
Abstract
Abstract
Background:
Caesarean scar pregnancy (CSP)—or isthmocele—is a rare form of ectopic pregnancy that usually is diagnosed by early pregnancy transvaginal ultrasound (TVUS) imaging.
Case:
A 33-year-old, gravida 4, para 2, alive 1, patient was diagnosed with a CSP at 7 weeks and 2 days' gestation, with TVUS signs of dense and abundant vascularization. Uterine arterial embolization (UAE) was first performed, followed by laparoscopic resection with repair of the defect, both procedures accomplished in one session of anesthesia.
Results:
This surgery was nearly bloodless and successful. The patient's human chorionic gonadotropin level became negative within 3 weeks.
Conclusions:
The natural course of CSP is a matter of controversy; however, most researchers agree with active management because of the significant risk of hemorrhage. Laparoscopic excision and repair have high success rates. Furthermore, UAE reduces the risk for hemorrhage strongly. This is the first report in the literature combining these two techniques in one general operative session. This approach could be an interesting addition to the various treatment options.
Introduction
Cesarean scar pregnancy (CSP), also referred to as isthmocele pregnancy, is a unique kind of ectopic pregnancy. It is estimated that 1 in 531 women with cesarean scars will develop a CSP. 1 The exact prevalence of CSP is unknown but is estimated to be between 1% and 4.2% of all ectopic pregnancies. CSP is more frequent in women with a history of two or more cesarean deliveries. Because of the increasing number of cesarean sections in the last decade, the incidence of CSPs has consequently risen and will probably continue to do so.1–3 This report presents a case in which uterine arterial embolization (UAE) combined with laparoscopic management was used in the management of a woman with a CSP to reduce intraoperative bleeding.
Case
A 33-year-old woman, gravida 4, para 2, alive 1, was referred at 7 weeks and 2 days' gestational age because of an ongoing CSP that was first suspected at a gestational age of 6 weeks and 6 days. She had undergone one previous termination of a pregnancy at 12 weeks' gestational age for a cytomegalovirus seroconversion, and then she had undergone two consecutive cesarean sections at term. Otherwise, her history was unremarkable, except for one episode of pyelonephritis. This patient denied any medication use. The presence of a niche was unknown prior to this index pregnancy. She was asymptomatic apart from morning nausea (i.e., she was normotensive, had a normal pulse, and had no abdominal tenderness).
Transvaginal ultrasound (TVUS) confirmed that she had a CSP, with a gestational sac protruding through the uterus, without an overlaying myometrial layer, and in contact with the bladder. The sac measured 29 × 8 × 12 mm, had a fetal pole of 11.3 mm (gestational age: 7 weeks and 2 days), and the embryo had a heartbeat (Fig. 1). A highly-vascularized network (International Ovarian Tumor Analysis color score 4) around the pregnancy was visualized by power Doppler examination. Given that the vascularization was quite impressive, an interventional radiologist was consulted about the potential of performing UAE first, followed by primary laparoscopic resection and cesarean-scar repair.
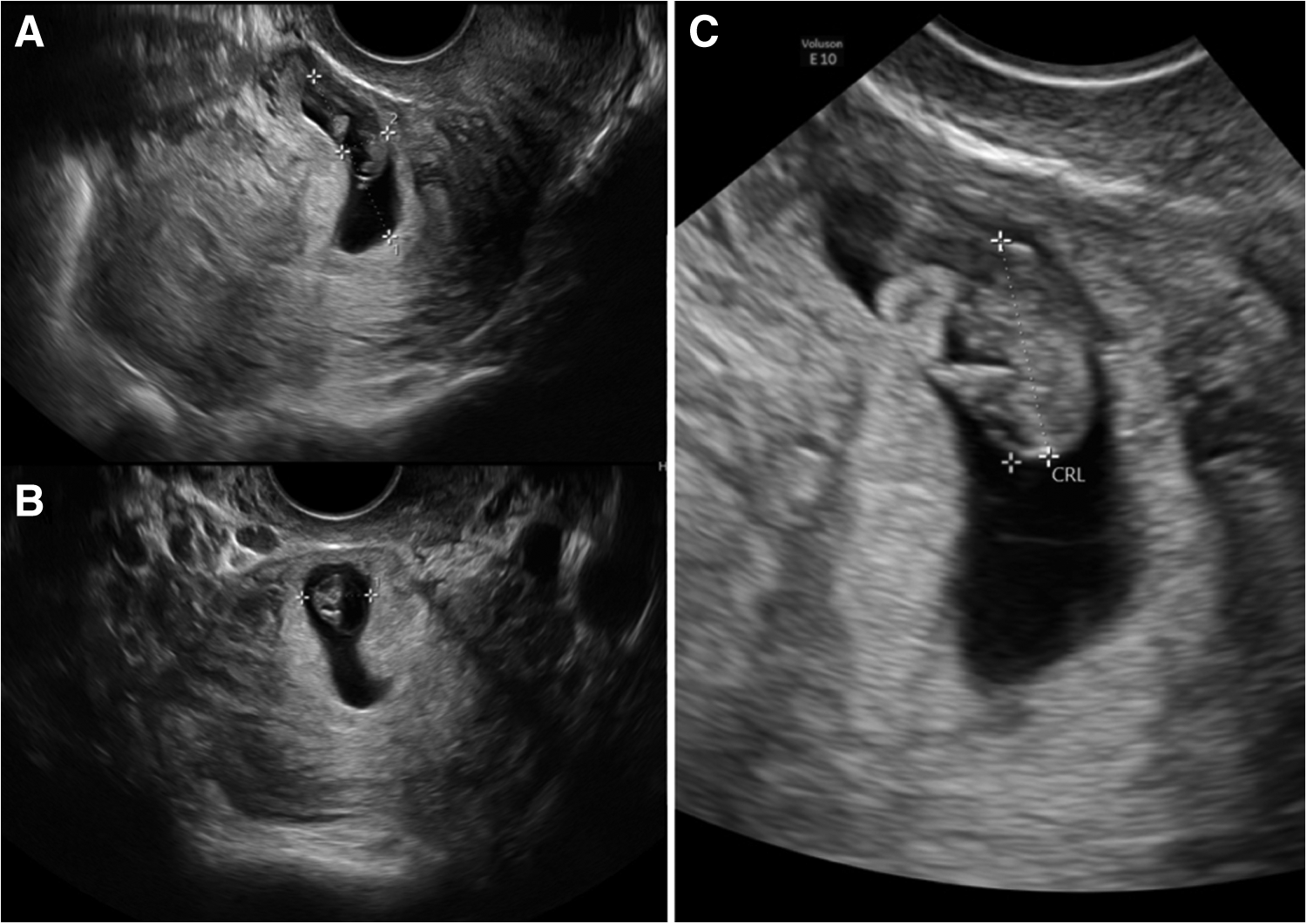
Transvaginal ultrasound (US).
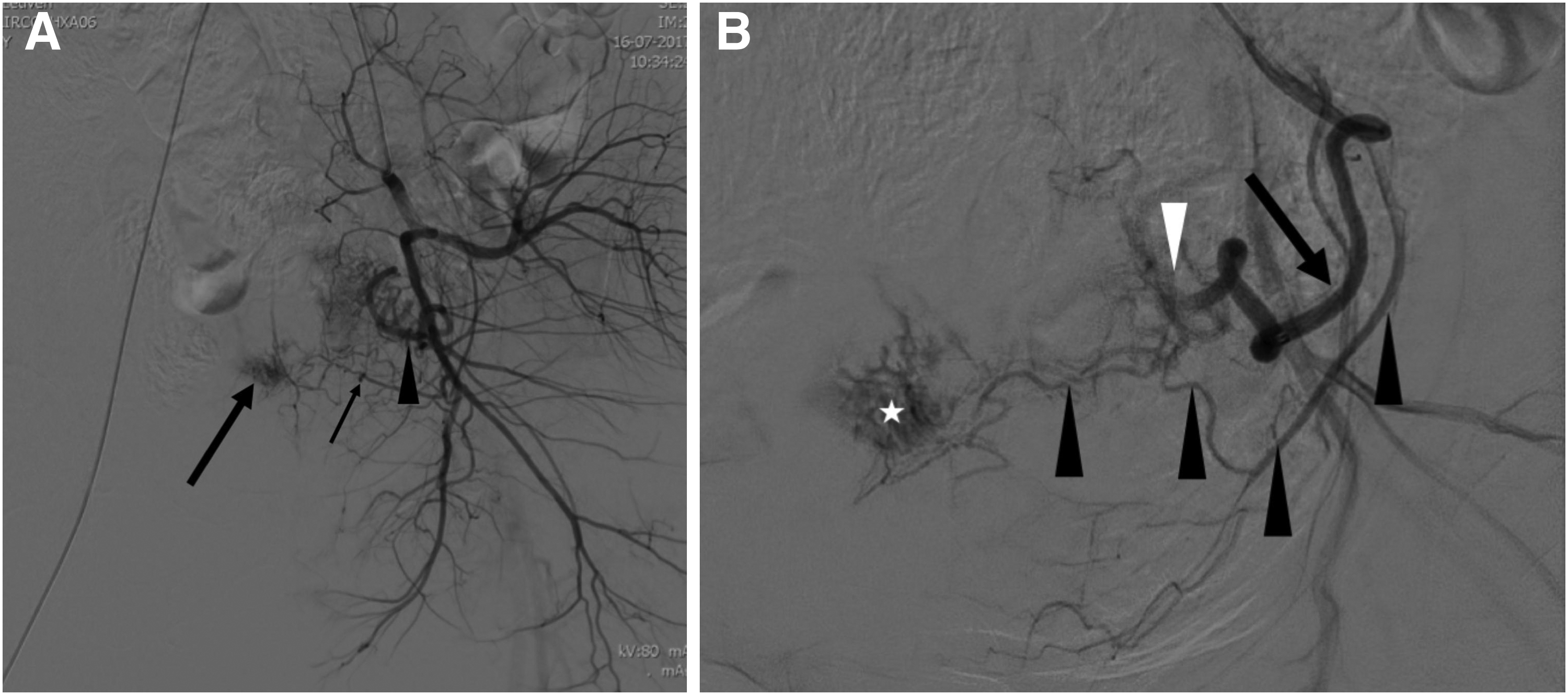
Under general anesthesia in a single operative session, both uterine arteries and the ascending branch of the vesical artery were embolized with trisacryl gelatin microspheres (Embosphere,® 500–700 μm, Merit Medical Systems) in an interventional radiology suite (Fig. 2). The latter vessel had been feeding the inferior aspect of the uterus. Once this was accomplished successfully, laparoscopic resection of the CSP was performed. The broad ligaments were opened and a bladder flap was raised to expose the uterine scar and pregnancy. This procedure was nearly bloodless. Laparoscopic resection and repair of the dehiscent area were performed with polyglactin 910 2/0 (Vicryl,® Ethicon) and polydioxanone 0 (PDS,® Ethicon). The total duration of the laparoscopic resection and repair was 3 hours. Intraoperative blood loss was minimal (a hemoglobin decline of 25 g/L).
Results
The patient was discharged from the hospital the following day. Her serum human chorionic gonadotropin (hCG) level dropped rapidly and normalized by day 25.
TVUS at 6 weeks after these interventions showed no dehiscence at the level of the uterine scar nor any residual trophoblastic tissue. The scar had a thickness of 3.9 mm. A pathology report on the excised specimen showed that there had been normal placental and embryonal tissue, as well as a minimum of myometrial tissue.
Discussion
Forty percent of patients with CSP present with painless vaginal bleeding; yet, the majority of such patients are asymptomatic.4,5 Therefore, a high index of suspicion for CSP is necessary for an adequate diagnosis. 2 As with any ectopic pregnancy, serum hCG and gynecologic TVUS findings will help determine what further management should be attempted. 2 Criteria on an early TVUS include the presence of a viable gestational sac in the lower uterine segment, thin-to-absent overlaying myometrium, prominent vascularization at the site of implantation, and an empty uterus and cervical canal.1,2,5
The natural course of CSP is a matter of controversy. 6 CSP is managed as a typical ectopic pregnancy because of the potential for severe complications. These include a morbidly adherent placenta, uterine rupture, and hemorrhage.2,6 To prevent these events, most cases diagnosed in the first trimester are terminated shortly after diagnosis.2,3,6
There are several medical management options for CSP. Yet, as single strategies, they are often insufficient. Maheux-Lacroix et al. systematically reviewed the literature and reported a 56%–77% success rate. 3 Laparoscopic excision and repair of the defect in one procedure had a high success rate of 97%. Furthermore, the addition of UAE to surgical evacuation reduced the risk for hemorrhage from 18% to 3%. 3 Based on the latter observation, we opted for prior UAE with surgical management in this patient, who presented with a CSP and had TVUS signs of strong vascularization. To our knowledge this combined approach had not yet been reported in the literature on CSP.
Conclusions
CSP is a rare condition that is often diagnosed early with screening TVUS. To prevent complications later in pregnancy, CSP is typically managed actively. Surgical therapy is effective. Currently, UAE is a widely available tool and may reduce intraoperative hemorrhage. In this article, we combined the use of UAE and surgery in a case with strong vascularization, which may have contributed to a nearly bloodless surgery.
Footnotes
Acknowledgments
This case report was exempted from institutional review board approval within University Hospitals Leuven. Formal informed consent for publication was obtained from the patient in writing by Bart Bronselaer, MD.
Author Disclosure Statement
No financial conflicts of interest exist.