
Abstract
Objective:
This article describes the average number of narcotics used after common ambulatory gynecologic surgeries and describes provider prescribing patterns.
Materials and Methods:
This was a prospective observational cross-sectional study in patients undergoing benign gynecologic surgery. Patients were identified via the gynecologic surgery schedule from a Midwestern urban academic hospital and enrolled from 8/2018 to 7/2019. Each patient was recruited preoperatively, signed consent, and completed a baseline pain and demographic survey. Inclusion criteria were patients ages 18–99; English-speaking; and undergoing benign gynecologic ambulatory surgery, such as benign laparoscopic adnexal surgery, midurethral sling placement, and/or anterior or posterior repair. Patients were excluded if they had past or current cancer diagnoses, chronically used narcotics, had chronic pain currently being treated by physicians, had surgeries converted into laparotomies, or were admitted to the hospital postoperatively for pain control. After enrollment, patients completed diaries to record narcotic use and postoperative pain for 7 days postoperatively. These patients were then contacted to provide information regarding amounts of narcotic medications used as well as additional medications used for pain. Descriptive statistics, Spearman-rank correlations, and Kruskal–Wallis tests were used.
Results:
Ninety subjects were enrolled and 75 completed follow-ups. Subjects on average were prescribed 14.3 tablets of narcotics (most often 5/325 of NORCO,® 50 mg of tramadol, or 300/30 mg of Tylenol® #3) correlating to 70.6 morphine mg equivalents (MMEs). Subjects on average used 3.9 tablets correlating to 19.5 MMEs, with 75% of patients using 6 tablets or less within 7 days after surgery. After ambulatory benign gynecologic surgery, patients had an average excess of 10.4 unused prescribed narcotic tablets (or 71% of prescribed pills). Age, patient history of depression, baseline pain medication use, and number of narcotics prescribed were associated with increased postoperative narcotic use.
Conclusions:
Gynecologic surgeons prescribe narcotics in excess of patients' needs.
Introduction
Over the past 25 years, the United States has seen an increase in the proportion of gynecologic procedures performed via minimally invasive techniques and in the ambulatory setting. 1 These patients often require a shorter recovery time and have fewer postoperative narcotic requirements. 1 Multiple guidelines for the management of postoperative pain have been published by agencies such as the American Pain Society, the American Society of Anesthesiologists, the Institute for Clinical Symptoms Improvement, and the Agency for Healthcare Research and Quality. A common acknowledgment in these guidelines is the recognition that there is a paucity of high-quality research for postoperative pain management. 2 In response, recent studies have described postoperative narcotic use after major gynecologic surgeries such as hysterectomy3–8 ; however, data on narcotic use after minor gynecologic surgeries are limited.
In the ambulatory gynecologic setting, the amounts of narcotics patients require postoperatively has not been studied thoroughly in the acute postoperative period (7–14 days). As the numbers and proportions of benign ambulatory gynecologic surgeries increase, it is essential to provide adequate pain control postoperatively while preventing opioid overprescribing. Opioid prescriptions in the United States have increased substantially over the past 2 decades.9,10 With this increase, the United States has also experienced an increase in overdoses from narcotics and narcotic addiction.9,10 The medical community is uniquely positioned to balance the unintended consequences of opioid misuse and abuse with the need to provide adequate pain control. 11
The primary objective of this research was to determine and describe the amounts of narcotics patients used in 7 days postoperatively after common ambulatory gynecologic surgeries. Secondary objectives included identifying risk factors for increased narcotic use postoperatively and describing provider prescribing patterns for narcotics after ambulatory gynecology procedures. The hypothesis was that patients use fewer narcotics postoperatively from ambulatory gynecologic surgery than gynecologists prescribe.
Materials and Methods
This was an observational cross-sectional study investigating narcotic use after benign ambulatory gynecologic surgery. Patients were recruited over the course of the 12-month timeperiod August, 2018 to July 2019. Patients included in the study were ages 18–99, English-speaking, and undergoing benign gynecologic ambulatory surgery (such as midurethral sling placement, anterior or posterior repair with or without vault suspension, laparoscopic salpingo-oophorectomy, laparoscopic salpingectomy, laparoscopic ovarian cystectomy, and/or laparoscopic tubal ligation). These specific surgeries were chosen because they are most often ambulatory with few patients admitted to the hospital postoperatively. At the University of Chicago Medical Center, in Chicago, IL, patients who undergo longer or more-complex surgeries are often admitted overnight for observation and might receive additional intravenous narcotics for pain control.
Patients were excluded if they had past or current pelvic cancer diagnoses, chronically used narcotics (self-described use of narcotic medications on most days for at least 3 months prior to their surgeries), had histories of chronic pain currently being treated with narcotic pain medications, were non-English primary speakers, and if their surgeries were converted into laparotomies, or if these patients were admitted to the hospital postoperatively. At the University of Chicago Medical Center, during the 12 months of data collection, the gynecology department performed ∼1915 gynecologic surgeries, 1135 of which were ambulatory gynecologic surgeries, including minor laparoscopic cases, dilation and curettage (D&C), hysteroscopic cases, midurethral sling placements, etc. As patients undergoing D&C and/or hysteroscopy are not prescribed narcotics routinely upon discharge from the hospital, these cases were not included in the data collection.
During this time, surgeons at the University of Chicago Medical Center operated on 780 “major cases,” including open and laparoscopic hysterectomy and myomectomy cases, in which the patients are routinely admitted for observation following surgery at this institution, and, therefore, were not included in this study.
Patients were approached in the preoperative area prior to surgery and asked if they would like to participate in the study. Participation was voluntary and did not change their care. Patients were identified weekly by a gynecologic surgery report generated by the electronic medical record system. Patients were approached consecutively; however, not every patient identified as a candidate was approached due to resident work-flow and logistical barriers. After informed consents were obtained, subjects were surveyed on their baseline pain, using a 11-point Likert scale (0–10), and their baseline pain medication usage, and demographic information was collected. After enrollment, each patient was provided with a pain diary to track daily pain scores using the same 11-point Likert scale and the number of narcotics used each day for 7 days after surgery as well as supplemental ibuprofen or acetaminophen usage during this postoperative timeperiod.
Baseline demographic information on each participant was obtained from the electronic medical record through chart review, including age, prior medical and surgical history, history of chronic pain, substance abuse, and psychiatric illness. The number of narcotics and type of narcotics prescribed postoperatively were obtained from the electronic medical record. At the University of Chicago Medical Center, the vast majority of providers prescribe NORCO® (5 mg of hydrocodone/325mg of acetaminophen) for pain control after surgery. Tramadol (50 mg) and Tylenol® #3 (300 mg of acetaminophen/30 mg of codeine) are also prescribed intermittently, and 1 patient was prescribed Percocet® (5 mg of oxycodone/325 mg of acetaminophen).
As this was an observational study, no guidance or instructions were provided to prescribers regarding type or number of narcotics to be issued postoperatively. The goal was to determine and describe ongoing prescribing patterns. Providers were aware that their patients were enrolled into the study but were not involved in the patients' follow-up. No institutional- or state-level efforts were concurrently implemented during the time of this study, and no standardized or consistent narcotic or Enhanced Recovery After Surgery® (ERAS®) protocols were initiated or utilized during this data-collection period.
When contacted on postoperative day 3 and postoperative day 7 by 1 of the coauthors or study staff, patients were asked about their pain scores each day for 7 days after surgery, the number of narcotics used as recorded in their provided diaries, and any additional acetaminophen or ibuprofen used postoperatively. This information, as well as the demographic information collected, was entered electronically—in a password-protected REDCap [Research Electronic Capture] database—and was later extrapolated and analyzed.
Primary outcomes included determining and describing the average number of narcotics used for patients postoperatively after ambulatory gynecologic surgeries. Secondary analysis evaluated associations between demographic and postoperative factors with an increased narcotic requirement postoperatively. It was determined also that, with 75 patients, there would be an 80% power to detect a correlation of 0.32 (2-sided α = 0.05). Analyses were performed using Stata 15 (StataCorp. LLC, College Station, TX). Data were summarized, using frequency counts and percentages for categorical data and mean, standard deviation (SD), or median and interquartile range (25%–75%) for continuous data. Spearman-rank correlation coefficients were calculated to assess the relationship between number of narcotics used and pain or age. Wilcoxon rank-sum tests or Kruskal–Wallis tests were used to compare the average number of narcotics used per day, total number of pills prescribed or used, and excess number of pills prescribed across the groups.
Results
One hundred and sixty-one patients were eligible for participation, 105 patients were approached, and 90 patients consented to be included in this study (Fig. 1). Seventy-five patients completed the study requirements. Two patients were admitted to the hospital and were, therefore, excluded, 8 patients were lost to follow-up, 1 patient withdrew from the study, 1 patient was excluded as her case was converted to laparotomy, 1 patient was excluded as she underwent laparoscopic myomectomy and was admitted to the hospital postoperatively, 1 patient gave her consent but her surgery was cancelled, and 1 patient also gave her consent but was excluded as she did not speak English (Fig. 1). Of the 8 patients lost to follow-up, 2 underwent midurethral sling placement, 3 underwent laparoscopic salpingectomy, 2 underwent laparoscopic salpingo-oophorectomy, and 1 underwent laparoscopic cystectomy.
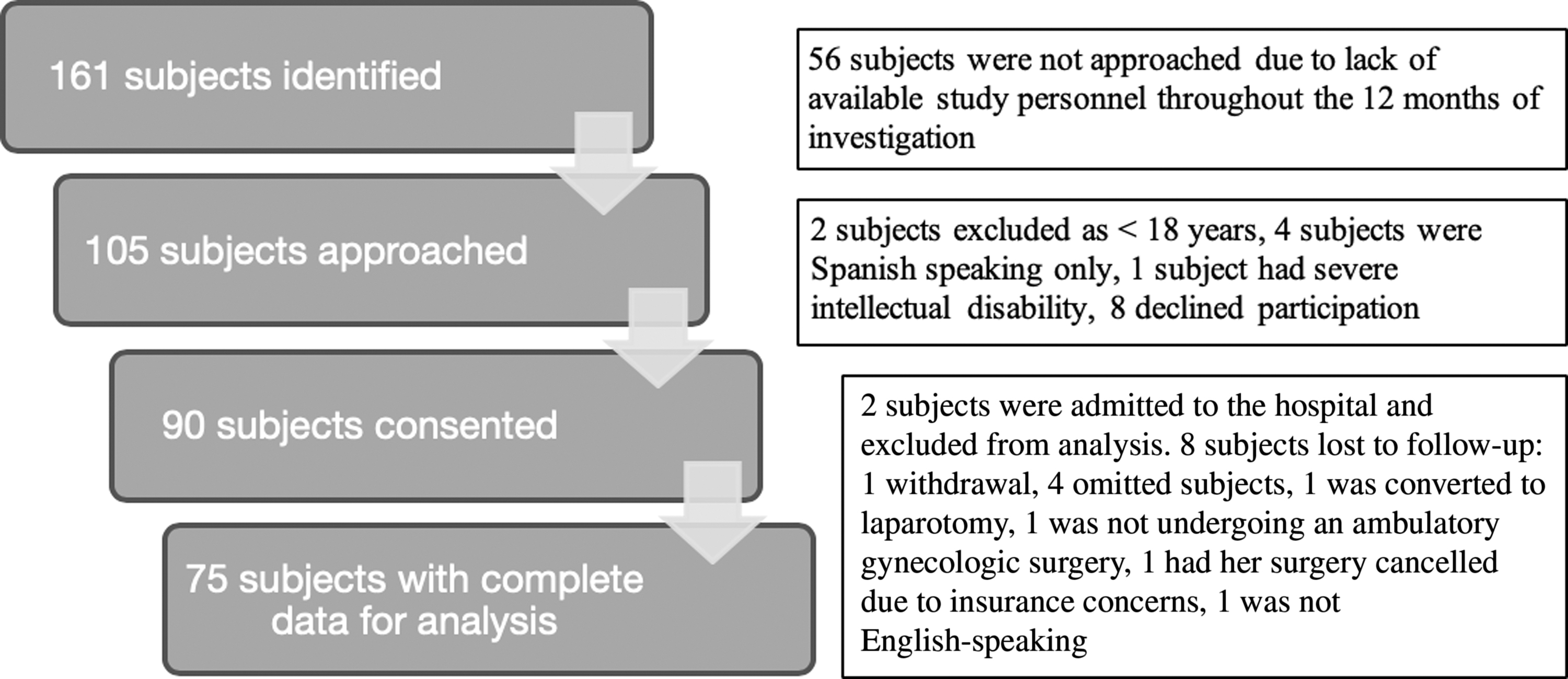
Study enrollment diagram.
Subjects were an average of 40 years of age (range: 20–77 years); the demographic information and baseline information are shown in Table 1. Patients were surveyed on baseline pain scores and 48 subjects had an average pain score at baseline of 1.1 (SD of 1.9). Their pain was primarily described as pelvic pain (11 subjects; 22.9% of subjects reporting baseline pain) and musculoskeletal pain (back and joint pain; 13 subjects; 27.1% of subjects reporting baseline pain). Sixteen subjects (21.3%) used daily nonnarcotic pain medications at home (Table 1). Forty-one percent of patients had used narcotics in the past, with 71% of these instances after prior surgery and 12.9% due to pain conditions, most frequently back pain, not currently being treated.
Demographic Data, Baseline Pain Scores, Medication Use, and Type of Surgery
Yrs, years; SD, standard deviation; n, number of subjects.
Subjects on average were prescribed 14.3 tablets of narcotics: 70 patients were prescribed hydrocodone–acetaminophen (NORCO) 5/325-mg tablets; 2 patients were prescribed tramadol 50-mg tablets; 2 patients were prescribed Tylenol #3 300/30; and 1 patient was prescribed Percocet 5/325, correlating to 70.6 morphine mg equivalents (MMEs). The number of narcotics prescribed ranged from 0 to 30 tablets correlating to 0–150 MMEs.
Narcotic medications were prescribed by attending physicians, as well as by residents and physician-assistants under the recommendations of the attending physicians in the gynecology department without instruction or guidance as to the types of narcotics or amounts prescribed with regard to this study. The average pain scores on postoperative days 1 and 2 were 6.0 and 4.9, respectively resulting in an average of 1.2 tablets of narcotics or 6.2 MMEs used in the first 48 hours postoperatively (SD: 6.4; 25%–75% of prescribed pills; 0–10 MMEs). In the first 7 days after surgery, subjects on average used 3.9 narcotic tablets, which correlated to 19.5 MMEs. Seventy-five percent of patients used 6 tablets or fewer (30 MMEs) in 7 days after surgery. This established an average excess of 10.4 narcotic tablets correlating to 51.1 MMEs prescribed (or 71% of prescribed pills on average; Table 2).
MMEs Prescribed and Used by Surgery Type and Overall
MMEs, morphine mg equivalents; IQR, interquartile range; BSO, bilateral salpingo-oophorectomy; SD, standard deviation; n, number of subjects.
For each type of surgery, number of narcotics prescribed and used were evaluated (Table 2). Patients who underwent laparoscopic salpingectomy were prescribed on average the greatest number of narcotics at 16 tablets (80 MMEs), whereas patients who underwent midurethral sling placement, with or without anterior or posterior repair, were prescribed the least number of narcotics with an average of 11.9 tablets correlating to 58.8 MMEs (Table 2). However, there was no statistically significant difference in the number of narcotics prescribed by surgery type (p = 0.35). Based on a Kruskal–Wallis test, there was a statistically significant difference identified among the groups for total narcotic amounts used after surgery (p = 0.035; Table 2). Patients on average used the highest numbers of narcotics (5.9 tablets, 29.7 MMEs) after laparoscopic ovarian cystectomy and the least after midurethral sling placement (1.3 tablets, 6.7 MMEs; Table 2). There was a statistically significant correlation between narcotic use and the number of prescribed narcotics (r = 0.29; p = 0.012) with increasing numbers of narcotics prescribed trending toward increased postoperative narcotic use.
Figure 2 shows visual analogue scale (VAS) scores for pain in subjects over the 7 days after surgery. Figure 3 shows the decline in narcotic use over time after surgery with the greatest decline between postoperative day 2 and day 3. Seventy-five percent of patients used 1 narcotic tablet or fewer by postoperative day 3, and 75% of patients stopped using narcotics after postoperative day 4 (Fig. 3). Seventy-five percent of patients used 6 narcotics or fewer (30 MMEs or fewer) postoperatively (Fig. 3). Figure 3 shows the decline in narcotic use after surgery over time with the greatest decline between postoperative day 2 and day 3 after surgery.
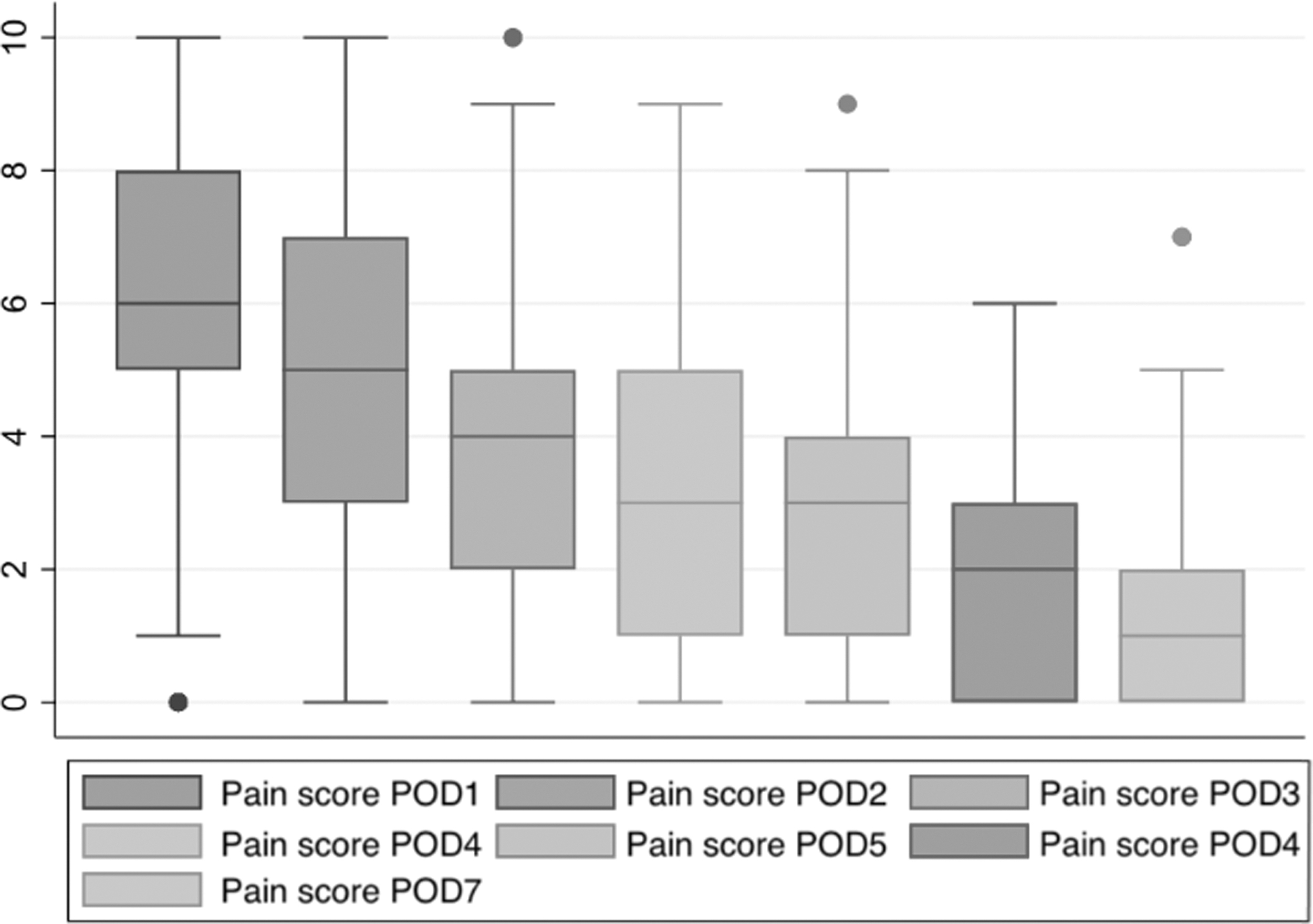
Postoperative pain by postoperative day (POD). Dots represent outliers.
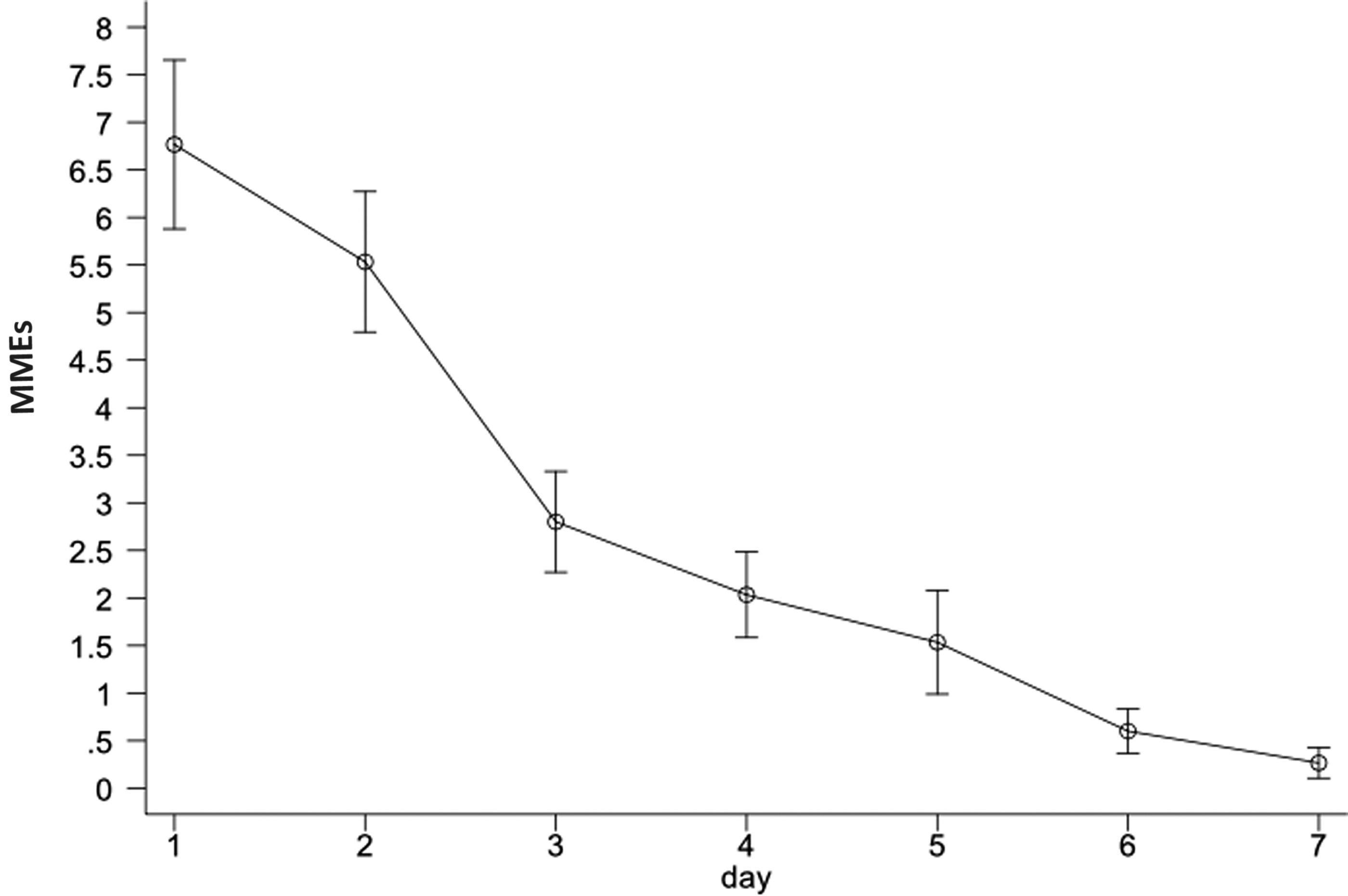
Morphine mg equivalents (MMEs) used each day after surgery, plot of the mean ± standard error.
There was a statistically significant association between total postoperative narcotic use and history of depression (p = 0.031). There was also a statistically significant association between postoperative narcotic use and home nonnarcotic pain medication use prior to surgery (p = 0.008), most often reported to be nonsteroidal anti-inflammatory drugs (63% of participants; Table 3). A correlation was identified between age at time of surgery and between narcotic use, with younger patients having increased average narcotic use over 7 days (r = −0.36; p = 0.002). A statistically significant association also emerged between baseline pain score before the surgery and postoperative narcotic usage (r = 0.24; p = 0.036).
Predictors of Increased Postoperative Narcotic Use
MMEs, morphine mg equivalents; SD, standard deviation.
Discussion
On average, gynecologic surgeons in this study prescribed 51.1 MMEs or 10.4 narcotic tablets in excess of patients' needs. There were associations among previous diagnosis of depression, increased baseline pain scores, and younger age with total narcotic use. These associations have been shown previously in the literature.3,4 Previously published studies have also suggested that higher preoperative pain scores might be related to persistent pelvic pain 6 months after hysterectomy, 12 which might be indicative of future chronic narcotic use and dependence. This could provide an opportunity to intervene with counseling if patients were screened and identified preoperatively.
Recent studies have been published regarding opioid use after minimally invasive surgery3–8 ; however, there are limited data on pain management after ambulatory gynecologic surgery. Regarding ambulatory gynecologic laparoscopy, a study published in January 2019 found that patients after minor laparoscopy procedures were prescribed 150 MMEs and used ∼45 MMEs, an excess of ∼105 MMEs. 13 In that study, Patanwala, et al. concluded that gynecologic surgeons prescribed nearly 3 times more opioid tablets than were used by patients after gynecologic surgery, 13 which has also been discussed throughout the minimally invasive urogynecology literature. Swenson, et al. showed that, in urogynecology, patients completed recovery with two-thirds of narcotics prescribed left unused at home. 14
These data are consistent with the current study's findings that patients were prescribed in excess of their needs. Patanwala et al. 13 had published similar results; however, they did not differentiate among minor surgeries performed or describe the criteria for “minor” and “major” laparoscopic surgeries. 13 The current study analyzed data further into surgical types, with patients using more narcotics after laparoscopic ovarian cystectomy (an average of 6 narcotic tablets used correlating with 29.7 MMEs, with 75% of patients using 6 or fewer tablets after surgery) and using fewer narcotics after midurethral sling placement (average of 1.3 narcotic tablets correlating with 6.7 MMEs with 75% of patients using fewer than 3 tablets). Although laparoscopic hysterectomies and laparoscopic myomectomies are increasingly becoming ambulatory procedures at the current institution, all patients undergoing hysterectomies are admitted for observation. Thus, these patients were not included in this analysis. Hysteroscopy, another common ambulatory gynecologic surgery, was not included as the protocol of the University of Chicago Medical Center is to discharge these patients without any narcotic pain medications.
This current study showed a statistically significant correlation between narcotic prescriptions and increased narcotic use. Patients who are prescribed more narcotic pain medications after surgery tend to use more narcotics postoperatively. This study showed that patients are prescribed on average 51.1 MMEs in excess of what is being used after benign ambulatory gynecologic surgeries. Previous articles have reported 16,000 deaths from opioid misuse in the United States in 2015, tripling the rate since 2000.9,11 Natural and semisynthetic opioid pain relievers (i.e., morphine, codeine, oxycodone, hydrocodone, and oxymorphone) continue to be involved in the majority of these fatalities. 9 Data from this current study comprised additional evidence that the numbers of narcotics prescribed postoperatively after ambulatory gynecologic surgeries might influence narcotic use. Prior studies have shown that the proportion of patients who become long-term opioid users increases with increased amounts of opioids dispensed in the initiation month. 10
By limiting the number of narcotics prescribed postoperatively, surgeons might be able to reduce the number of patients who transition toward becoming long-term opioid users and limit the societal burden of opioid misuse. Reports have previously cited patient satisfaction as a concern trending toward higher postoperative narcotic prescriptions at discharge. 7 As-sanie et al. found no association between the initial postoperative prescription dose and patient satisfaction or postoperative pain measures. 7 Thus, gynecologic surgeons often prescribe in excess of patients' needs and should consider 10 or fewer narcotic tablets (50 MMEs) after ambulatory gynecologic surgeries.
Strengths of the current study included its prospective nature, use of a standardized VAS to reduce the effect of the inherently subjective nature of reports of pain, and daily diaries to reduce recall bias. This 11-point VAS was used to create a uniform description of each pain score level to be compared across patients. Having patients recall pain scores each day for a week after surgery—recording pain scores each day—helped reduce recall bias that might have occurred. This study allowed for evaluation of trends for narcotic use as patients were actively recovering from surgeries. The current study also assessed postoperative pain based on an 11-point Likert scale each day for 7 days after surgery, allowing postoperative pain to be assessed and trended in conjunction with narcotic use. The study provided a baseline for postoperative pain after ambulatory gynecologic surgeries as well as a reference for surgeons for narcotic prescribing postoperatively after specific ambulatory gynecologic surgeries, analyzed by surgery type.
Limitations of the current study included a limited sample size, and the subjective nature of pain assessment and self-reporting of narcotic use. The primary source of data collection was obtained by calling patients 7 days after surgery. Eight patients (∼ 10% of those who consented be in the study) were lost to follow-up. Patients were contacted 3 times after surgery and after 2 weeks without follow-ups; then patients were no longer contacted. These 8 subjects underwent varying surgeries (2 underwent midurethral sling placement, 3 underwent laparoscopic salpingectomy, 2 underwent laparoscopic salpingo-oophorectomy, and 1 underwent laparoscopic cystectomy). This might have affected the study's results. As the pain diaries were not collected, this study relied on patient reporting of pain scores and narcotic use in the postoperative timeperiod. Reporting bias from self-reporting of narcotic use could have played a role in the setting of media coverage regarding narcotic use and overuse and might have affected the results. Further studies with larger sample sizes at multiple institutions can increase the generalizability of these data.
Conclusions
Future directions will include how patients dispose of these excess narcotics to ensure that excess pain medications are disposed of in a safe manner. With increasing use of ERAS protocols, patients will tend to use fewer narcotics after surgery, which will result in an increased excess of narcotics left unused at home.15,16 As gynecologic surgeons prescribe fewer narcotics to limit the excess opioids prescribed, investigation of patient satisfaction with pain control postoperatively as well as availability of refills can ensure adequate postoperative pain control.
Footnotes
Author Disclosure Statement
No conflicts of interest exist.
Funding Information
No external funding was provided for this study.