
Abstract
Objective:
Total salpingectomy is the “gold standard” treatment for tubal ectopic pregnancy. This procedure avoids the risks of persistent trophoblasts and recurrent ipsilateral tubal pregnancies but affects ovarian blood supply. Is distal partial salpingectomy, using an Endoloop® Ligature (made with polydioxanone II a, violet monofilament; Ethicon, Somerville, NJ) an easy and fast way to remove the tubal fimbria, without producing a thermal destructive effect? Is the procedure minimally associated with risks of persistent trophoblast and recurrent ipsilateral tubal pregnancies? Should distal partial salpingectomy be recommended for nonisthmic tubal pregnancy, especially in countries of low socioeconomic status?
Materials and Methods:
In this controlled, comparative observational trial, 54 women with ampullary or fimbrial tubal ectopic pregnancies underwent laparoscopic salpingectomy. The patients were divided into 2 groups of 27 patients each. Group 1 underwent distal partial salpingectomy, using an Endoloop Ligature and group 2 underwent the gold standard total salpingectomy, using bipolar diathermy. Primary outcomes were duration of operative procedure and intraoperative hemoglobin loss; secondary outcomes were recurrent ectopic pregnancy in the ipsilateral tube, persistent trophoblast tissues, and spontaneous intrauterine pregnancy later.
Results:
Use of an Endoloop Ligature was associated with significantly shorter operating times and less intraoperative hemoglobin loss. No cases of recurrent ectopic pregnancies in the ipsilateral tubes or persistent trophoblast tissues were reported in both studied groups. Seventeen (62.9%) and 16 (59.2%) women achieved spontaneous intrauterine pregnancies during the follow-up period in both groups, respectively.
Conclusions:
Performing distal partial salpingectomy using an Endoloop Ligature is a safe, rapid, and effective procedure, compared to electrosurgical total salpingectomy. Further studies are still needed to support distal partial salpingectomy as a recommended treatment. (J GYNECOL SURG 36:120)
Introduction
Ectopic pregnancy is an acute life-threatening condition; it is the leading cause of maternal death in early pregnancy. 1 Approximately 95% of ectopic pregnancies occur in the fallopian tubes. 2 Management of ectopic pregnancy can be expectant, medically with methotrexate, or surgically. 3 Ideally, most ectopic pregnancies can be treated medically, and surgical management is reserved for patients who do not fit the criteria for medical treatment or for whom such treatment has failed. For a limited number of conditions, patients can be managed expectantly.1,3 Most ectopic pregnancies are treated surgically. 3 The decision of whether to preserve or remove the tube when treating a woman who has a tubal pregnancy has been debated for many years; this controversy still remains.4–7 Laparoscopic salpingectomy is the “gold standard” procedure for addressing tubal pregnancy. 8 Salpingectomy requires securing hemostasis prior to excision of the diseased fallopian tube, using different hemostatic procedures. 9
The ovary is supplied by the ovarian artery and by the ascending branch of the uterine artery in the mesosalpinx. Lateral thermal spread from electrocoagulation on the tube during salpingectomy can lead to direct ovarian perfusion damage. 10 It is generally recognized that removal of a hydrosalpinx can increase the implantation rate of in-vitro fertilization (IVF) and embryo transfer (ET; IVF-ET).10,11 Some researchers have reported that salpingectomy reduces the ovarian blood supply and therefore compromises ovarian reserve.12,13 Ye et al. concluded in 2015 that salpingectomy is associated with decreased anti-Müllerian hormone level and increased follicle stimulation hormone in women seeking IVF, suggesting that salpingectomy is associated with decreased ovarian reserve. 13
Total salpingectomy of an ectopically implanted embryo is usually achieved by resection of the whole fallopian tube, including the remaining proximal healthy tubal segment. Partial salpingectomy means removing a segment of the fallopian tube that contains the ectopic gestation. However, partial distal salpingectomy means removing part of the tube from the fimbria to the proximal end of the ectopic swelling toward the uterine cornual side.
The idea underlying this current study arose from two issues regarding the literature. The first issue is the reports of decreased ovarian reserve after total salpingectomy in IVF-ET cases.9,10,13 The second issue is that recurrent ectopic pregnancy in the remnant portion of the fallopian tube after partial salpingectomy has rarely been reported, with only nearly 20 cases reported in the last 30 years.14–16
This study explored three concerns:
Removal of ectopic pregnancy tissue with an Endoloop® Ligature (made with polydioxanone II a, violet monofilament; Ethicon, Somerville, NJ), without electrocoagulation or thermal injury, and with a minimal incidence of recurrent ectopic pregnancies and the presence of persistent trophoblastic tissue in the ipsilateral portion of the fallopian tube8–10,14–17 Removal of the fimbria, which has been said to be the potential origin of ovarian cancer
11
Availability of recent expensive hemostatic instruments in countries that have low socioeconomic status, making these instruments difficult to obtain.
Consequently, the objective of the current trial was to assess if distal partial salpingectomy was effective, safe, and fast with a tourniquet hemostatic procedure for treating nonisthmic tubal pregnancies in countries of low socioeconomic status.
Materials and Methods
Study design and participants
In this controlled, comparative observational trial, 54 patients with nonisthmic tubal (fimbrial or ampullary) pregnancies received laparoscopic salpingectomies, from May 2015 to December 2018, in the department of obstetrics and gynecology, of Zagazig University Hospital, in Cairo, Egypt. The study was approved by the hospital's institutional review board. The procedures were performed by the same surgeon (M.F. Selim assisted by M.M.A. Abdou). The patients were counseled regarding partial distal salpingectomy using an Endoloop Ligature (group 1) or total salpingectomy using bipolar diathermy (group 2). Informed consent was obtained from all patients after providing a detailed description of each operative process and its possible associated complications.
All patients with tubal pregnancies who chose to have medical treatment with methotrexate or a conservative surgical procedure (salpingotomy) were excluded from the analysis. All cases of isthmic tubal pregnancy were also excluded from the study, as total salpingectomy was indicated in such case. The 54 cases that were eligible for the statistical analysis who included 27 cases in group 1 and 27 cases in group 2.
Ectopic pregnancies were diagnosed by evaluation of each patient's clinical history, gynecologic examination, transvaginal ultrasound (TVUS) results, and measurement of serum β–human chorionic gonadotropin (hCG) level. The ultrasound (US) had to show an extraovarian adnexal mass when ectopic pregnancy (amenorrhea, bleeding, and pain) was suspected, and the patient had to test positive for β-hCG.
Hemodynamically stable women with the presumptive diagnosis of tubal ectopic pregnancy, who were scheduled for laparoscopic salpingectomy, were eligible for inclusion. The laparoscopic procedure was performed as previously described by Pouly et al. 17 and Tulandi and Saleh. 18 Either an Endoloop Ligature or conventional bipolar diathermy was chosen to treat the tubal pregnancies per Moon et al.'s conclusions that the Endoloop Ligature is simple, safe, effective, and nearly bloodless. 19
At surgery, the presence of a tubal pregnancy had to be confirmed. A case was not eligible for the analysis if the condition of the patient's contralateral tube was unhealthy and rendered future fertility unlikely and, thus, she had to undergo salpingotomy. The decision that the a patient was eligible for a distal partial salpingectomy was made by the surgeon, based on intraoperative findings and the patient's previous consent to undergo that procedure. After surgery, all of the women were informed about which interventions they had received.
The three outcomes sought were: (1) risk of persistent trophoblast tissues; (2) risk of a repeated ectopic pregnancy; or (3) chance of an intrauterine pregnancy (IUP) within 18 months postoperatively.
The total operating time was recorded from the time that the surgeon made the intraumbilical incision until completion of the surgery by suturing the skin. All patients were discharged within 48 hours following surgery unless they had fever, persistent pain, or other intraoperative complications. A follow-up review was scheduled on the seventh postoperative day. Each patient was interviewed regarding complications or side-effects following her surgery. Serum β-hCG concentration was also assessed. Each patient's serum β-hCG concentration should have decreased by at least 50% on postoperative day 2 and by 75% on postoperative day 4; this measurement was repeated weekly until the serum β-hCG concentration dropped to a nonpregnant value. 12
To assess spontaneous pregnancy after surgery, the each patient was followed-up for 18 months. An ongoing pregnancy was defined as an intrauterine pregnancy visible on US at a gestational age of 7 weeks or more with fetal cardiac activity. The time to the first ongoing pregnancy was calculated in months, from the date of surgery to the first day of the last menstrual period before the ongoing pregnancy. If an ongoing pregnancy did not occur, follow-up ended on the last date of contact, or when either IVF or reconstructive tubal surgery was performed. Persistent trophoblastic tissue was defined as rising or plateauing serum β-hCG concentrations postoperatively that necessitated systemic methotrexate treatment or surgical intervention. 4 Diagnosis of suspected persistent trophoblastic tissue was made 2 and 4 days postoperatively according to the criteria noted above. Repeated ectopic pregnancy was defined as any ectopic pregnancy either in the remaining distal part of the ipsilateral fallopian tube or in the contralateral fallopian tube.
Operative technique
All procedures were performed with each patient under general anesthesia. Each patient was placed in the lithotomy position. Pneumoperitoneum was achieved using a Veress needle inserted through the umbilicus, and CO2 insufflation was performed up to an intra-abdominal pressure of 14 mm Hg. Then, a 10-mm trocar was inserted in the same umbilical location for the optic system. Under direct visualization, 2 ancillary trocars were inserted into the left and right lower abdominal quadrants lateral to the inferior epigastric arteries (1 10-mm trocar and 1 5-mm trocar). In cases of hemoperitoneum, aspiration and washing of the pelvis was performed with saline solution under pressure using the Hamou Endomat (Karl Storz Endoscopy Japan K.K., Tokyo, Japan). The amount of aspirated hemoperitoneum before starting the salpingectomy was not counted in the estimation of intraoperative blood loss. First, the ectopic mass was localized by pelvic and abdominal visualization. Using atraumatic grasping forceps, the fallopian tube was manipulated by grasping the serosa to delineate the portion to be excised.
Then, salpingectomy was performed for group 1 using an Endoloop Ligature. Salpingectomy was accomplished by application of the Endoloop over the mesosalpinx and broad ligament of the affected part of the fallopian tube (partial distal salpingectomy). The loop was placed under the mass on the uterine side so that the removed part was from the fimbria through the end of the conceptus swelling in proximal end of the fallopian tube near the uterine side. Hemostasis was achieved by looping the ligature over the affected fallopian tube under direct vision and advancing the plastic sheath to tighten the pretied knot. The ligature was easy to use and quickly achieved hemostasis with an excellent tourniquet effect. There was no risk of thermal injury with this technique. The tubal pregnancy was then excised with laparoscopic scissors. Adequate bleeding control of the ectopic mass was established by double Endoloop suturing. The abdominal cavity was thoroughly irrigated and explored (Fig. 1) to confirm proper hemostasis.
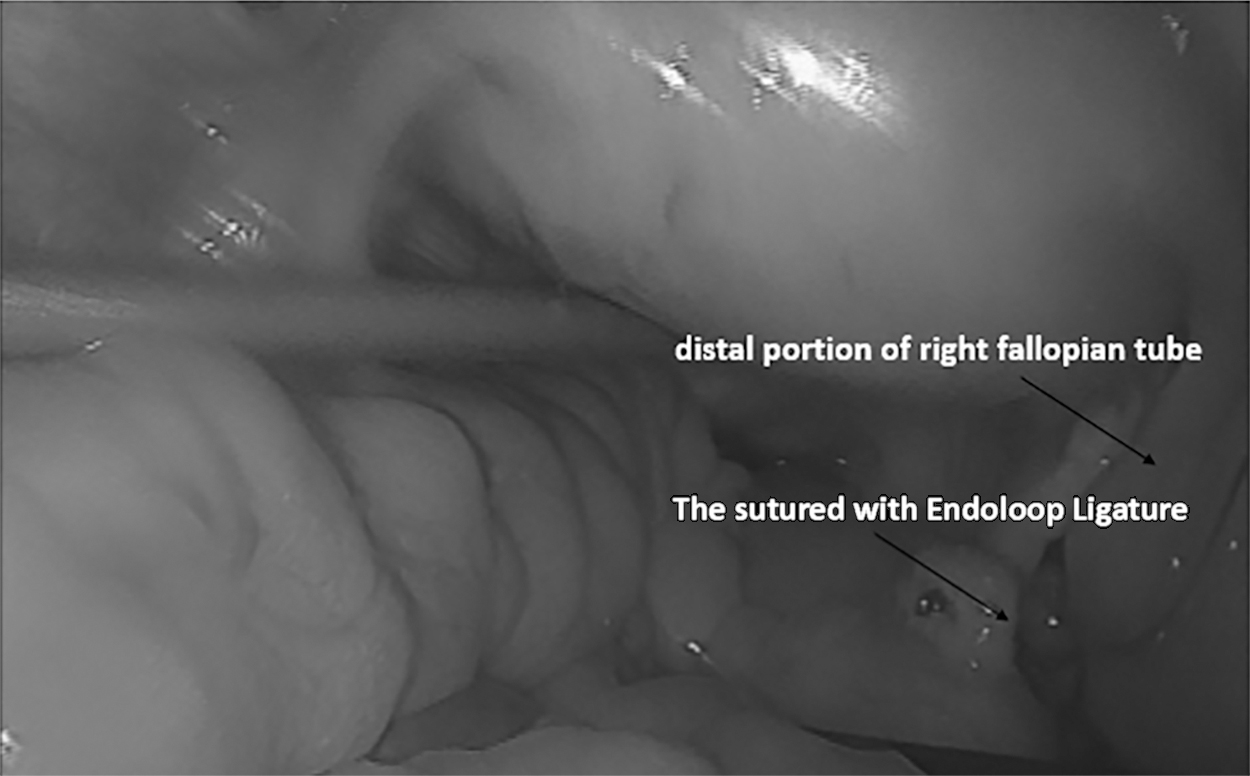
Fallopian tube post partial distal salpingectomy. Sutured with an Endoloop® Ligature (made with polydioxanone [PDS] II a, violet monofilament; Ethicon, Somerville, NJ).
For patients in the electrosurgery group (group 2), salpingectomy was performed by using bipolar electrosurgical forceps designed by Kleppinger (Karl Storz Endoscopy Japan K.K.), powered by a Force 2 or 40 electrosurgical generator (Valley Lab, London, UK). The procedure involved progressively coagulating and cutting the mesosalpinx, beginning from the isthmic portion of the fallopian tube and progressing to the fimbriated end of the tube. Salpingectomy was started by thermocoagulation and transection of the affected tube, then mesosalpinx was thermocoagulated and transected with numerous bites of 1 to 2 cm going to the tubo-ovarian ligament, which was also thermocoagulated and cut. A thorough check of hemostasis was confirmed at the end of the procedure.
After either procedure, the excised part of the fallopian tube containing products of conception was removed through a 5- or10-mm trocar sleeve or the tissue was be placed in an endoscopic bag and removed from the abdominal cavity. The amount of intraprocedural blood loss was calculated as follows:
Postoperative hemoglobin decrease was calculated by checking the difference between preoperative hemoglobin level and 24-hour postoperative level.
Statistical analysis
Statistical analysis was carried out using SPSS ver. 20 (SPSS Inc., Chicago, IL). After an assessment of normal distribution, data were presented as the mean ± standard deviation (SD) or the median (range) for quantitative variables. Qualitative variables were presented as the frequency (percentage). Continuous variables were compared using Student's t-test or Pearson's correlation. Categorical data were analyzed using a χ 2 test or Fisher's exact test. The differences were considered to be significant if p was <0.05.
Results
During this study, 98 patients were diagnosed with tubal pregnancy. Twenty-three cases were successfully treated medically with methotrexate. For the other 75 surgically treated cases, 3 of them had laparotomies for hemodynamic instability and 72 cases underwent laparoscopy. Laparoscopic total salpingectomy had been performed in 18 cases (3 cases for isthmic tubal pregnancy and 15 cases of patients who refused to participate in the study). The remaining 54 patients who had agreed to participate in the study were enrolled in the 2 studied groups. During the follow-ups after successful treatment, 17 and 16 patients achieved spontaneous pregnancies in groups 1 and 2, respectively. No patients developed recurrent tubal pregnancy in the ipsilateral fallopian tube; yet 1 patient in group 1 had recurrent tubal pregnancy in the contralateral fallopian tube. Persistent trophoblastic tissues were not detected in any of the 54 patients.
The demographic characteristics of the study population are shown in Table 1. There was no significant difference between the 2 groups at the time of surgery, including the patients' age, body mass index. and parity. Three patients (11.2%) in each group had histories of tubal disease previously diagnosed either by laparoscopy or hysterosalpingography. In group 1, 1 patient (3.7%) had a history of a previous ectopic pregnancy, while another 2 patients (7.4%) had intrauterine contraceptive devices in situ, and 4 patients (14.8%) had infertility. There was a nonsignificant difference with group 2, which had no cases (0%) of previous ectopic pregnancies, another 3 patients (11.2%) had intrauterine contraceptive devices in situ, and 5 patients (18.5%) had infertility. Yet, 17 (62.9%) patients and 16 (59.2%) patients were without any histories suggesting risk factors for developing ectopic pregnancies in groups 1 and 2, respectively.
Preoperative Characteristics of the 54 Tubal Pregnancy Cases Treated with Laparoscopic Partial Distal Salpingectomy
Values are represented as the mean ± SD (interquartile ranges) or, number (%).
All characteristics were nonsignificantly different in both studied groups.
Made with polydioxanone II a, violet monofilament; Ethicon, Somerville, NJ.
yrs, years; d, day(s); SD, standard deviation; β-hCG, beta human chorionic gonadotropin
Table 1 also shows no significant difference between the 2 groups with respect to clinical presenting symptoms as pelvic pain, vaginal bleeding, and both pelvic pains associated with vaginal bleeding. Yet, 1 case (3.7%) was discovered accidently while the patient, without complaints, presented for a checkup in group 1, and there were 2 such cases (7.4%) in group 2. The US findings of the enrolled cases revealed adnexal masses in all 54 cases (100%). The mean ± SD for size of the adnexal masses was 4.1 ± 1.7 cm with embryonic fetal heart pulsation detected in 3 cases (11.2%) in group 1. The mean ± SD for size of the adnexal masses was 3.4 ± 1.9 cm with embryonic fetal heart pulsation detected in 2 cases (7.4%) in group 2. US showed hemoperitoneum in 23 cases (85.2%) and 24 cases (88.8%) in groups 1 and 2, respectively.
The mean ± SD for durations of gestation based on the first day of last menstrual period were 55.3 ± 7.9 and 50.9 ± 8.2 days and the median preoperative serum β-hCG levels were 3247 ± 1454 and 3304 ± 1274 mIU/mL in groups 1 and 2, respectively. The mean ± SD for the preoperative hemoglobin content were 10.4 ± 2.7 and 10.7 ± 1.9 g/dL for groups 1 and 2, respectively without significant differences in both groups.
The indications for surgery, as shown in Table 1, in groups 1 and 2, respectively, were serum β-hCG level >10,000 mIU/mL in 4 patients (14.8%) and in 5 patients (18.5%); positive embryonic cardiac pulsation in 3 patients (11.2%) and in 2 patients (7.4%); an adnexal mass ≥3.5 cm in 22 cases (81.4%) and in 20 cases (74.1%). A suspicion of marked hemoperitoneum was the indication for surgery in 23 patients (85.2%) in either group. The indication of surgery was failure of methotrexate treatment in 1 patient (3.7%) no patients in groups 1 and 2, respectively, and contraindication for methotrexate therapy in another 5 patients (18.5%) in group 1 and 3 cases (11.2%) in group 2.
Operative characteristics of both groups are shown in Table 2. The number of patients who had ampullary tubal pregnancy were 24 (88.8%) and 22 (81.5%) and fimbrial pregnancy were 3 (11.2%) and 5 (18.5%) in groups 1 and 2, respectively. At the beginning of surgery 25 cases (92.6%) had tubal rupture and another 2 cases (7.4%) had intact tubes in similar numbers in both groups. The amounts of intraprocedural hemorrhage calculated at the end of the operations were significantly different in both groups as ranges between 50 mL and 530 mL in the Endoloop group (group 1), compared to ranges between 80 mL and 1250 mL in the electrosurgical group (group 2) at p < .05). The Endoloop group had a significantly shorter operating time (25 ± 12.4 minutes) ranging between 18 and 42 minutes, compared to the electrosurgical group (35 ± 17.2 minutes) ranging between 28 and 81 minutes (p < 0.05).
Operative Characteristics of the 54 Tubal Pregnancy Cases Treated with Laparoscopic Partial Distal Salpingectomy
Values are represented as the mean ± SD (interquartile ranges) or, number (%).
Made with polydioxanone II a, violet monofilament; Ethicon, Somerville, NJ.
Intraprocedural hemorrhage (mL) = total amount of aspirated fluid – amount aspirated before salpingectomy technique – amount of fluid used during the procedure.
Hemoglobin decrease is defined as the difference between preoperative hemoglobin level and day 1 postoperative hemoglobin level.
β-hCG resolution duration is defined as the period from date of surgery till the date of achieving a serum β-hCG level <5 mIU/mL
CI, confidence interval; min, minutes; d, day(s); β-hCG, beta human chorionic gonadotropin; SD, standard deviation.
The decrease in hemoglobin content between preoperative and postoperative values was significantly lower in the Endoloop group, compared to those of the electrosurgical group; the mean ± SD of decrease in hemoglobin content was 0.9 ± 0.7 g mL (range: 0.3–1.7 g/mL) in the Endoloop group, compared to mean ± SD 2.3 ± 0.8 g/mL (range: 0.4–3.9 g/mL) in the electrosurgery group. (p < 0.05).
Duration of hospitalization and β-hCG resolution duration in both groups were nonsignificantly different. None of the patients developed complications during the laparoscopic procedure, so, there were no conversations to laparotomy.
The postoperative outcomes are presented in Table 3. No patient developed persistent trophoblastic tissue. After following-up all cases for 18 months, no patient had any repeated ectopic pregnancy in the ipsilateral tube, but, unfortunately, 1 patient in group 1 had recurrent ectopic pregnancy the contralateral fallopian tube. Seventeen women (62.9%) in the Endoloop group and 16 women (59.2%) in the electrosurgery group achieved spontaneous pregnancies, which was nonsignificantly different between both groups.
Postoperative Outcomes of the 54 Tubal Pregnancy Cases treated with Laparoscopic Partial Distal Salpingectomy
Values are represented as number (%). All outcomes were nonsignificantly different in both studied groups.
Made with polydioxanone II a, violet monofilament; Ethicon, Somerville, NJ.
Discussion
Historically, ectopic pregnancy was a fatal condition wherein diagnosis was possible only at postmortem. Today, early diagnosis and management are associated with minimal maternal mortality and morbidity and better fertility outcomes. 20 The majority of ectopic pregnancies are located in the fallopian tube, ∼70% in the ampullary portion, 12% in the isthmic portion, and 11% in the fimbria. 2 Management of ectopic pregnancy can be expectant, medically with methotrexate, or surgically. 3 Until 1978, when laparoscopic salpingotomy was first reported by Bruhat and Pouly, 21 the choice of salpingotomy versus salpingectomy depended on many factors, including patient ages, tubes' condition, serum hCG levels, and patients' future fertility desires. Salpingectomy is preferable, as the success rate should be 100%, although there have been reports of persistent trophoblast tissue after salpingectomy, when the whole tubes had not been removed. 22 Moreover, salpingectomy was adopted for women with ruptured tubal pregnancies or women with uncontrolled tubal bleeding and severely damaged tubes. 23 The European Surgery in Ectopic Pregnancy (ESEP) trial, in 2014, failed to identify a difference in spontaneous conception between patients receiving salpingotomy versus salpingectomy (60.7% versus 56.2%; p = 0.678). 12 Salpingotomy did not result in a statistically significant higher incidence of recurrent ectopic pregnancy, compared with salpingectomy. 15
The fallopian tubes derive their blood supply from branches of the uterine and ovarian arteries. Salpingectomy may therefore potentially diminish collateral blood flow to the ovaries. 24 Coagulation of the blood supply in the mesosalpinx during salpingectomy could have an impact on collateral blood flow to the ovaries or damage ovarian tissue directly by lateral thermal spread. 25 Disturbing the blood supply during surgery could decrease ovarian perfusion and have a negative impact on steroid production and follicular development within the ovary. 26
Some studies have cited evidence regarding the potential detrimental effects of salpingectomy on ovarian reserve.18,27,28 However, other studies have indicated that it has no effect on ovarian reserve.29–31 A systematic review and meta-analysis by Boots et al., in 2015, recommended that more data were needed to stratify the analysis to determine if women of advanced age or with diminished ovarian reserves are at higher risk of negative effects from salpingectomy. 32 A systematic review and meta-analysis on ovarian reserve after salpingectomy in 2017 concluded that salpingectomy did not seem to compromise ovarian reserve in the short-term. However, the long-term effect of salpingectomy on ovarian reserve remains uncertain. 33
The Endoloop Ligature is a pretied suture with a plastic sheath that serves as an introducer. Hemostasis is achieved by looping the suture over the affected fallopian tube under direct vision and advancing the plastic sheath to tighten the pretied knot. The Endoloop is easy to use and achieves hemostasis quickly, with an excellent tourniquet effect and without risk of thermal injury. 34 Use of an Endoloop is associated with a shorter operating time, as well as lower postoperative pain scores and total analgesia requirements. 19 Faioli et al., stated that the Endoloop was a simple and effective technique for laparoscopic management of ectopic pregnancy, both in elective and emergency situations. 35
Conventional electrosurgery includes unipolar and bipolar diathermy. Bipolar cautery is safer than monopolar cautery as the former does not spread the burn to the surrounding structures. 36 The disadvantages of using conventional bipolar electrosurgery are that it cannot cut tissue and requires more time to coagulate the blood, causing more tissue charring and adherence of tissue that can lead to tearing of adjacent vessels, causing yet more bleeding. 37 The introduction of newer vessel-sealing systems—such as ultrasonic shears and feedback-monitored bipolar forceps—has revolutionized hemostasis techniques during laparoscopic procedures. Although associated with a lesser degree of thermal injury, compared to conventional bipolar energy, an ultrasonic harmonic device can seal vessels up to 4 mm in diameter. 38 Modern feedback-controlled energy sources—such as the Ligasure™ (Valleylab Inc., Boulder, CO) and the Plasma Kinetic Gyrus™ (PK) (Gyrus ACMI, Southborough, MA)—can seal vessels up to 7 mm in diameter. 38 However, these new instruments typically designed to be for single use and require the expenditure of capital for proprietary energy generators that increases per-case costs and thus are not easily available in countries of low socioeconomic status.36–38
Preference for energy-based modalities for tissue management in laparoscopic procedures depends upon each surgeon's own experience, as well as instrument availability and cost. 39 Thus, monopolar and conventional bipolar electrosurgery still are problematic in countries of low socioeconomic status, due to their wider range of tissue effects, dissection capabilities, cost-effectiveness, and lack of availability.38,39
Complete tubal resection (total salpingectomy) might reduce the risk of ipsilateral recurrent ectopic pregnancy but cannot prevent cornual pregnancy and might affect ovarian reserve by disturbing the blood supply. Partial salpingectomy is excision of the affected part of an ectopic pregnancy leaving the proximal and distal parts of fallopian tubes away from the ectopic swelling. In the current study, partial distal salpingectomy was performed, which included removal from fimbria till the end of the conceptus swelling at the end of the fallopian tube nearest to the uterine side; this was not partial salpingectomy. Partial distal salpingectomy was chosen because there is evidence for risks of pyosalpinx and hydrosalpinx. 40 In addition, tubal fimbria might also be a source of origin of serous intratubal carcinoma, and the site of development of the majority of serous ovarian and primary peritoneal cancers.40,41 For these reasons, leaving a remnant of the fallopian tube with the fimbrial ends during surgery should be avoided. 40 The Endoloop procedure was associated with significant less operative time and less intraoperative blood loss.
The Endoloop achieved good hemostasis in a quick one-step technique, compared to electrosurgery, which involved multiple repeated thermal energy maneuvers applied to the fallopian tube. No patient had repeated ectopic pregnancy in the ipsilateral tube using both procedures but, unfortunately, 1 patient, in the Endoloop procedure group, had a recurrent ectopic pregnancy in the contralateral fallopian tube. Seventeen women (62.9%) in the Endoloop group and 16 women (59.2%) in the electrosurgery group achieved spontaneous pregnancy, which was nonsignificantly different between both groups. Persistent trophoblastic tissue was not detected in any cases of the current study. It is not surprising that the Endoloop technique appears to be superior to electrosurgery in terms of simplicity, safety, blood supply, conservation of tubo-ovarian vessels, operating time, and operative blood loss.
Previous studies had reported that the rate of subsequent intrauterine pregnancy after salpingectomy ranged from 38% to 66%, whereas the rate of repeated ectopic pregnancy usually varied from 6% to 28%. However, no data are available for incidence of recurrent ipsilateral ectopic pregnancies.40,41 The exact incidence of ectopic pregnancy in the remnant stump following salpingectomy is not currently known. Between January 2000 and April 2012, of 816 women who presented with ectopic pregnancy to Whipps Cross University Hospital, in London, UK, 72 women had repeat ectopic pregnancies; 3 of these were ipsilateral, of which 1 was found in the distal remnant part of the fallopian tube. 42 Takeda et al. reported an incidence of 1.16% from January 1994 to August 2005. 43 Ko et al. reported 6 cases of recurrent ectopic pregnancy in the remnant portion of the tube after ipsilateral salpingectomy in women who had undergone assisted reproductive technologies. 44
Therefore, most of the previous studies40–45 could not prove that partial salpingectomy was associated with a significant incidence of recurrent ipsilateral ectopic or persistent trophoblastic tissue, compared with total salpingectomy. There are still debates about the effect of total salpingectomy on ovarian reserve.32,33 The tourniquet effect of Endoloop achieved good hemostasis without spreading thermal energy destructive effects in salpingectomy procedures as treatments for ectopic pregnancis.19,34,35
Conclusions
The current study showed that using the Endoloop Ligature tourniquet was a fast, effective hemostatic procedure without thermal use and that distal partial salpingectomy is minimally associated with recurrence of ectopic pregnancy or persistent trophoblastic tissue in the remaining portion of the ipsilateral fallopian tube. This finding encourages using distal partial salpingectomy with an Endoloop Ligature for treating fimbrial and ampullary ectopic pregnancy.
The long-term incidence of recurrent ipsilateral ectopic pregnancies following distal partial salpingectomy should be studied in future trials, and those results should be reproduced in order to make a recommendation in favor or not in favor of this approach to preserving ovarian blood supply.
Footnotes
Author Disclosure Statement
No financial conflicts of interest exist.
Funding Information
No funding was received for this article.