
Abstract
Objective:
Avoiding surgical delay in the operating room (OR) is essential to provide timely, safe, and cost-effective care. The objective of this study was to identify the causes of OR delays and assess trends related to surgical specialties or approaches.
Materials and Methods:
This retrospective study included all elective gynecology (Gyn), general surgery (GS), and urology (Uro) surgeries performed during a 12-month period. Operative case details, surgical times, and reasons for delays were retrieved from a perioperative database. Representative specialty-specific procedures (hysterectomy, colectomy, nephrectomy) were chosen and compared separately to assess trends in delays.
Results:
A total of 4206 surgeries were completed during the study period; of which 1447 (34%) were Gyn, 2226 (52%) GS, and 533 (12%) Uro. Delays occurred in 1010 Gyn (70%), 1304 GS (59%), and 225 Uro cases (48%). The most-common reason for delay was case-related—delays in case due to delays in prior cases—(n = 1171 [28%]), followed by patient-related delays (n = 458 [11%]), then delays in patient preparedness (n = 340 [8%]). These rates of delay frequency were similar across representative specialty-specific procedures. Delays were more frequent when comparing laparoscopic to open colectomy (38/51, 75% versus 24/25, 96%; p = 0.02), whereas there was no significant difference in delays between laparoscopic and open hysterectomy (162/198, 82% versus 50/68, 74%; p = 0.07) or nephrectomy (4/7, 57% versus 35/76, 46%; p = 0.70).
Conclusions:
This study suggests that among specialties and cases, the most-common cause of delays was case-related. These findings provide a platform from which to introduce quality-improvement initiatives. (J GYNECOL SURG 36:109)
Introduction
Efficiency in the operating room (OR) is essential for both hospitals and health care systems in order to provide timely, safe, and cost-effective care to patients. However, various studies have shown that there are significant inefficiencies and delays within ORs.1,2 A surgical delay is defined as an operation that does not start on or before schedule, and that has been shown to increase surgical wait times, number of cancelled cases, costs, and time under anesthesia. 1 In addition, although delays and disruptions to workflow can be minor, the accumulation of delays can create provider stress and fatigue, and ultimately lead to errors.3–5 Several studies have shown that sources of delay are multifactorial. These include issues related to equipment, instruments and/or supplies, patients and staff, communication, administration, bed availability, environmental events, and intraoperative complications. 6
Understanding the most common reasons for time delays and the frequency of which they occur can help prevent delays by being prepared; that is, anticipating the potential for delays and having plans to minimize inefficiency. The majority of studies have looked at the preoperative and changeover times as targets for increasing OR efficiency. 7 Additionally, there have been several prospective studies measuring delays; these studies have relied on subjective reporting of 1 surgeon, 1 1 OR nurse, 8 or research personnel. 9 Hence, most surgical case delay tracking is performed by a member of the surgical team. The subjectivity of this process makes it susceptible to inconsistency and bias. There is, therefore, a need to observe and evaluate case duration objectively, as well as also exploring care-related factors that might contribute to delays.
Objectives
The main objective of this study was to identify the causes of OR delays at an urban tertiary-care hospital. Secondary objectives were to identify if there were patterns in the types of delays related to surgical specialties or surgical approaches (i.e., open, laparoscopic, robotic, or vaginal).
Materials and Methods
Design
This study was a retrospective study created to assess perioperative delays across 3 specialties gynecology (Gyn), general surgery (GS), and urology (Uro), at an urban tertiary-care academic hospital. The protocol for this study was approved by the research ethics board of St. Michael's Hospital (16-264), in Toronto, Ontario, Canada.
Inclusion criteria
All elective surgical procedures in the departments of Gyn, GS, and Uro, from July 1, 2015 through June 30, 2016, inclusive were included in the analysis. All emergency cases, including cases that occurred on weekends or evenings, were excluded.
Data collection
Data were retrieved from an electronic perioperative management system database. The database is maintained by OR nursing staff, who prospectively record delays, operative case details, and surgical times on a standardized perioperative delay form. The perioperative database requires delays to be categorized into 7 root causes: (1) bed availability (when there was no destination bed for a patient); (2) case-related (when a previous case was delayed, there was a prolonged setup time, or a case was bumped); (3) patient factors (when there was a delay in bringing a patient to the OR due to transportation issues or the patient was unavailable); (4) patient unpreparedness (critical bloodwork or workup was not performed); (5) staff factors (the OR staff were delayed or unavailable); (6) equipment, instrument and/or supplies (key supplies for the case were unavailable); and (7) prolonged case time (due to unforeseen complications, incident reports, or environmental factors). Figure 1 shows the sheet used to report on such delays. In addition, the number of elective cases for each specialty that were cancelled due to insufficient time during the study period was tabulated.

Delay tracking sheet utilized by nursing staff to track and characterized various reasons for delay during a surgical case. ICU, intensive care unit; PACU, postanesthetic care unit; DSU, day surgery unit; PT, patient; NPO, nil per os; IV, intravenous; MDRD, medical device reprocessing unit; PSA, patient service associate; RN, registered nurse; TA, technical assistant; USW, unit support worker.
Data analysis
Type of surgery, specialty, American Society of Anesthesia (ASA) class, and approach (open, laparoscopic, robotic, or vaginal) were extracted from the electronic perioperative management system for all relevant cases that occurred in the OR during the study period. A representative specialty-specific procedure (hysterectomy, colectomy, nephrectomy) was chosen for each specialty. These procedures were chosen to be as similar as possible in complexity by surgical experts in the study team (E.S., V.P., and J.L.). These procedures were compared separately to assess the delay patterns.
Statistical analysis
Data were retrospectively collected, including surgical times, procedure types, and delay codes. Data were analyzed in statistical software IBM SPSS, version 25. Continuous variables (time) were described using medians and interquartile ranges; categorical variables (surgical routes, reasons for delays) were described using frequencies and proportions. Categories of delays were evaluated descriptively across procedures and specialties. The Mann–Whitney nonparametric test was used to compare case times between different surgical routes (e.g., open versus minimally invasive). The χ 2 test (or Fisher's exact test when there were small counts) were used to evaluate factors such as surgical approaches and case delays. Kruskal–Wallis tests were used to compare ASA values among 3 surgery types.
Results
A total of 4206 surgeries were completed by the departments of Gyn, GS, and Uro, of which 1447 (34%) were Gyn, 2226 (52%) were GS, and 533 (12%) were Uro. The median ASA class was for 2 for Gyn, 3 for GS, and 2 for Uro, and there was a statistically significant difference in ASA among the specialties (p = 0.001)
Frequency and type of delay within each specialty
Delays occurred in more than half of the cases in Gyn (n = 1010 [70%]) and GS (n = 1304, [59%]) and approached nearly half of the cases in Uro (n = 255 [48%]). The most-common reason for delay across all specialties was case-related delays (n = 1171 [28%]), followed by patient-related delays (n = 458 [11%]), then patient unpreparedness (n = 340 [8%]). See Table 1. Similarly, within each specialty, case-related delays were the most-common, followed by patient-related delays, then patient unpreparedness (Table 1).
Frequency and Types of Delay Within Each Specialty

The shaded area indicate the 3 most common reasons for delays.
Gyn, gynecology; GS, general surgery; Uro, urology.
Delay trends in each specialty's representative procedure
Over the study period, there were 266 hysterectomies, 76 colectomies, and 83 nephrectomies.
The median ASA class for each type was 3 for colectomy, 2 for nephrectomy, and 2 for hysterectomy, and there was a statistically significant difference in ASA among the specialties (p < 0.001).
Delays occurred in 217 (82%) of hysterectomies, 62 (82%) of colectomies, and 39 (47%) of nephrectomies (p < 0.001). For each procedure the three most-common causes of delays were case-related, patient-related, and patient unpreparedness (Table 2).
Delay Trends in Each Specialty's Representative Procedure
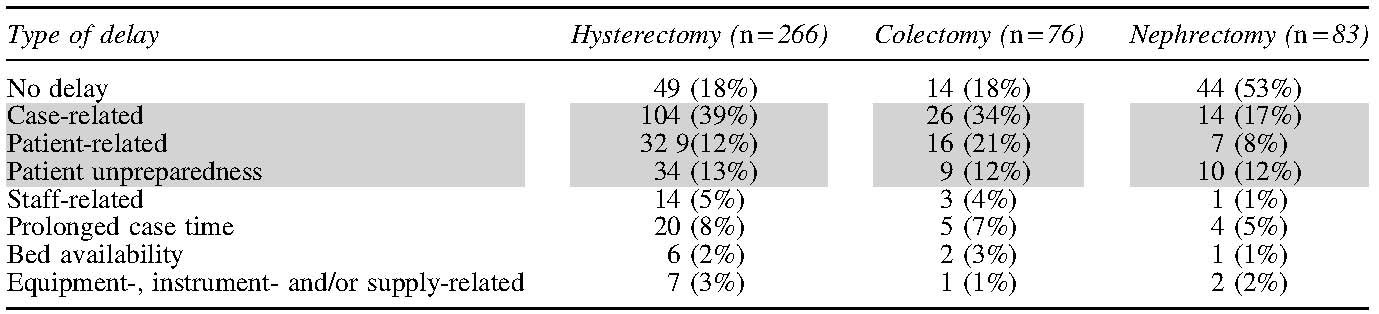
The shaded area indicate the 3 most common reasons for delays.
Delays comparing open and laparoscopic approaches
Of the 266 patients who had hysterectomies, 198 (74%) were performed via a minimally invasive surgical approach, and 5 (3%) were converted to open surgery. There was no significant difference in the frequency of delays among minimally invasive (vaginal hysterectomy, laparoscopic-assisted vaginal hysterectomy, total laparoscopic hysterectomy, total robotic hysterectomy; 162/198, 82%), and open hysterectomy (50/68, 74%). For these approaches, p = 0.059.
Of the 76 patients who had colectomies, 51 (67%) were performed laparoscopically, with 6 cases (8%) converted to open surgeries. Twenty-five (33%) were performed with an open technique. Delays were significantly more common when colectomy was performed via laparotomy (24/25, 96%), compared to laparoscopy (38/51, 75%). For these, p = 0.028.
Of the 83 patients who had nephrectomies, 75 (86%) were performed laparoscopically, 1 case (1%) was performed robotically, and 4 cases (5%) were converted to open surgeries. Seven (8%) were performed with an open technique. No significant difference in delays was found among nephrectomies performed via laparotomy (4/7, 57%) or minimally invasively (35/76, 46%). For these procedures, p = 0.701.
ASA and delay
One hundred- and seventy-eight-women undergoing hysterectomy had low-risk ASA class (ASA 1 or 2) and 8 women had high ASA class risk (ASA 3 or 4). Patient-related delays (patient and patient preparedness) for women undergoing hysterectomy were significantly higher for patients with high ASA class (33% delayed), compared to low-risk ASA class (21% delayed) For ASA, p = 0.031.
There was no association between ASA class and delay for any reason for colectomy (p = 1.00) and urology (p = 0.221).
Cancelled cases
During the study period, there were 84 cases cancelled due to insufficient time, Gyn (n = 45, 54%), GS (n = 28, 33%), and Uro (n = 11, 13%).
Discussion
Delays occurred in a significant number of cases across specialties, ranging from 48% of Uro cases to 70% of Gyn cases. The most-common reason for delay was case-related. This refers to a situation in which a delay in a previous case affects the start time of the subsequent case, a change in case order, or a case being bumped for an emergency case. The other most-common causes of delays were related to factors occurring prior to the patient coming to the OR (patient-related delays or patient unpreparedness). These trends in delays were found across all specialties and also in a subanalysis of elective cases per specialty.
These findings were somewhat different than previous reports in the literature. Other researchers have found that the most-frequent cause of delay was due to lack of patient preparedness (23%) followed by staff availability. 10 Panni, et al. similarly noted that common delay trends included: surgeon unavailability (19%); missing paperwork (16%); schedule changes (14%); and anesthesia delay (11%). 11 Other work has focused on decreasing turnaround-time delay rather than intraoperative delays as their primary outcomes to improve.12–14 This reflects the current study's finding that the most-common cause of delay was related to a delay in a previous case. Indeed, Wong et al. showed that there were significantly more delays in second and third cases if the first case of the day was delayed. 1 Additionally, Does et al. looked at start times and showed that first cases started an average of 40 minutes late. 15 Perhaps the most-similar study to the current patient population looked at 3 tertiary-care urban centers and timing of the first case. 16 These researchers found that patient placement in the OR was delayed in 88% of their first cases and that 60% of delayed cases had no documented reasons for delay. Strategies to improve OR efficiency must be targeted to the ensuring that the first case starts on time.
No association was found between delay (for any reason) and surgical approach (minimally invasive versus laparotomy) for hysterectomy or nephrectomy. This suggests that, at least for these procedures, the equipment-related differences in surgical approaches do not have an impact on surgical delays. Interestingly, however, delays were significantly more common when colectomy was performed via laparotomy (96%) compared to laparoscopy (75%; p = 0.02), suggesting that there might be differences in surgical techniques, equipment setups, and complexity among specialties.
The effect of ASA class on delay differed across specialties. While the current study found no association between ASA class and delays in colorectal cases; in gynecology, patients with lower ASA classes had a higher likelihood of delays, compared to patients with higher ASA classes. This may be due to several factors. First, surgeons booking cases might preemptively book more surgical time for medically complex cases, anticipating that the anesthesia portion of these cases might take longer. Second, more medically complex cases are usually booked first in the day. The current study's data showed that most delays were related to delays in the previous cases, and, as such, lower ASA cases might be disproportionally affected.
Limitations of the study included the following. First, the retrospective design only allowed for a certain amount of detail regarding the causes of the delays. For example, although the current authors could determine that a delay was case-related, due to the nature of the study design it was impossible to understand whether that was related to the case being bumped or not starting on time due to a delay in a previous case. Second, the categorization of delays was subjective and has the potential for bias. Finally, the case bookings are arranged by the surgeons' offices, and, although one can presume that the surgeons plan to finish all their cases within the OR day, it is probable, that the details of case length and booking time are not necessarily representative of the time that the surgeon plans to spend on each individual case, but rather the number of cases the surgeon can accomplish in the full OR day. The fact, however, that there were significant case cancellations during the study period indicated that not all case delays were related to scheduling and booking limitations.
Conclusions
This study demonstrated that, across specialties and cases, the most-common cause of delay is case-related delay. This aligns with previous literature stating the importance of the first case starting on time to reduce inefficiencies during the whole day in the OR.10,17,18 This is important, as it provides a platform from which to introduce quality-improvement initiatives. Focusing on starting the first case of the day at the correct time, as well as optimizing resources when case order changes or a case is bumped, has the potential for significant reductions in delays. Future prospective work focusing on flow throughout the whole day in the OR, rather than focusing on individual cases, will provide more data regarding causes and lengths of delays. This has the potential to improve workflow and efficiency in the OR significantly.
Footnotes
Author Disclosure Statement
V.P., A.S., J.L., and E.S. have no financial conflicts of interest.
G.Y. has received personal fees from Bayer and Hologic outside of the content of this article.
T.G. owns the intellectual property for Surgical Safety Technologies, Inc., and has received grants from Medtronic, Ethicon, Olympus, Karl Storz, Intuitive Surgical, Baxter, and Takeda.
Funding Information
Funding was provided by the St. Michael's Hospital Association Alternate Funding Plan Innovation Funds.