
Abstract
Background:
An anterior uteroperitoneal fistula, or isthmocele, is an increasingly recognized complication of a cesarean section. A posterior uteroperitoneal fistula developing after a cesarean section had not been described, prior to this current article.
Case:
A 26-year-old female presented 16 months after a cesarean section with amenorrhea and pelvic pain. She had a posterior cervicoperitoneal fistula, with a hematoma collection between the posterior cervix and peritoneum.
Results:
The patient's fistula was repaired laparoscopically, leading to complete resolution of her symptoms.
Conclusions:
A cervicoperitoneal fistula, or posterior uteroperitoneal fistula, is a potentially new type of complication after a cesarean section. Laparoscopic management is an ideal way to treat this complication with reduced morbidity.
Introduction
Increasing rates of cesarean sections worldwide has led to the development—and improved recognition of—new complications. 1 Anterior uteroperitoneal fistulas, also known as isthmoceles or cesarean scar niches, are being increasingly described since the last decade. 2 The advent of minimally invasive gynecology has allowed surgeons to diagnose and treat such complications endoscopically, leading to immediate resolution of symptoms with reduced surgical morbidity. This is the first article to describe a case of a posterior cervicoperitoneal fistula in a woman presenting with amenorrhea and pelvic pain 16 months after undergoing a lower-segment cesarean section. This case was managed laparoscopically, leading to complete resolution of the patient's symptoms.
Case
A 26-year-old para 1, live 1, female presented with complaints of secondary amenorrhea and lower-abdominal pain since 16 months, when she had undergone lower-segment cesarean section for non-progression of labor at a cervical dilatation of 3 cm. Her intraoperative records were not noteworthy, and she had a smooth postpartum recovery at that time. She had suffered a miscarriage 2 years prior, for which curettage was performed.
A pelvic ultrasound was suggestive of a fluid collection posterior to the uterus. Magnetic resonance imaging (MRI) revealed a discontinuity in the posterior aspect of the uterocervical junction, with a lobulated fluid collection in the endometrial cavity, and a lower-uterine segment that was continuous with a fluid collection posterior to the uterus, measuring 44 × 42 × 35 mm (Fig. 1). This suggested the possibility of a posterior uterine fistula; thus diagnostic hysteroscopy and laparoscopy were performed.

Magnetic resonance imaging depicting a discontinuity in the posterior aspect of the uterocervical junction, with a lobulated blood collection.
During the hysteroscopy, the cervix was pulled up, and bilateral ostia were seen. A posterior-wall rent with overlying fibrosis was noted. During the laparoscopy, it was noted that the uterine fundus was adhered with a thick band to the anterior abdominal wall. Her bilateral tubes and ovaries were normal. A 5 × 5–cm hematoma was present over the posterior aspect of the cervix (Fig. 2). The posterior peritoneum was opened over the cervix to drain copious chocolate-colored fluid, thus confirming the diagnosis of a cervicoperitoneal fistula (Fig. 3). A dilator was then placed in the uterine cavity, the margins of the fistula were freshened, and the edges were sutured in layers over the dilator with a V-Loctm 1-0 barbed suture (Medtronic, Dublin, Ireland). Thereby, the fistulous tract between the cervix and the pouch of Douglas was repaired in two layers (Fig. 4). Next, a Foley's catheter was inserted into the uterine cavity, to maintain uterocervical continuity, and was secured to the ectocervix with a polygalactin 910 (Vicryl,® Ethicon Inc., Sommerville, NJ, USA) suture.
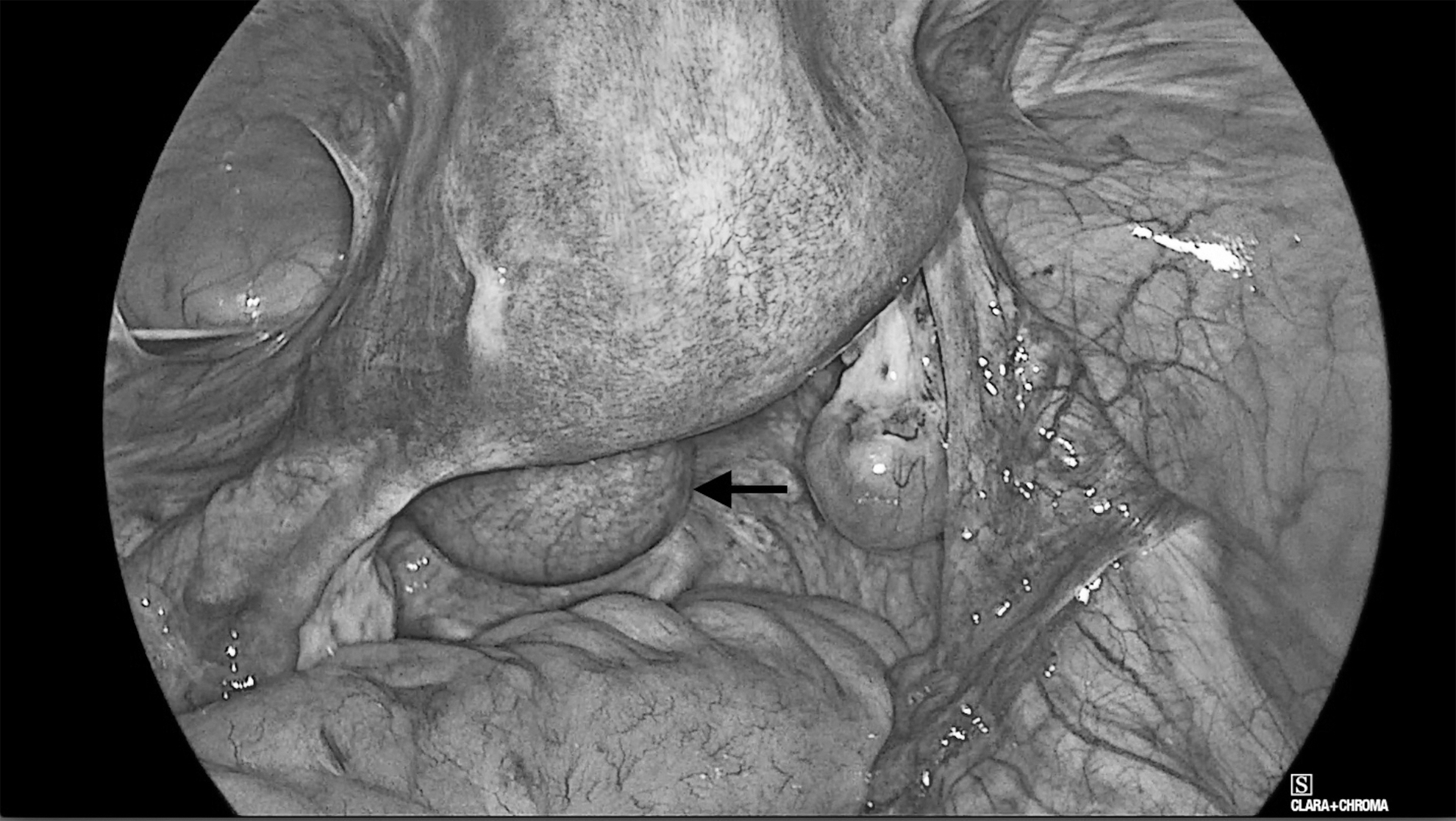
Laparoscopic view showing the adhesion bands between the anterior uterus and abdominal wall, and a 5 × 5–cm hematoma posteriorly at the cervical level (dark arrow).
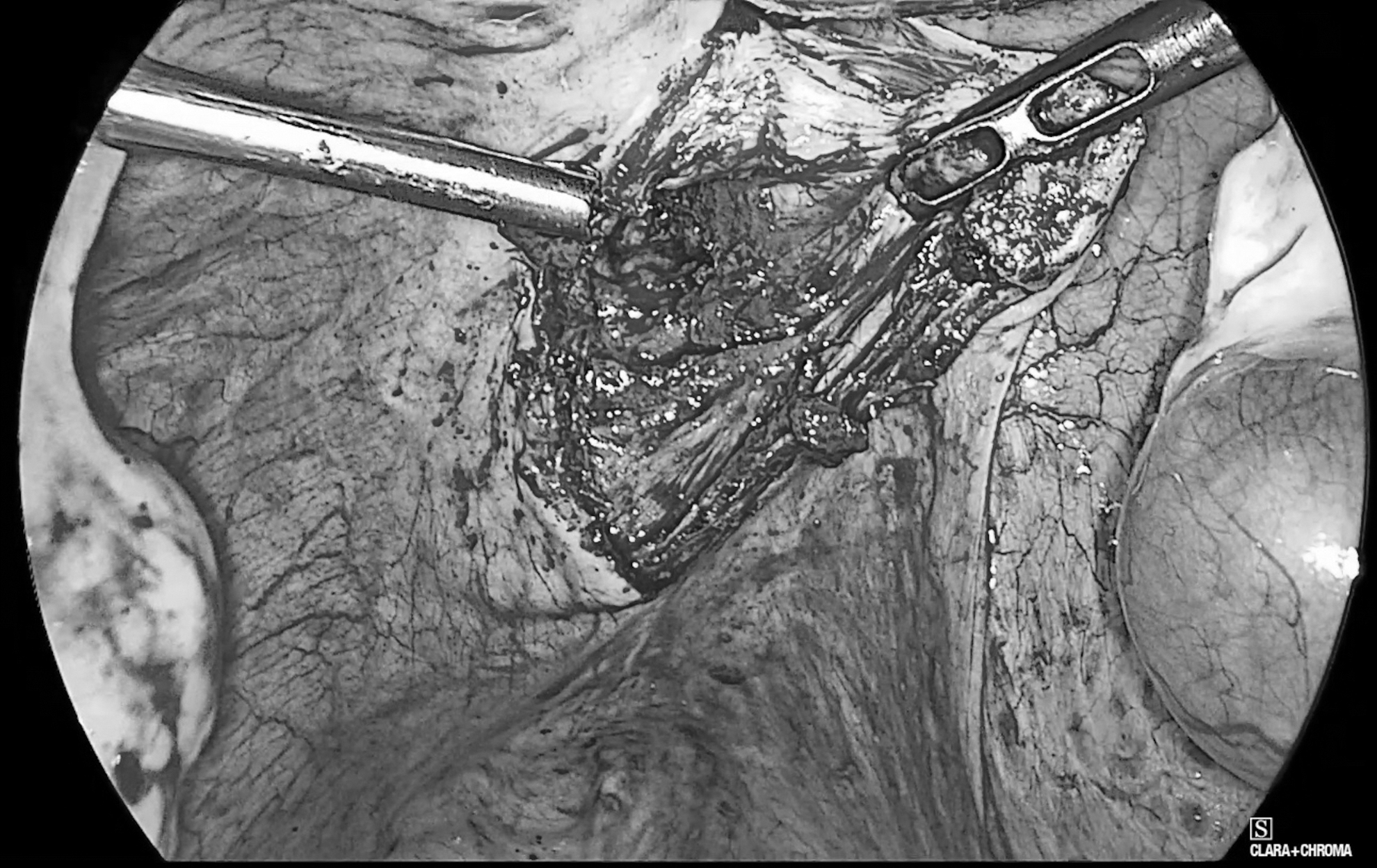
The posterior cervicoperitoneal fistula, containing old collected blood, being drained.

Repair of the cervicoperitoneal defect performed in two layers with a V-Loctm 1-0 barbed suture (Medtronic, Dublin, Ireland).
Results
The patient had resumption of her menstrual period 4 weeks after the surgery with the Foley's catheter in situ. The catheter was removed 2 weeks after her first period. She has been under follow-up for 3 months, as of this writing, and has had monthly menstrual bleeding.
Histopathologic evaluation of the fistula tract was consistent with endometriosis.
The patient consented to have this case report published.
Discussion
A uteroperitoneal fistula—a connection between the uterus and peritoneal cavity—is extremely rare, in comparison to an obstetric fistula, which develops between the genital and urinary tracts, the latter of which 50,000–100,000 cases are estimated to occur every year. 3 Uteroperitoneal fistulas have been described to occur after cesarean sections, 4 myomectomies, 5 salpingectomies, 6 and abortions.7,8 Tuboperitoneal fistulas are among the mechanisms of failure of tubal ligation. 9 The other possible causes and contributory factors might include inadequate healing after a cesarean section, especially after prolonged labor, and exacerbated by smoking or diabetes, forceps delivery, gynecologic injuries such as perforation during endoscopy, tuberculosis of the genital tract, and perforation with intrauterine contraceptive devices. This case represents, to the best of the current authors' knowledge, the first described posterior cervicoperitoneal fistula leading to amenorrhea and pelvic pain, a case that was managed endoscopically.
Anterior uteroperitoneal fistulas are frequently described as cesarean-scar niches or isthmoceles, and are increasingly recognized as complications of cesarean sections.1,2,7 Anterior uteroperitoneal fistulas are explained by virtue of their closeness to cesarean scars, but a plausible cause in the current case could not be pinpointed. A case of a spontaneous posterior uterine perforation leading to a uteroperitoneal fistula after myomectomy was described by Koyama et al., 5 and the presentation and surgical findings of that case resonate closely with the current case. Those authors hypothesized that the triggering insult for uterine perforation was poor blood supply, because the site of the perforation was not the same as the incision made during that patient's myomectomy. This was worsened due to the patient's retrograde menstruation, leading to the development of polypoid endometriosis posterior to the uterine cavity.
While poor blood supply and healing could explain the current case, the current authors also hypothesize that overzealous uterine or vaginal toileting during her cesarean section might have led to a focal weakening at the site of the fistula. Although the patient denied that any subsequent pregnancy occurred after her cesarean, another possibility is that the anatomical distortion created by the anterior adhesions might have predisposed her to sustain a posterior cervical injury during curettage or suction. The fistula could have also been caused by the curettage done before the patient's pregnancy, but the possibility of such a defect being asymptomatic during her pregnancy is questionable. The rarity of this case precludes the current authors from making more-definitive conclusions about the fistula's etiology, but it is likely that an overlooked iatrogenic insult precipitated the fistula's development.
Any case of prolonged amenorrhea after a cesarean section—especially when accompanied by spotting, pelvic pain, or infertility—should prompt a search for local causes. The latter could include adhesions or fistulas. Sonography is a good screening test, and hysterosalpingography or MRI can be useful for confirmation. Following the general principle of fistula surgery, the optimal management is excision of the fistulous tract and reinforcement of the uterine wall. Not only does this treat the patient's symptoms immediately, but this also prevents the risk of a cervical pregnancy and uterine rupture in subsequent pregnancies.
Conclusions
The ever-increasing rate of cesarean sections and ready availability of laparoscopic services in various parts of the world will lead to an increase in complications, such as the one described in this article. This calls for a closer scrutiny of cesarean surgical techniques in order to reduce long-term complications.
Footnotes
Author Disclosure Statement
No financial conflicts of interest exist.
Funding Information
No funding was provided in connection with this case report.