
Abstract
Abstract
Objective:
The aims of this research were to evaluate concordance of practice patterns for preoperative electrocardiogram (EKG) and chest X-ray for benign hysterectomy with institutional and international guidelines, and to assess implications for perioperative management.
Materials and Methods:
For this retrospective cohort study (Canadian Task Force II-2), medical records of 587 women who underwent hysterectomy for benign indications at a single institution, from January 1 through December 31, 2016, were reviewed. Each EKG and chest X-ray (CXR) was evaluated for indications, concordance with institutional and with the United Kingdom's National Institute for Health and Care Excellence (NICE) guidelines, results, effects on management, and association with perioperative complications. Descriptive statistics were used for analysis.
Results:
Subjects were, on average, 45 (range: 27–76) years old, with primarily Hispanic (58.4%) and black (30.0%) race. For 587 hysterectomies, 182 EKGs (31.0%) and 70 CXRs (11.9%) were ordered. EKG was indicated for s90 (49.5%) patients per institutional criteria and for 177 (97.3%) patients per NICE criteria. Findings were abnormal in 81 (44.5%) of 182 EKGs. Further work-up was pursued for 16 (19.8%) patients. There were 2 case delays, but no cancellations. Notable perioperative events included nonspecific EKG changes and airway edema in 2 patients with abnormal preoperative EKGs. Of 70 CXRs ordered, 17 (24.3%) were in concordance with institutional criteria. No CXRs were indicated per NICE criteria. There were abnormal findings on 10 (14.3%) chest X-rays. The anesthesia department was consulted for 1 patient. There were no case delays/cancellations or perioperative cardiopulmonary complications.
Conclusions:
Preoperative EKGs and CXRs offer little clinical utility for patients undergoing benign hysterectomy.
Introduction
Preoperative testing for hysterectomy in benign gynecology is variable, as there is no single standard of care. The University of Texas Southwestern Medical Center, in Dallas, TX (the current authors' institution), like other medical institutions in the United States, uses guidelines developed by the clinical staff and managed by the anesthesia department. 1 In contrast, in several European countries, the National Institute for Health and Care Excellence (NICE) recommendations are used to guide preoperative work-ups for elective procedures such as hysterectomy. 2 These guidelines are unique because they are based on available evidence from systematic reviews and cost analyses. 2 No evidence-based guidelines for preoperative work-ups specific to gynecologic surgery are presently available.
Although various preoperative tests are commonly pursued to optimize patients for surgery, there are few data linking such studies to surgical outcomes. The ideal preoperative tests should stratify preoperative risk, guide anesthetic management, and direct postoperative care. Testing without clear indications could lead to unnecessary work-ups and potential physical, psychologic, or financial harms. Studies have shown that, although abnormal test results are frequent, changes in management are rare.3,4
Electrocardiograms (EKGs) and chest X-rays (CXRs) are commonly ordered to assess cardiopulmonary function prior to hysterectomy. The current authors' institutional guidelines largely overlap with those of NICE for EKG, but differ starkly for CXR.1,2 This discordance demonstrates the lack of consensus on appropriate utilization of preoperative testing. The current study was conducted to evaluate the rates of preoperative EKG and CXR for benign hysterectomy in the context of institutional and NICE guidelines, and to assess implications for surgical management, perioperative complications, and costs.
Materials and Methods
Approval through the University of Texas Southwestern Medical Center's institutional review board (IRB) was obtained for this study (IRB Protocol #082017-063, approved September 6, 2017). Because the study was designed with the intention of collecting baseline data for subsequent quality-improvement interventions, convenience sampling of patients who underwent benign hysterectomy over the course of 1 year was utilized. The medical records of these 587 consecutive women who underwent hysterectomy for benign indications at a single institution, Parkland Hospital, Dallas, TX, from January 1 through December 31, 2016 were identified using an institutional database. Cases treated in the benign gynecology, urogynecology, and reproductive endocrine and infertility services for women ages 18 or older were included. Participants were excluded if their hysterectomies were performed for emergent indications or if performed by the gynecology oncology team for known or suspected malignancies.
Retrospective analysis was performed. Demographic characteristics of subjects, including age, body mass index, and comorbid medical conditions at the time of preoperative evaluation were recorded. Each preoperative EKG and CXR was evaluated for indication, concordance with both institutional and NICE guidelines, results, effect on management, and association with cardiopulmonary complications from the time of surgery through 6 weeks postoperatively.
EKG results were read independently by a staff cardiologist. CXRs were read by a staff radiologist or resident physician with certification by a staff radiologist. Changes in preoperative planning were defined as changes in route of hysterectomy, orders for new medications or additional work-ups, or delays in care. The postoperative period was meticulously evaluated with consideration of all categories of complications. Readmissions visible through “Care Everywhere”—a medical-record exchange feature shared by major local hospitals through the Epic electronic medical record system 5 —were included in this analysis. Postoperative readmissions were graded using Clavien–Dindo (CD) classification criteria. 6 Costs of tests performed were calculated using 2017 state-specific (TX) Medicaid reimbursement rates and included technical and professional fees for CXR, but technical fees only for EKG. 7 Descriptive statistics were included in the analysis, using Microsoft Excel.
Results
The average age of the study subjects was 45 (range: 27–76). Patients were primarily of Hispanic (58.4%) and black (30.0%) races. Additional races included non-Hispanic white (8.3%), Asian (1.4%), and Native American, or Alaska Native (0.2%). The races of 10 patients (1.7%) was unknown. All patients received general endotracheal anesthesia. For 587 benign hysterectomies performed, 182 EKGs (31.0%) and 70 CXRs (11.9%) were ordered.
Hysterectomy routes for patients who underwent preoperative EKG included 82 (45.1%) total abdominal hysterectomies (TAHs), 53 (29.1%) total laparoscopic hysterectomies (TLH) or laparoscopic-assisted vaginal hysterectomies (LAVHs), and 47 (25.8%) total vaginal hysterectomies (TVHs). The average age of women who underwent preoperative EKG was 47.4 years (range: 30–76).
EKG in 90 (49.5%) patients was indicated according to institutional criteria and in 177 (97.3%) patients per NICE criteria (Table 1). By institutional criteria, age and alcohol/drug use were the most common indications in 46 (51.1%) and 42 (46.7%) patients, respectively. Although hypertension and obesity were commonly cited by ordering providers as indications, only “cardiovascular disease” was specified as an institutional criterion. The American Heart Association's definition of atherosclerotic cardiovascular disease as prior myocardial infarction or stroke was used for this analysis. 8 Additional indications are listed in Table 2. By NICE criteria, 145 (82.0%) EKGs were indicated for American Society of Anesthesiologists (ASA) classification 2, 28 (15.8%) for ASA classification 3, and 8 (4.5%) for age 65 or above.
Institutional Versus National Institute for Health and Care Excellence Guidelines for Preoperative Electrocardiogram Prior to Elective Surgery
NICE, National Institute for Health and Care Excellence; ASA, American Society of Anesthesiologists.
Stated Indications for EKG & Concordance with Institutional Versus NICE Criteria
Multiple indications were possible for each electrocardiogram, thus, percentages do not add to 100%.
EKG, electrocardiogram; NICE, National Institute for Health and Care Excellence.
Findings were abnormal in 81 (44.5%) EKGs. The average age for patients with abnormal EKGs was 47.2 years (range: 32–68). In the 17 patients whose EKGs were indicated because of abnormal results in reviews of systems or cardiac examinations, 10 (58.8%) were found to have EKG abnormalities. A breakdown of positive results is shown in Figure 1. Further work-ups were pursued in 16 of 81 (19.8%) patients with abnormal EKG findings including repeat EKGs (6), cardiac testing such as echocardiograms or stress tests (7), and/or specialist consultations (7). Two surgical delays of 1 and 4 months occurred as a result of additional work-ups ordered for 2 patients with abnormal EKGs with ultimate completion of the planned hysterectomies without changes in routes of hysterectomy, prescribed medications, or postoperative management.
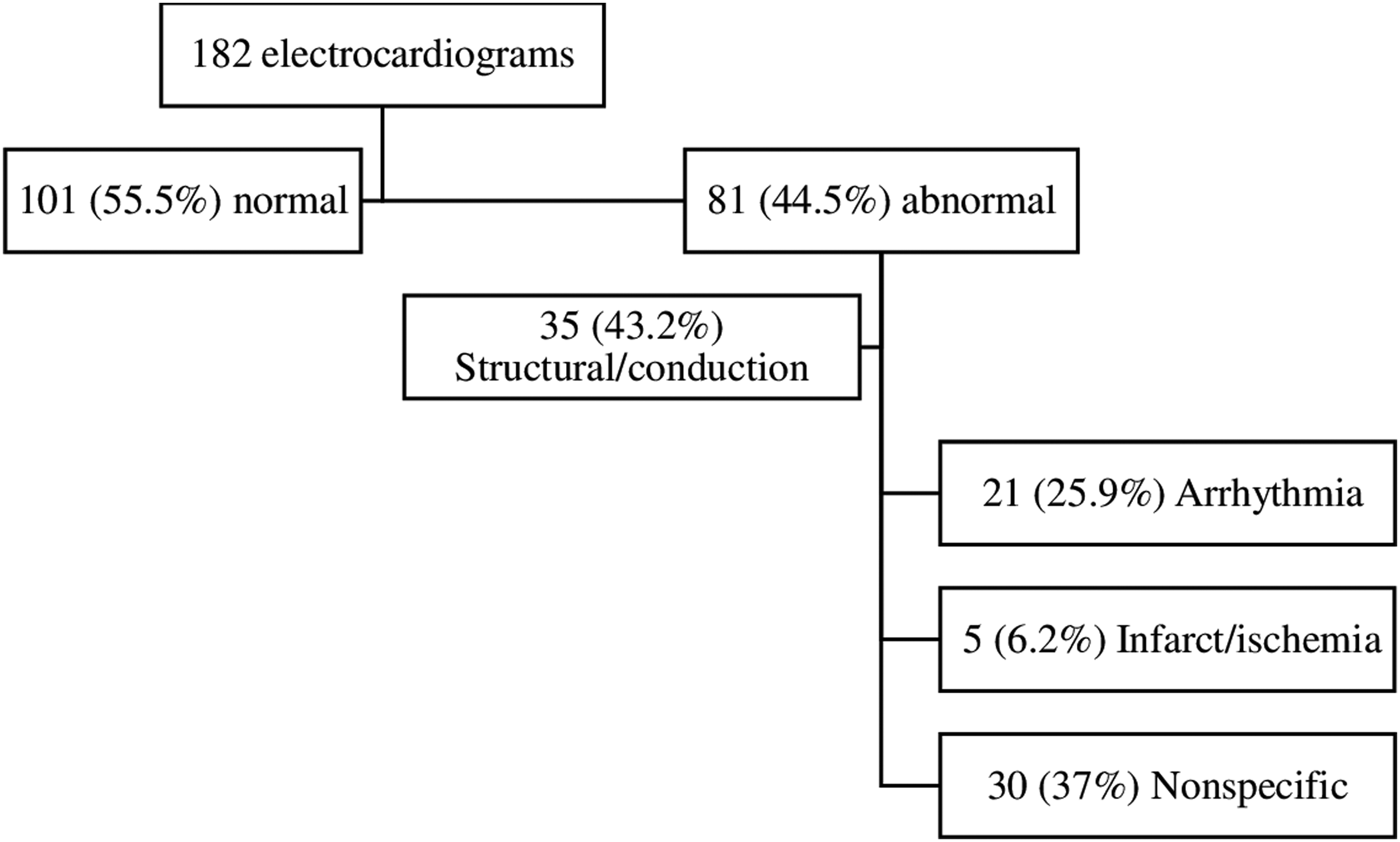
Preoperative electrocardiogram (EKG) results with examples from each category of abnormality. Irregularities were related to structure/conduction, arrhythmia, infarction/ischemia, and nonspecific findings. Several EKGs showed abnormalities spanning multiple categories.
Two perioperative complications and 10 postoperative readmissions were noted in patients who underwent preoperative EKG. Surgery was aborted after nonspecific ST-segment changes after induction in a patient with left ventricular hypertrophy revealed on a preoperative EKG. A second patient, with a preoperative EKG showing a prior inferior infarct, had a failed extubation due to airway edema. Indications for postoperative readmissions, 9 of which were within 30 days, included 3 wound infections managed with antibiotics (Clavien–Dindo II) in 2 patients and with surgical intervention (Clavien–Dindo IIIb) in 1 patient, 1 ureteral injury (Clavien–Dindo IIIa), 1 pulmonary embolism (Clavien–Dindo II), 1 ileus (Clavien–Dindo I), 1 gastroenteritis (Clavien–Dindo I), 1 pyelonephritis (Clavien–Dindo II), and 1 nonischemic chest pain (Clavien–Dindo I). Eight of these patients had abnormal preoperative EKGs, but none of them had additional work-ups or changes in perioperative management.
Hysterectomy routes for subjects who underwent preoperative CXR included 32 (45.7%) TAHs, 21 (30.0%) TLHs or LAVHs, and 17 (24.3%) TVHs. The average age of women who underwent preoperative CXR was 47.8 years (range: 31–76).
Of the 70 CXRs ordered, 17 (24.3%) were in accordance with institutional criteria (Table 3). No CXRs were indicated per NICE criteria. Stated indications for obtaining a CXR included histories of asthma in 13 patients (61.5% mild intermittent, 57.1% mild persistent, and 7.7% moderate persistent) with other indications listed in Table 4. The remaining 53 (75.7%) CXRs were not indicated by institutional criteria, but were ordered most commonly for histories of smoking with a median pack–year history of 3.8 (range: 0.1–40).
Institutional Versus NICE guidelines for preoperative CXR prior to elective surgery
NICE, National Institute for Health and Care Excellence; CXR, chest X-ray
Stated Indications for CXR & Concordance with Institutional Versus NICE Criteria
Multiple indications were possible for each CXR, thus, percentages will not add to 100%.
CXR, chest X-ray; NICE, National Institute for Health and Care Excellence; N/A, not applicable.
Results showed new abnormal findings in 10 of 70 (14.3%) CXRs with results as listed in Figure 2. The average age for patients with abnormal CXRs was 54.2 years (range: 38–76). Known cardiomegaly and atelectasis were shown again in 2 patients. In the 4 patients with CXRs ordered for abnormal results on reviews of systems or physical examinations, there were no new findings. One patient had a 4-month delay in surgery due to a CXR ordered for work-up related to a reported history of “anesthetic complications.” No surgeries were cancelled based on CXR findings.

Preoperative chest X-ray (CXR) results with breakdown of abnormalities. Results were considered abnormal if they showed new pathology that was not previously seen on CXRs. Several CXRs showed abnormalities spanning multiple categories.
There were no intraoperative cardiopulmonary surgical or anesthetic complications in patients who had preoperative CXRs. Three patients were admitted postoperatively, all within 30 days, for wound infection (CD II), ileus (CD I), and pulmonary embolism (CD II). The latter patient also had a preoperative EKG as described above. Of these 3 patients, only the patient with the wound infection had an abnormal preoperative CXR with finding of mild cardiomegaly. Management for this patient was not altered.
Medicaid reimbursement rates estimated $17.28 per EKG and $23.09 per CXR, totaling to $3,144.96 and $1,616.30 over 1 year, respectively. 7
Discussion
A growing body of literature has questioned the evidence behind routine preoperative testing across surgical specialties, but few studies have focused on individual tests in relation to specific procedures. This study contributes an isolated analysis of EKGs and CXRs used to evaluate cardiopulmonary risks prior to hysterectomy for benign indications, one of the most commonly performed major surgical procedures.
At the current authors' institution, EKGs are ordered for preoperative evaluation of 31% and CXRs for 12% of patients undergoing benign hysterectomies. In the current study, although concordance with institutional guidelines for EKG was poor, concordance with NICE guidelines was excellent. This is likely explained by prevalent comorbidities such as obesity that raise ASA classification but are not considered “cardiovascular disease” according to institutional criteria. Institutional criteria did not reference an operational definition for cardiovascular disease, which varies by organization. Similarly, alcohol use, a common indication for EKG under both guidelines, was not quantified by either set of criteria.
Guideline concordance for CXR was unexpectedly low. Smoking was the most common stated indication for CXR in this study and was nonconcordant with both criteria. In our analysis, none of the CXRs ordered were indicated per NICE guidelines. The discrepancy between guideline indications and observed utilization highlights the variability in preoperative work-ups for gynecologic surgery.
A second discrepancy was the anticipated versus actual utility of preoperative testing. Approximately 50% of EKGs and 15% of CXRs showed abnormal findings. EKG abnormalities did not reflect acute cardiac issues. In fact, the clinical significance of most of these abnormalities was unclear. Abnormal screening results should prompt specific testing to confirm or refute a diagnosis. However, additional testing or specialist consultations occurred for only 20% and 10% of patients in this cohort, respectively. This suggests that abnormalities found on screening tests performed without specific clinical indications might have minimal impacts on decisions regarding surgical preparation, and, thus, would have limited clinical relevance.
The current findings support the limited available literature on preoperative evaluation in gynecologic surgery, which shows that 90% of women undergo at least 1 nonindicated test, with 64% of EKGs and 99% of CXRs classified as “inappropriate.” 9 Rates of nonindicated preoperative testing across specialties is reported to be as high as 99%, with rare management changes in response to abnormal test results and poor correlations with perioperative complications.4,10–11 Excessively broad applications and lack of appropriate responses to positive results suggest that EKG and CXR might not be useful screening tests.
It is important to consider the detriments of preoperative screening with EKGs and CXRs when abnormal test results have unclear clinical significance. There are no guidelines describing how specific test abnormalities should influence management. For patients who do undergo further evaluation, follow-up testing can be costly, uncomfortable, and time-consuming. Indeed, 3 patients in the current study experienced delays of up to 4 months while awaiting additional work-ups with ultimate completion of surgery.
Unnecessary preoperative testing also comes at a cost. At one institution, the cumulative cost of nonindicated preoperative tests before gynecologic surgery exceeded $418,000 across 2 years. 9 In a Canadian hospital where preoperative EKG rates were as low as 2.7% prior to hysterectomy and preoperative CXR averaged 11.7% across specialties, costs of these 2 tests totaled $369,000 and $637,000, respectively, over 2 years. 11 Authors of published estimates claim that preoperative work-up costs the United States up to 3 billion dollars annually. 9
The current study was limited by the use of convenience sampling. The current authors acknowledge that the study's limited sample size might not have captured the rare “sick” patient or uncommon surgical complications predicted by preoperative testing, given the low incidence of these events over the course of a single year. Information regarding surgical planning was limited to what was documented in the patients' electronic medical records. The current authors believe that most readmissions were accounted for through the “Care Everywhere” program, given that the current authors' institution primarily cares for residents of their county, but patients might have sought postoperative care at hospitals outside of this network. Additionally, although preoperative testing can serve to reassure the surgical team of a patient's health status, this was not a measurable outcome in this study. Similarly, downstream effects on long-term health management were not assessed.
Conclusions
Regardless of guideline concordance, EKG and CXR in this sample provided little clinical utility in terms of modifying preoperative risk prior to hysterectomy for benign indications. These tests did not change perioperative management significantly or correlate with surgical complications. Given the widespread utilization of preoperative testing nationally, the current authors anticipate that these study findings have high external validity. Limiting indications for preoperative screening EKG and CXR in otherwise low risk patients could offer an opportunity to reduce over-testing, avoid potential patient harms, and reduce costs.
Footnotes
Acknowledgments
Thank you to the Parkland Center for Healthcare Innovation and Clinical Outcomes Studies, Dallas, TX, for its support of this study.
The findings in this article were presented as an oral poster at the Society of Gynecologic Surgeons, 44th Annual Scientific Meeting, in Orlando, FL, on March 12, 2018, and at the American Association of Gynecologic Laparoscopists, 47th Global Congress on Minimally Invasive Surgery, Las Vegas, NV (November 11–15, 2018) on November 14, 2018.
Author Disclosure Statement
No financial conflicts exist.