
Abstract
Abstract
Objective:
Chronic postoperative pain poses a significant clinical challenge and is associated with a reduced quality of life and increased use of health services. The present study was conducted to determine the prevalence of chronic postoperative pain and potential risk factors for developing chronic postoperative pain after robot-assisted laparoscopic hysterectomy.
Materials and Methods:
This was a questionnaire-based, cross-sectional retrospective study. Patients treated for endometrial cancer with robot-assisted laparoscopic hysterectomy from January 2010 until July 2015 received a validated questionnaire. The questionnaire had 32 questions related to preoperative and the postoperative conditions and was used to assess the presence of preoperative pelvic pain, chronic postoperative pelvic pain, pain intensity ratings, frequency and location of pain, pain during everyday activities, and demographic data. The medical records were reviewed for details concerning body mass index, duration of surgery, blood loss during surgery, histopathologic diagnoses, and stages of cancer.
Results:
Questionnaires were sent to 272 patients and 207 (76.1%) responded. The prevalence of chronic postoperative pain was 14.9%. It was predominantly localized to dermatomes T-12–L-3 and S2–S4. Significant risk factors for chronic postoperative pain were preoperative pelvic pain (odds ratio [OR]: 4.99) and a high level of acute postoperative pain (OR: 1.27) (p < 0.05).
Conclusions:
The prevalence of chronic postoperative pain after robot-assisted laparoscopic hysterectomy was 14.9%. Risk factors were preoperative pelvic pain and a high level of acute postoperative pain, indicating that these factors should be included when counseling patients and that research efforts should be taken to find ways to minimize the postoperative impact of these factors.
Introduction
Endometrial cancer is the fourth most common cancer among women in the United States and Western Europe. 1 The primary treatment is surgery, depending on the stage of cancer, ranging from hysterectomy and bilateral salpingo-oophorectomy to more advanced surgery with additional pelvic and para-aortic lymphadenectomy. Robot-assisted laparoscopic surgery has become the standard method of choice at many centers of gynecologic oncology. 2 This approach offers a combination of minimally invasive surgery and a superior level of microsurgical technique, compared with conventional laparoscopic surgery or laparotomy.3,4 Development of chronic postoperative pain following hysterectomy has been reported to affect 4.7%–31.9% of patients, is associated with a decreased quality of life, and poses a significant clinical challenge to manage adequately.5–17 No differences in the percentage of chronic postoperative pain in patients has been found between those who underwent abdominal hysterectomy versus robot-assisted laparoscopic hysterectomy. Studies have indicated that the pain predominantly is of visceral origin and is less associated with the level of somatic trauma. 8
It is important to understand the risk factors for development of chronic postoperative pain, and it is hoped that understanding will help reduce that pain to improve outcomes. Previous studies have indicated that preoperative chronic pain conditions, such as severe endometriosis and a high intensity of acute postoperative pain, are associated with the development of chronic postoperative pain.8,18,19
The objectives of the present study were (1) to determine the prevalence of chronic postoperative pain after robot-assisted laparoscopic hysterectomy for endometrial cancer and (2) to assess potential pre- and postoperative risk factors for the development of chronic postoperative pain.
Materials and Methods
This was a questionnaire-based, cross-sectional retrospective study. The inclusion criteria were Danish-speaking women, ages 18–85, with histopathologic diagnoses of endometrial cancer that was treated with robot-assisted laparoscopic hysterectomy at the department of obstetrics and gynecology, Aalborg University Hospital, in Aalborg, Denmark, from January 1, 2010, until July 31, 2015. The exclusion criteria were use of cannabis or opioids, conversion of the robot-assisted laparoscopic procedure to open surgery, subsequent open surgery, and neurologic or mental illnesses.
Diagnosis and staging
Each patient was diagnosed by means of tissue sampling from the endometrial cavity and was stratified in a risk category based on the histologic type and grade according to the ESMO-ESGO-ESTRO [European Society for Medical Oncology–European Society of Gynecological Oncology–European Society of Radiotherapy and Oncology] guidelines. 20 Low-risk cases were assigned to robot-assisted laparoscopic hysterectomy and bilateral salpingo-oophorectomy. The degree of macroscopic myometrial invasion was assessed by a pathologist peroperatively and cases with >50% myometrial invasion—indicating an International Federation of Gynecology and Obstetrics (FIGO) stage of Ib or higher 21 —received additional pelvic lymphadenectomy. Intermediate-risk cases were also assigned to hysterectomy, bilateral salpingo-oophorectomy, and pelvic lymphadenectomy, while only high-risk cases received additional para-aortic lymphadenectomy. High-risk patients with tumors of nonendometrioid types, including sarcomas, also underwent preoperative positron emission tomography–computed tomography for staging purposes.
Surgical procedures
The surgical procedures were performed with Da Vinci™ Si robotic systems (Intuitive Surgical Inc., Sunnyvale, CA) with the patients placed in a 30° Trendelenburg position. All cases were reviewed postoperatively in multidisciplinary tumor board meetings and final staging was determined in accordance with the FIGO criteria. Secondary lymphadenectomy was performed in case of upstaging from stage Ia to stage Ib.
Study approval
The study was performed in accordance with the declaration of Helsinki, approved by the local ethics committee (N-20150028), and conducted in agreement with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines. 22
The questionnaire
The questionnaire was comprised of 32 questions in the Danish language and was structured in two parts. It was mailed along with a prepaid return envelope to each patient in July 2017. The first part contained questions related to the preoperative time period, while the second part was related to the postoperative time period. The following variables were collected: presence of preoperative pelvic pain (“yes/no”); chronic postoperative pelvic pain (“yes/no”); pain intensity ratings by a numeric rating scale (NRS); frequency of the pain (“1–3 days a week, 4–6 days a week, every day”); the location of any pain (marked on an illustration of a woman's torso); influence of the pain in everyday activities (“none, mild, moderate, strong”); influence of the pain on sex life (“yes/no”); influence of the pain on sleep (“yes/no”); and demographic data such as education level and employment status. Chronic postoperative pain was defined as constant or periodical pain for at least 3 months. 17
The questionnaire was controlled for validity after development and had been applied subsequently in a previously published study. 8
Nonresponsive patients were contacted by telephone 3 weeks after receiving the mailed questionnaire and again after 2 weeks, if the patient still did not respond. The returned questionnaires were gathered for data analysis in October 2017.
Review of medical records
The medical records of all eligible patients were reviewed for details concerning body mass index (BMI) at the time of surgery (kg/m 2 ), duration of surgery (in minutes), the blood loss during surgery (in mL), number and type of intraoperative lesions if any, parity and caesarean sections and histopathologic diagnoses and stages of cancers.
Statistical analysis
Continuous data were displayed as mean with 95% confidence intervals (CIs) and categorical data were displayed as frequency in percentage. Analysis of baseline characteristics included age, BMI, education, employment status, parity, operating time, blood loss, and time of follow up.
To examine potential selection bias among questionnaire responders and nonresponders, a Mann-Whitney–U test of the 2 groups were performed, using the independent variables age, BMI, operating time, and blood loss. Furthermore, a sample survey of 10 nonresponders were contacted by telephone and asked about presence of chronic pelvic pain, frequency and pain intensity rating.
A binary logistic regression analysis with a backward stepwise selection of risk factors for chronic postoperative pain following robot-assisted hysterectomy was performed with the following independent variables: preoperative pelvic pain; acute postoperative pain intensity; preoperative pain elsewhere; age; severity of cancer stage ± lymphadenectomy; operating time; blood loss; education; and employment status. The statistical analyses were performed with IBM SPSS Statistics software for Mac OS, Version 25.0 (IBM Corp., Armonk, NY).
Results
Two hundred and eighty patients were treated for endometrial cancer with robot-assisted laparoscopic hysterectomy at the department from January 1, 2010 until July 31, 2015. Eight patients were excluded due to dementia, subsequent open surgery, or death. The remaining 272 were included in the study and received the questionnaire.
Two hundred and seven patients returned the questionnaire (76.1%) whereas 65 patients did not return the questionnaire (23.9%). Figure 1 is a flowchart of the study and questionnaire responses. Nonresponders were significantly older (mean age: 67.2; p = 0.027), compared with the responders (mean age: 63.4) but had similar BMIs (p = 0.869), operating times (p = 0.551), and blood losses (p = 0.126). When contacted by telephone, one out 1 of 10 randomly selected nonresponders indicated a chronic pelvic pain condition with a frequency of 1–3 days/week and an intensity of 3 on the NRS.

Flowchart of the study and questionnaire responses.
There were no recorded cases of severe procedure-related injuries, including lymphocysts following lymphadenectomy, damage to pelvic nerves, or other traction injuries due to the Trendelenburg position during the procedure. Please refer to Table 1 for baseline characteristics of the included patients.
Baseline Characteristics
Data are displayed as mean (95% CI) for continuous data and n (%) for categorical data.
BMI, body mass index, CI, confidence interval.
Tumor characteristics
Histologic type and grade, FIGO stage, and risk category of all 207 responding patients are shown in Table 2. The low-risk cases (without lymphadenectomy) accounted for 58.5% of the patients, while the intermediate and high-risk cases (with lymphadenectomy) accounted for 41.5%.
Tumor Characteristics
FIGO, International Federation of Gynecology and Obstetrics.
Pain characteristics
The reported pain characteristics are shown in Table 3. Thirty-five patients (16.9%) indicated that they had preoperative pain and 31 patients (14.9%) indicated that they had chronic postoperative pain. The mean preoperative pain intensity was 4.3 (95% CI: 3.2–4.8) and mean postoperative pain intensity was 3.6 (95% CI: 2.8–4.4). The prevalence of postoperative pain in everyday activities were most prominent during heavy lifts (40.0% in the preoperative group and 48.4% in the postoperative group) and sexual intercourse (37.1% and 29.0%, respectively).
Pain Characteristics of the Preoperative Pelvic Pain and Postoperative Pelvic Pain
Data are displayed as n (%) for categorical data and mean (95% \ CI) for continuous data.
Based on the mean age of the study sample.
Based on the mean BMI of the study sample.
Intensity ratings by numeric rating scale.
CI, confidence interval; BMI, body mass index.
The thirty-one patients with chronic postoperative pain marked the areas corresponding to dermatomes T-12–L-3 and S-2–S-4 on an illustration of a woman's torso. Please refer to the summarized illustration in Figure 2.
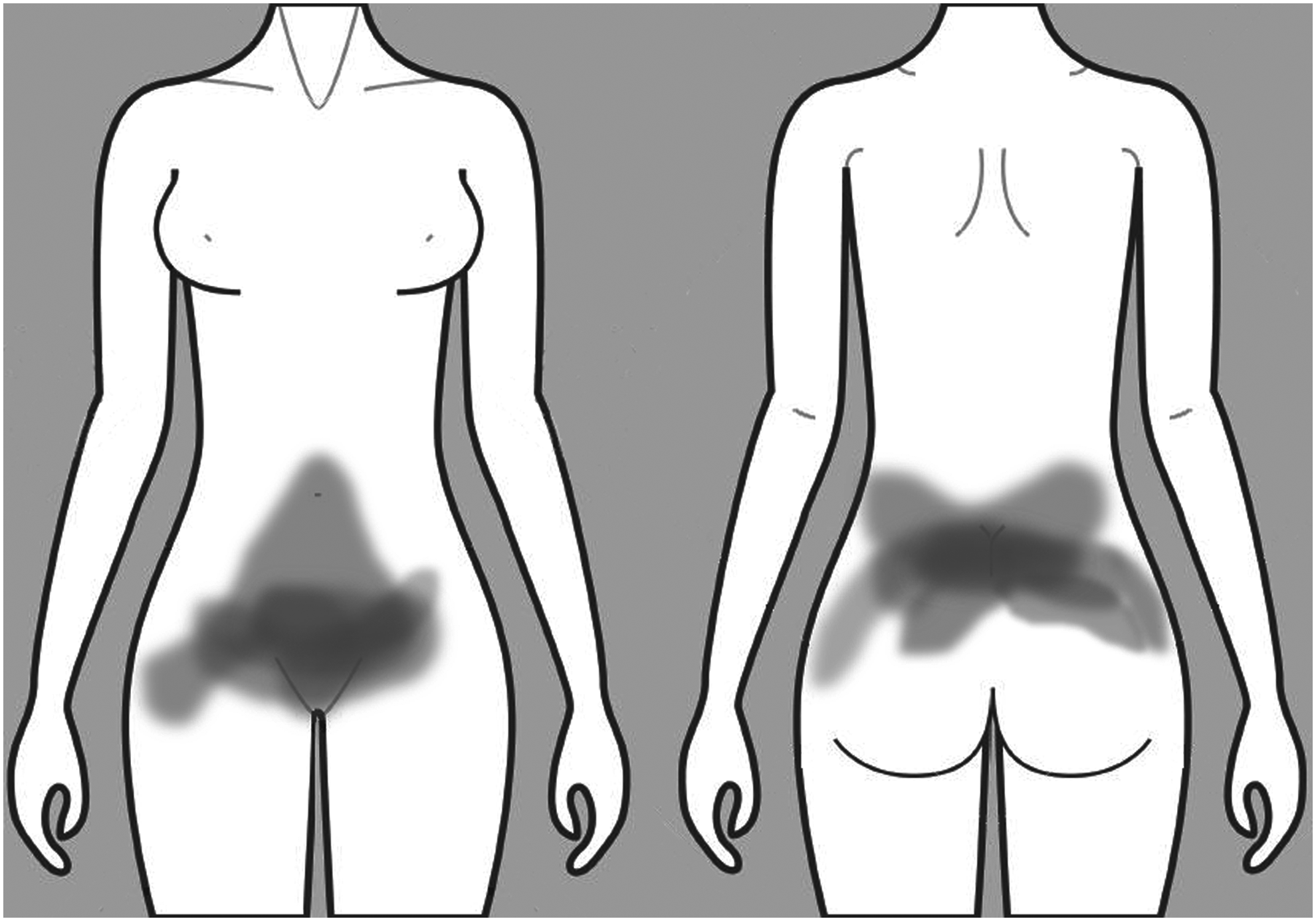
Summarized areas of chronic postoperative pain.
Risk factors for development of chronic postoperative pain
The binary logistic regression model with a backward stepwise selection of risk factors was made in 2 models. Model 1 (Nagelkerke R2 0.419) included all study parameters (preoperative pelvic pain, acute postoperative pain intensity, preoperative pain elsewhere, age, severity of cancer stage ± lymphadenectomy, operating time, blood loss, education, and employment status). Model 2 (Nagelkerke R2 0.382) only included 4 study parameters from model 1 (preoperative pelvic pain, acute postoperative pain intensity, age, and education). The regression model established 2 significant factors for development of chronic postoperative pain (p < 0.05): preoperative pelvic pain (odds ratio [OR]: 4.99, 95% CI: 4.15–5.83) and acute postoperative pain (OR: 1.27; 95% CI: 1.09–1.45) while demonstrating a trend toward age as a protective factor (OR: 0.94: 95% CI: 0.88–1.00). Please refer to Table 4.
Binary Logistic Regression with Backward Stepwise Selection of Risk Factors for Postoperative Chronic Pain Following Robot-Assisted Hysterectomy
Data are displayed as OR (95% CI).
OR, odds ratio; CI, confidence interval.
Discussion
The present study showed a prevalence of chronic postoperative pain of 14.9% after robot-assisted laparoscopic hysterectomy for endometrial cancer. Linear regression models showed that higher preoperative pelvic pain intensities and higher acute postoperative pain intensities were independent and significant predictors for chronic postoperative pain.
The prevalence of chronic postoperative pain
This prevalence of chronic postoperative pain corresponds well to a previously published research article from Sørensen et al., 8 in which chronic postoperative pain was found in 16.9% and 11.9%, respectively, of patients following abdominal hysterectomy or robot-assisted laparoscopic hysterectomy for endometrial cancer. Remarkably, the researchers did not find any significant difference between the incidence of chronic postoperative pain in the 2 groups, suggesting that the level of somatic trauma (i.e., difference in surgical access) is of less importance, while visceral deafferentation pain (phantom visceral pain) could be a plausible explanation for chronic postoperative pain after hysterectomy.
Conversely, several earlier studies have demonstrated a significantly higher prevalence of chronic pelvic pain after hysterectomy: Stovall et al. 5 found a prevalence of 22.2% (abdominal hysterectomy), Hillis et al. 10 found a prevalence of 26.0% (abdominal hysterectomy), and Brandsborg et al. 17 found a prevalence of 31.9% (abdominal, vaginal and laparoscopic hysterectomy). These results, in part, could be explained by the different measures of pain scales and criteria used to assess chronic postoperative pain. The indication for hysterectomy, however, could also explain the difference in reported prevalence of chronic pelvic pain. The indication for hysterectomy in the first-mentioned studies was chronic pelvic pain,5,10 whereas the indications for hysterectomy in the latter study in addition to chronic pelvic pain were other benign disorders such as leiomyomas, dysmenorrhea, or endometriosis. 17 This differentiation of indication is of key importance, given that numerous benign disorders of the uterus are strongly associated with chronic pelvic pain. 23 Moreover, numerous studies from other fields, have shown that patients suffering from chronic pain conditions are predisposed to develop postoperative pain.8,17–19
The primary symptom of endometrial cancer is postmenopausal vaginal bleeding while pelvic pain is rarely a clinical symptom. Hence, studies of postoperative pain following hysterectomy for benign disorders (including chronic pelvic pain) are not fully comparable to studies of postoperative pain following hysterectomy for malignant disorders. Consequently, the current authors assume that the true prevalence of chronic postoperative pelvic pain following robot-assisted laparoscopic hysterectomy for endometrial cancer is somewhat closer to the current authors' finding of 14.9% rather than studies of higher prevalence among benign, yet pain-causing, disorders of the uterus.
Predicting chronic postoperative pain
Preoperative pelvic pain and a high level of acute postoperative pain intensity proved to be significant independent risk factors for development of chronic postoperative pain. These findings are in accordance with previous research.17,24 Binary logistic regression also showed a trend toward older age as a protective factor, which has also been reported in patients undergoing inguinal herniorrhaphy.9,25 The vast majority of endometrial cancers are diagnosed at an early stage, 26 mainly due to the pathognomonic symptom of postmenopausal vaginal bleeding. Likewise, most of the patients in the present study were at an early stage of endometrial cancer, thus, reducing the number of patients with advanced stages of the cancer to a minor fraction. This might be one of the reasons why the severity of cancer stage did not prove to be a significant factor.
The pathophysiology responsible for chronic postoperative pain is assumed to be triggered predominantly by deafferentation of the visceral-nerve innervations. 27 The uterus and adnexa are richly innervated by visceral, sympathetic nerve fibers that converge in the dorsal horn of the spinal segments T-12–L-3 and S-2–S-4. 28 These spinal segments are the same as indicated by the summarized areas of chronic pain shown in the present study, thereby supporting a theory of referred pain/phantom pain from the reproductive organs.29,30 In cases of hysterectomy and bilateral salpingo-oophorectomy, these nerve fibers are irrevocably transected, thus, activating an inflammatory cascade with release of sensitizing humeral mediators. These mediators—for instance, tumor necrosis factor (TNF)—lower the excitatory threshold of the free nerve endings and thereby heighten peripheral pain sensitivity. 27 This state, known as primary hyperalgesia, is an appropriate, biologic response to tissue injury; in individuals with a preoperative pelvic pain condition, the peripheral sensitization can be supplemented further by a pathologic response of central sensitization in the spinal cord (secondary hyperalgesia). 31 This condition is believed to be triggered by intense noxious peripheral stimuli, leading to an amplified synaptic activity and loss of segmented inhibitory transmission in the dorsal horn. 32 This mechanism is also believed to be the predominant pathophysiology in cases of hyperalgesia and allodynia. 33 The association between central sensitization and allodynia was demonstrated further in a study by Brandsborg et al., 34 in which allodynia of the dermatomes T-12–L-3 and S-2–S-4 was correlated to an increased risk of chronic postoperative pain after hysterectomy. These are the same dermatomes that were reported to be affected by the patients with chronic postoperative pain in the present study.
Limitations
The present study was conducted solely at one department of obstetrics and gynecology. In general, studies from a single center should be interpreted with caution, given that the findings should be verified at multiple centers for complete validity. The risk of recall bias is also an important limitation, considering the mean number of days from surgery to questionnaire was 1053.2 (2.9 years). A questionnaire responder rate of 76.1% is acceptable; however, the analysis of the responders versus nonresponders showed a significant difference in mean age of 67.2 versus a mean age of 63.4 years, respectively, but no general difference in the incidence of chronic postoperative pain. This indicates a selection bias, although there were no differences in BMI, operating time, nor blood loss.
Conclusions
The present study showed a prevalence of chronic postoperative pelvic pain of 14.9% after robot-assisted laparoscopic hysterectomy for endometrial cancer. Linear regression models identified high preoperative pelvic pain intensities and a high level of acute postoperative pain intensities as significant independent risk factors for development of chronic postoperative pain. The findings suggest that deafferentation of visceral, sensory, and sympathetic nerve fibers is the plausible trigger of chronic pain, and, as such, was considered as a visceral phantom pain syndrome.
Footnotes
Author Disclosure Statement
No competing financial interests exist.