade serous (15 patients); low-grade endometrioid (2 patients); grade 3 endometrioid (1 patient); mixed high-grade serous carcinoma and clear-cell carcinoma (1 patient); and poorly differentiated carcinoma (1 patient). The sarcomatous components were homologous in 10 patients. The heterologous components were: chondrosarcoma (7 patients); rhabdomyosarcoma (1 patient); mixed chondrosarcoma and rhabdomyosarcoma (1 patient); and mixed chondrosarcoma, osteosarcoma, and rhabdomyosarcoma (1 patient).
Peritoneal fluid was positive in 6 patients, pelvic lymph nodes and retroperitoneal lymph nodes were positive in 4 patients each, and omentum was involved in 9 patients, while the appendix was involved in 2 patients. Four patients (20%) had stage I disease, 3 patients (15%) had stage II disease, 11 patients (55%) had stage III disease, and 2 patients (10%) had stage IV disease. For the 2 stage 1V patients, pleural fluid was positive for malignant cells in 1 patient while the inguinal node was involved in the other patient. All patients with early stage disease (stages I and II) had optimal debulking status (100%), while 8/13 (65%) of patients with advanced-stage disease (stages III and IV) had optimal debulking (p = 0.023; Fisher's exact test).
Thirteen patients received 6 cycles of adjuvant chemotherapy (TIP for 4 patients and PC for 9 patients). Two patients received 3 cycles as NACT and 3 cycles as adjuvant chemotherapy (TIP for 1 patient and PC for another patient). One patient was kept on follow-up in view of her early stage disease after a tumor-board discussion. Two patients could not receive chemotherapy due to having poor general conditions. Two patients received just 1 cycle of single-agent chemotherapy (ifosfamide for 1 patient and carboplatin for another patient) as they died due to progressive disease before the second cycle could be given. Patients with suboptimal CRS were less likely to receive adjuvant chemotherapy due to early postoperative death (p = 0.001; Fisher's exact test).
The mean follow-up period was 28.8 months (range: 15 days to 82 months). Recurrences developed in 9 patients, and 4 patients had progressive disease after surgery. Ten patients died of recurrent/progressive disease. The median time to develop a recurrence was 11 months (range: 3–36 months). Six patients with recurrent disease underwent secondary CRS and complete cytoreduction was achieved in these patients. To achieve complete cytoreduction, procedures that were performed were: small-bowel resection anastomosis (2 patients); right hemicolectomy with ileo-transverse anastomosis (1 patient); low anterior resection with colorectal anastomosis (1 patient); removal of perihepatic deposits (2 patients); retroperitoneal lymph-node dissection (2 patients); removal of vault mass (2 patients); peritonectomy (1 patient); and hysterectomy (one patient). Table 1, shows the sites of recurrence, treatments, and outcomes of the patients with recurrences. The median DFS for the entire group was 17 months, with the 3-year DFS being 33%; and the median OS was 35 months with 3-year OS being 40.52% (Figs. 1 and 2), <F1&2> respectively.

Kaplan–Meier survival curve for disease-free survival (DFS). Cum, cumulative.
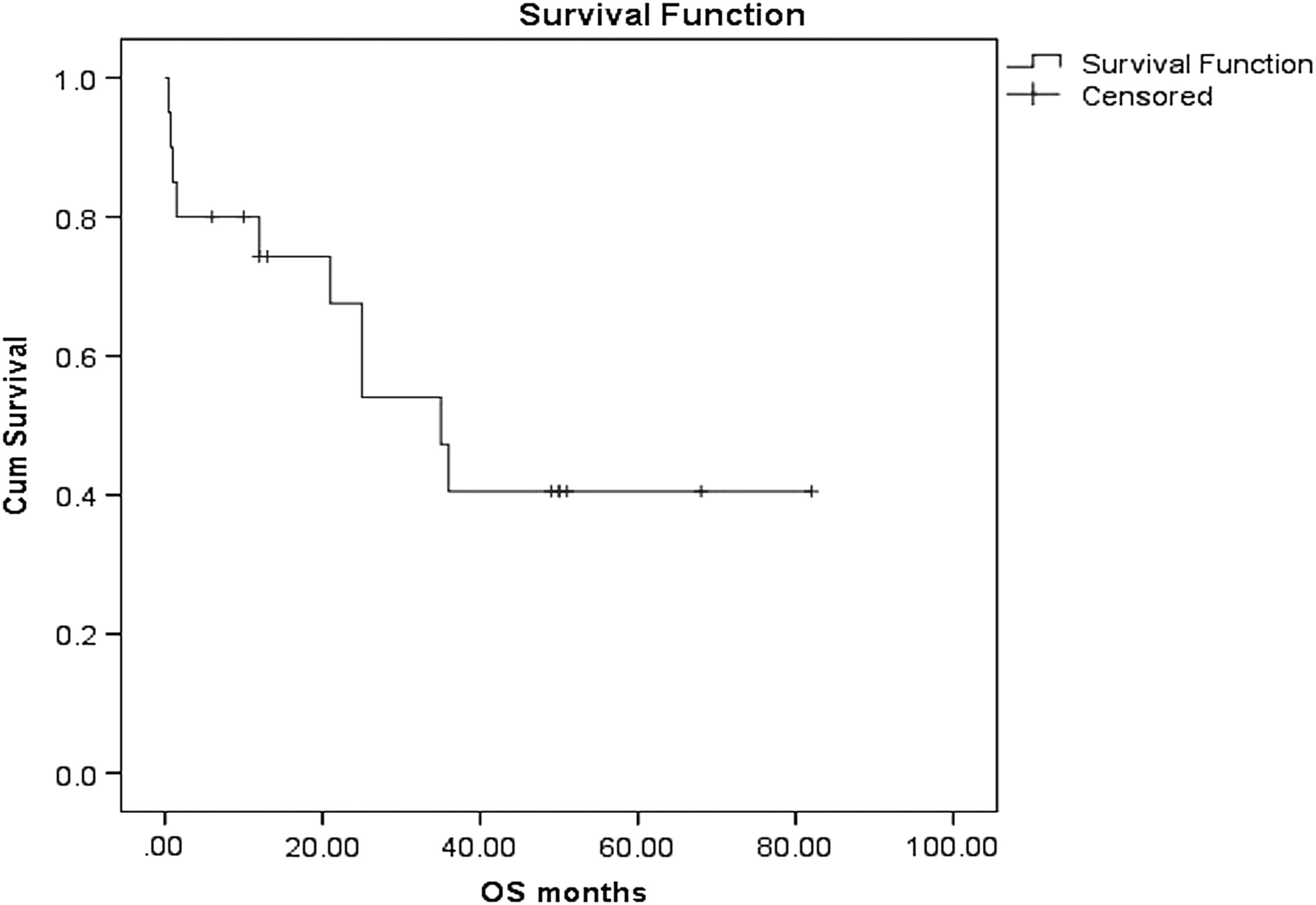
Kaplan- Meier survival curve for overall survival (OS). Cum, cumulative.
Clinicopathologic Characteristics & Management of Patients with Recurrent Ovarian Carcinosarcoma
S. #, serial number; FIGO, International Federation of Gynecology and Obstetrics; DFS, disease-free survival (months); OS, overall survival (months); CC-0, complete cytoreduction; PC, paclitaxel & carboplatin; POD, pouch of Douglas; CRS, cytoreductive surgery; f/b, followed by; DFS II, disease-free survival between surgery for 1st recurrence & development of 2nd recurrence; CT, chemotherapy; NED, no evidence of disease; TIP, paclitaxel, ifosfamide & cisplatin; DOD, died of disease; NACT, neoadjuvant chemotherapy; AWD, alive with disease; EBRT, external-beam radiotherapy.
Of the various prognostic factors evaluated, homologous histology and optimal cytoreductive status showed significant survival benefit on the log-rank test. The median OS was 21 months for heterologous histology and was not yet reached for homologous histology (0–42.14; 95% confidence interval [CI]; p = 0.019; Fig 3). The median OS was 1 month for suboptimal surgery and was not yet reached for optimal surgery (0.46–1.54; 95% CI; p < 0.0001; Fig. 4). On univariate analysis, optimal CRS and homologous histology were associated with significantly improved OS (p = 0.001 and 0.031, respectively). On multivariate analysis, only optimal surgery retained significance (p = 0.017; Table 2). For DFS, only homologous histology showed significantly improved survival on univariate analysis (p = 0.04), but not on multivariate analysis (Supplementary Table S1)
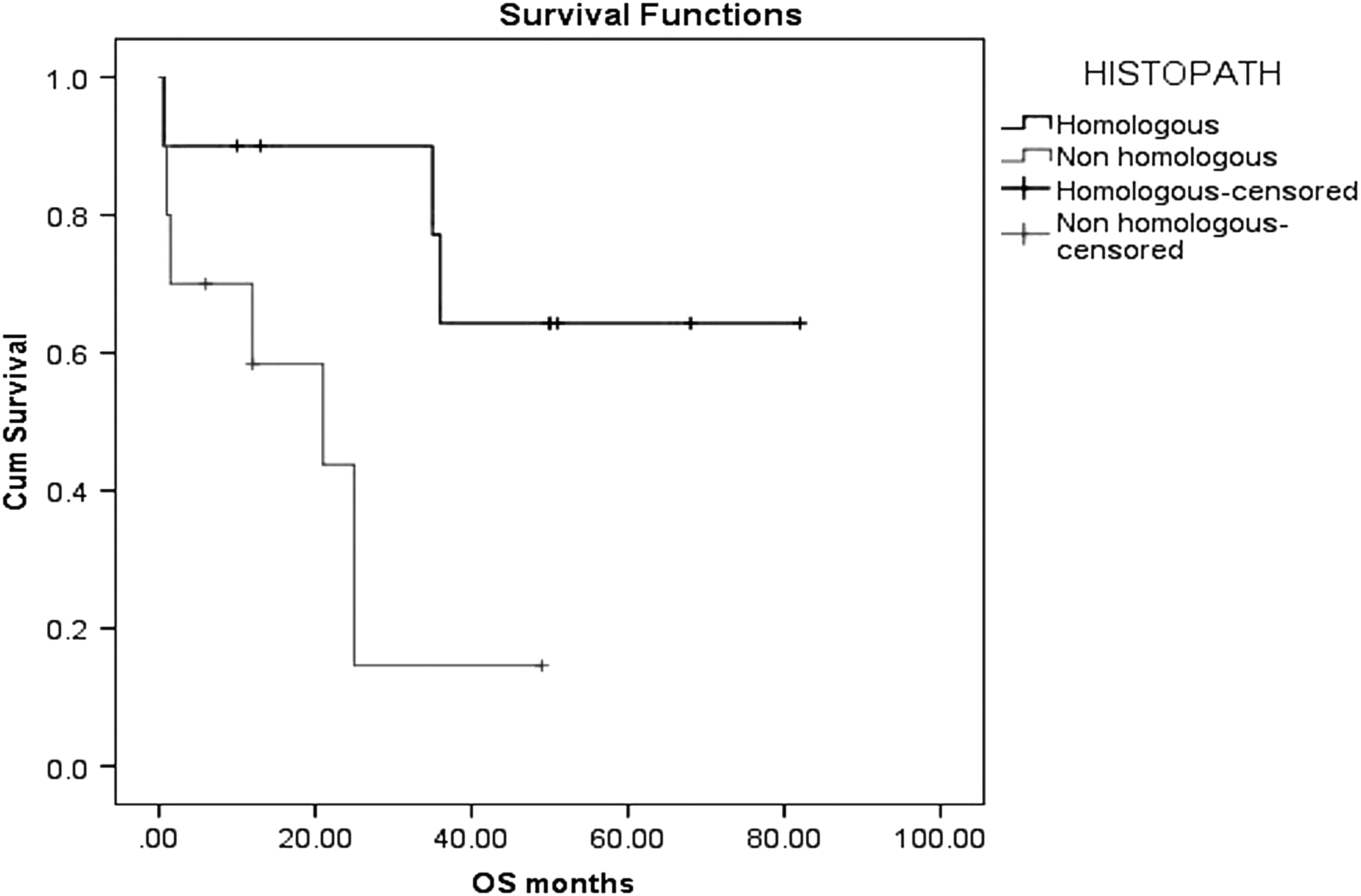
Kaplan-Meier survival curve. Survival analysis of patients with homologous histology, compared to patients with heterologous histology. Cum, cumulative; OS, overall survival; HISTOPATH, histopathology.

Kaplan-Meier survival curve. Survival analysis of patients with optimal surgery, compared to patients with suboptimal surgery. Cum, cumulative; OS, overall survival.
Univariate & Multivariate Analyses of Factors Predicting Overall Survival
Only includes patients who received 6 cycles chemotherapy.
Bold numbers denote significance.
CI, confidence interval; BMI, body mass index; TIP, paclitaxel, ifosfamide & cisplatin; PC, paclitaxel & carboplatin.
Discussion
Ovarian carcinosarcomas comprise one of the rarest and most-challenging histologic subtype of ovarian cancer. These tumors are defined histologically by the presence of malignant epithelial and stromal elements. The tumors are called homologous or heterologous, depending upon whether the sarcomatous component is native to the ovary or not. Homologous elements include fibrosarcomas and leiomyosarcomas. Heterologous elements include chondrosarcomas, osteosarcomas, rhabdomyosarcomas, and/or liposarcomas.7,8
The median age of patients in the current study was 54 years, which was lower than the quoted median of 60–70 years.2,9 The majority of the patients (65%) in the current study had stages III and IV disease, as was seen in various studies.2,6 In the current study, 85% of the patients had elevated preoperative CA-125 levels, which were similar to Sood et al.'s 10 findings, in which 90% of the patients had elevated CA-125 levels. In the current study, age was not an independent prognostic indicator, which was consistent with findings reported by Rutledge et al. 11
According to articles in the literature, early stage is the most important prognostic factor for OCS.6,12,13 Cicin et al. 6 reported longer median OS (50 versus 9.7 months; p = 0.042) and median progression-free interval (PFI; 25 versus 7.7 months; p = 0.05) in patients with early (I/II) versus advanced-stage disease. However, no significant difference was found in early versus advanced stage disease in a study by Harris et al. 5 In the current study, early stage was associated with improved DFS and OS, although the results were not significant for DFS (p = 0.20) and reached only borderline significance for OS (p = 0.06).
The malignant epithelial component in OCS is usually serous, endometrioid, or undifferentiated carcinoma, but can also be clear-cell or squamous-cell carcinoma. 3 In the current study, the most-common histology of epithelial components was serous carcinoma.
The impact of heterologous components on survival is unclear. Some studies suggest that the presence of heterologous components portends a poor prognosis.1,10 However, other studies failed to show any significant impact on survival due to heterologous components.2,5,12,14 In the current study, homologous histology of sarcomatous components was associated with statistically significant improvement in DFS and OS on univariate analysis.
Although the survival benefit associated with optimal cytoreduction in EOC is proven, earlier studies on OCS failed to demonstrate a correlation between the extent of cytoreduction and survival.9,15,16 However, the definition of optimal cytoreduction has varied over time. Eventually, studies have shown that, among women with advanced-stage OCS, optimal cytoreduction appears to be an important determinant of survival.1,5,10–12
Data on EOC from 2009 suggest that the goal of primary surgery should be cytoreduction to no gross residual disease. 17 However, the radical surgical procedures required to achieve this goal are associated with high postoperative morbidity. 18 Studies that have included patients with debulking to no residual disease have shown similar results in OCS. In a study by Doo et al., 19 patients who were cytoreduced to no residual disease had a median PFS of 29 months, versus 21 months for patients with ≤1 cm of residual disease and 2 months for those with >1 cm of residual disease (p = 0.036). The median OS was 57 months in patients with no residual disease, versus 32 months in those with ≤1 cm of residual disease and 11 months in patients with >1 cm of residual disease (p = 0.015). Similarly, Rauh-Hain et al. 20 reported a significant correlation between cytoreductive status and survival. The current study's results reinforce the notion that complete cytoreduction resulting in no gross residual disease should be the goal of upfront surgery for OCS. Operative management of these tumors should resemble that for EOC and should be performed at specialized centers by experienced gynecologic oncologists.21,22
Two patients received NACT outside. They were diagnosed as having stages IIB and IIIC after biopsies from pelvic deposits and omentum. The 2 patients underwent interval debulking surgery at the institute and complete cytoreduction was achieved in both cases. The patient with stage IIB disease was a long-term survivor with a DFS of 82 months. The patient with stage IIIC disease developed a recurrence in the perihepatic region and underwent secondary CRS and palliative chemotherapy but died of progressive disease with an OS of 35 months. Various reports have shown that NACT might be a reasonable strategy in patients with advanced-stage OCS.23,24
Given the proven efficacy of PC chemotherapy in EOC, various investigators have evaluated the role of this regimen in OCS. Duska et al., 25 reported a 72% response rate and an overall median survival of 27 months in 26 patients with OCS who were treated with PC. Similarly, Rauh-Hain et al. 20 reported a 62% response rate to this regimen in 50 patients with OCS.
The efficacy of cisplatin–ifosfamide in uterine carcinosarcomas has prompted the adoption of this regimen for OCS.26,27 In a study by Rutledge et al., 11 the median PFI was 12 months in a carboplatin–Taxol® group and had not yet been reached in an ifosfamide–cisplatin group (p = 0.005). OS was also significantly improved with ifosfamide–cisplatin (p = 0.03). In advanced-stage disease, no significant difference was seen between these 2 groups in OS. However, a greater proportion of patients with optimally debulked and early staged disease were treated with ifosfamide–cisplatin. The type of regimen lost significance on multivariate analysis. In the current study, the 3-year DFS for TIP (5 patients), compared to PC (10 patients), was 60% versus 17.8%, respectively (p = 0.21); and the 3-year OS was 80% versus 33.3%, respectively (p = 0.11), showing no significant advantage of adding ifosfamide. The toxicities associated with these regimens were not evaluated. Ifosfamide is cumbersome to deliver, requires prolonged hospitalization, and is less easy to tolerate than platinum and Taxol.11,27,28 Thus, the choice of paclitaxel versus ifosfamide as the second agent requires comprehensive clinical judgement.
In a review of literature by del Carmen et al., optimal CRS was associated with improved survival in patients with OCS and platinum-based chemotherapy was suggested to be the mainstay of adjuvant treatment. 29
In 2016, Rauh-Hain et al. reviewed the English language literature on OCS over 30 years from January 1985 till March 2016. 30 These investigators reviewed a total of 21 studies including 611 patients with OCS. The researchers concluded that treatment of OCS includes comprehensive surgical staging in patients with early stages disease and optimal cytoreductions in patients with advanced stages of disease, and that this should be followed by platinum-based adjuvant chemotherapy.
In a retrospective study of 47 patients with OCS, 72% developed recurrent or progressive disease, with a mean time to recurrence of 10.5 months, with 96% recurrences occurring in the first 2 years. Of these recurrences, 27 of 28 were in the pelvis and/or abdomen. 10 In the current study, 65% of the patients developed recurrent/ progressive disease with a median time to recurrence of 11 months. Due to its rarity, there are no prospective trials on the management of patients with recurrent OCS, and patients are treated on lines of management of women with recurrent EOC.
The current study showed an encouraging median OS of 35 months with a median follow-up of 23 months. The main strength of this study was that all of the patients underwent comprehensive staging or cytoreduction at the institute by experienced gynecologic oncologists. The histologic reports were reviewed by a dedicated gynecologic pathologist, which is important for such rare tumors so that they are not misclassified. The main limitations of the study were its retrospective design; small number of cases, which was insufficient to determine the impact of various clinical factors on survival using multivariate analysis; and heterogeneous nature of the patient population. This last limitation involved the cancer stages and chemotherapeutic regimens received, with 2 patients receiving NACT. Moreover, it was difficult to determine whether the improvement in survival associated with optimal cytoreduction was due to the surgery itself or was a function of the inherent aggressiveness of the tumors.
Conclusions
Optimal CRS resulting in no gross residual disease is associated with improved survival in patients with ovarian carcinosarcoma. Platinum-based chemotherapy is the current accepted adjuvant treatment. For a patient with an ovarian carcinosarcoma, the pathologic review should distinguish between heterologous and homologous histology, as this factor influences survival.
Clinical trials on carcinosarcoma of the ovary would be beneficial, but it might be difficult to obtain enough data on such patients because of the rarity of this entity.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.