
Abstract
Background:
Extrapelvic endometriosis is rare, with vulvar endometriosis being rarer. Spontaneous manifestation is extremely uncommon.
Case:
We report a case of spontaneous vulvar endometriosis of the labium minus in a woman with history of previous cesarean delivery and an incision and drainage procedure for Bartholin's abscess, and discuss the challenges in diagnosis and management.
Results:
A 24-year-old primipara presented with cyclical pain and swelling in the vulva for 6 months. On examination, a firm 3 × 3 cm tender mass was palpated in the right periclitoral region. Wide local excision was performed. Histopathology confirmed vulvar endometriosis.
Conclusion:
Vulvar endometriosis presents both diagnostic and management challenges and should be managed with surgery, close surveillance, and follow-up.
Introduction
Extrapelvic endometriosis is rare, with vulvar endometriosis being rarer. Risk factors include previous episiotomy scar. Spontaneous manifestation is extremely uncommon. We report a case of spontaneous vulvar endometriosis in a woman with history of previous cesarean delivery and an incision and drainage procedure for Bartholin's abscess. The challenges in diagnosis and management of such cases are discussed.
Case
A 24-year-old primipara with previous cesarean delivery presented to our institute with complaints of cyclical pain and swelling in the vulva for the past 6 months. The swelling was visible only during her menstruation in the upper part of right labium minus and was associated with extreme pain and altered blood-stained discharge (Fig. 1A; self-clicked image by patient). She reported that the swelling subsided after cessation of menstruation. Her last menstrual period was 2 weeks back. The previous cycles before 6 months were regular, of average flow and without any dysmenorrhea. She was para one with one living issue, having undergone a cesarean delivery 5 years back. There was no history of any contraceptive use.

Clinical images.
Her past history was significant for having undergone an incision and drainage procedure 4 years back for Bartholin's abscess of right labium majus. General and systemic examinations were unremarkable. Per abdominal examination revealed a healthy Pfannensteil scar. On local examination, there was no obvious swelling. A firm 3 × 3 cm tender mass could be palpated in the right periclitoral region, below the upper labia minora. Bimanual examination revealed a normal size, anteverted, firm and mobile uterus with fornices being free. Transabdominal ultrasonography revealed no evidence of adenomyosis or endometrioma. Patient refused transvaginal sonography and transperineal ultrasonography due to pain. Fine needle aspiration cytology was advised, but failed due to technical reasons. A provisional diagnosis of vulvar endometriosis of right labium minus was made and she was planned for wide local excision under spinal anesthesia.
Results
A curvilinear incision was given over the lesion taking care to preserve the clitoris. Tarry-colored fluid drained on dissection (Fig. 1B). A 3 × 3 cm fibrosed mass with cystic areas and bluish content was excised. Histopathology revealed ectopic endometrial glands (Fig. 2A), consistent with vulvar endometriosis with adequate fatty tissue (Fig. 2B), indicative of a wide local excision. At follow-up after her next periods, patient was asymptomatic with no evidence of vulvar endometriosis (Fig. 2C). Currently, she has completed 1 year of follow-up and is asymptomatic.
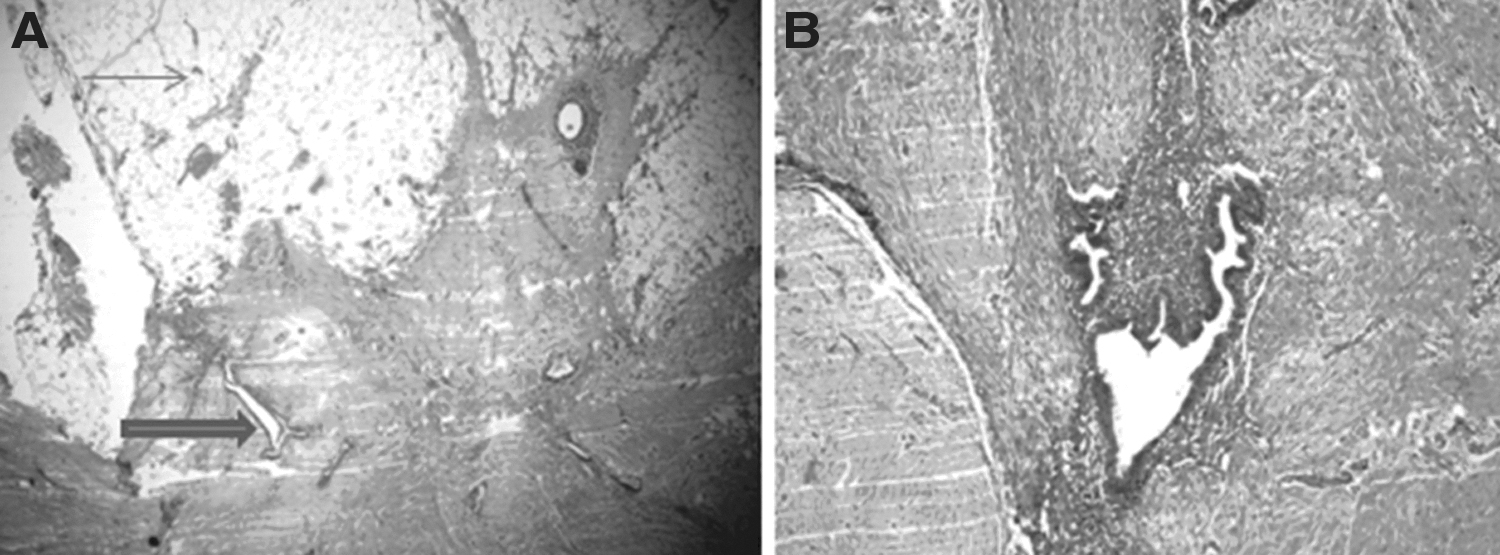
Histopathological images.
Discussion
Endometriosis is the occurrence of endometrial glands and stroma outside the endometrium. It affects 6%–10% women in the reproductive age group. The common theories concerning the pathogenesis of endometriosis include ectopic transplantation of endometrial tissue, coelomic metaplasia, and vascular dissemination.
Extrapelvic vulvar endometriosis is considered rare although the true incidence is unknown in the absence of epidemiological studies. The reported sites of vulvar endometriosis are episiotomy scars, Bartholin's gland and rarely, labia majora, labia minora, and hymen. 1 Our case had vulvar endometriosis of the right labium minus.
Differential diagnoses include Bartholin cysts, ulcers, and vulvar carcinomas. A clue to diagnosis of vulvar endometriosis may be the cyclic pattern of presentation related to menstruation, which was present in our case also. Vulvar endometriosis usually occurs after surgery or trauma and rarely spontaneously. 2 A case of a young girl developing vulvar endometriosis with a history of previous vulvar ulcers has been reported. 2 In another instance, a case of spontaneous periclitoral endometriosis has been reported in a 29-year-old woman that required two surgeries. 3 Spontaneous vulvar endometriosis is explained by the perviousness of the canal of Nuck, holding true Sampson's theory of retrograde menstruation. The development of vulvar endometriosis may also be due to a local inflammation leading to modulation and growth of ectopic endometrial tissue. 2 Our case had previous cesarean delivery and no episiotomy had been performed. A possible reason in our case might have been the incision and drainage procedure done 4 years back for Bartholin's abscess, which might have caused the surgical implantation of endometriosis.
The challenges in surgery include complete excision of the lesion while preserving sexual function. 3 The unusual location of the lesion in the upper part of labium minus near the clitoris was challenging. However, unlike the report by Gririmstad and Carey, 3 where they could excise only as much of the lesion possible since it was densely adherent to the clitoris, in our case the lesion was periclitoral with a small margin in between.
Although vulvar endometriosis is benign, the rare possibility of its malignant transformation to clear cell adenocarcinoma should be borne in mind. In a report from Korea, it was found that clear cell adenocarcinoma had developed from vulvar endometriosis that had been excised 3 years back. 4 Hence, there is a need to follow-up these women with vulvar endometriosis. It should also be differentiated from adenoid cystic carcinoma of the Bartholin's gland, especially if age of the patient is >40 years and lesion is near Bartholin's gland.
Conclusion
To conclude, vulvar endometriosis presents both diagnostic and management challenges and should be managed with surgery, close surveillance, and follow-up.
Footnotes
Authors' Contributions
S.S. and M.N. were involved in the management of the case. S.S. wrote the initial draft of the article. S.S. and M.N. helped in data collection and preparation of final article to be submitted.
Acknowledgment
The authors thank the department of Pathology for providing the histopathology images.
Disclaimer
The article has been read and approved by all the authors, the requirements for authorship as stated earlier have been met, and each author believes that the article represents honest work.
Ethics
Written informed consent was obtained from the patient.
Author Disclosure Statement
The authors declare no conflict of interest.
Funding Information
No funding was received for this article.