
Abstract
Introduction:
To facilitate vaginal cuff closure, several endomechanical suturing devices can be used. This retrospective study was undertaken to compare two different devices to determine if there was an advantage to either device.
Methods:
Laparoscopic hysterectomies performed where vaginal cuff closure times could be measured on recorded video were reviewed. Demographic information was obtained on these cases and the two suturing devices were compared.
Results:
Cuff closure times with the EndoStitch® (Covidien, Norwalk, CT) and the RD-180® (LSI Solutions, Rochester, NY) devices were evaluated for overall cuff closure time, per stitch time, and assessed for confounding factors. The EndoStitch had an overall faster cuff closure time than the RD-180 (17.2 minutes vs. 20.1 minutes, p = 0.046). However, the per-stitch closure times were similar (5.66 minutes/stitch, 5.56 minutes/stitch, p = 0.78). No conversions to laparotomy and no cuff dehiscences were experienced. Per-stitch closure time was not affected by the level of resident, but was lengthened by increased patient body mass index. However, closure times were longer with both devices than when using barbed suture and conventional suturing techniques.
Conclusions:
Both the EndoStitch and RD-180 suturing devices provide a reasonable cuff closure time with a low risk of cuff dehiscence. The learning curve for both instruments is relatively flat. (J GYNECOL SURG 37:227)
Introduction
More than 400,000
One of the more daunting aspects of laparoscopic hysterectomy has been suturing the vaginal cuff. This is often reported as one of the most time-consuming steps in a laparoscopic hysterectomy with average cuff closure time of ∼20 minutes. 4 The technique of the vaginal cuff closure is also important. Vaginal cuff dehiscence is an uncommon but serious complication of hysterectomy, which has been reported to be more likely after laparoscopic hysterectomy. 5 Poor surgical technique in closing the vaginal cuff may increase the risk of cuff dehiscence. Although suturing during laparoscopy can be challenging, several devices are available to aid in suturing during laparoscopic surgery. Given the choice, we wanted to see if there was any difference between devices. Therefore, we compared vaginal cuff closure using the EndoStitch and RD-180 suturing devices from our surgical database, which are the two most common devices used to aid with vaginal cuff closure within our institution.
Materials and Methods
Institutional Review Board approval was obtained to review surgical techniques in laparoscopic hysterectomy at Carolinas Medical Center in Charlotte, NC. A database of cases is maintained by the Division of Gynecologic Oncology and was reviewed for this study. All cases for this study were recorded between April 2006 and March 2016. During that time cases were recorded for teaching purposes for review with the residents as part of a teaching method for reviewing surgical technique. There was no specific case selection, but were often the first several cases performed by the residents rotating on to the service. Inclusion criteria included all cases of laparoscopic cuff closure performed where unedited video of the cuff closure was available and one of the two suturing instruments was used. All cases that met the inclusion criteria were included in this report. The surgeries were performed by residents or junior attending physicians learning laparoscopic hysterectomy with a single senior attending (R.W.N.) assisting. All of the suturing was done by the residents or the junior attending. Review of the video record by a single reviewer (R.A.H.) allowed measurement of vaginal cuff closure time as well as an assessment of the number of sutures used in each closure. The videos are time stamped allowing for accurate measurement of the start time and ending time for the cuff closure. The time for vaginal cuff closure and the number of sutures were recorded. The demographics were retrieved from the patient record. No funding was provided to perform this study. IRB: Atrium Health 01-10-23E, renewal date 12/18/19.
The laparoscopic hysterectomies were performed using a standard surgical technique. Either a 5 or 10 mm camera port was used at the umbilicus. Two 5 mm ports were placed on the right side of the patient, ∼10 cm apart. A single 5 mm port for the assistant was placed in the left lower quadrant. In all cases the suturing was performed by the resident or attending physician who was learning the procedure and assisted by the senior attending physician. For the EndoStitch, a 5 mm camera was introduced into the right upper quadrant port. The 10 mm umbilical port was used to suture and this was performed from the left side of the patient. For the RD-180, the camera remained in the umbilical port and the suturing device was introduced into the right lower quadrant. Suturing was performed from the right side of the patient.
Cuff closure time was defined as the first introduction of the suturing instrument until cutting the final suture. Inclusion criteria for this study included all patients who had a vaginal cuff closure as part of their procedure, the cuff closure time was available through video recording, and the cuff had been closed with either the EndoStitch® (Covidien, Norwalk, CT) or the RD-180® (LSI Solutions, Rochester, NY) suturing devices. All patients are >1 year from the surgery and the medical records were reviewed for readmission in all hospitals within the Carolinas Health care System for possible cuff dehiscence. For the surgeons in training, the device was demonstrated to them at the time of surgery, but no formal or presurgical practice was required other than the standard fundamentals of laparoscopic surgery curriculum and required practice time in the simulation laboratory using conventional suturing techniques. The suturing technique was directed by the senior attending surgeon who was present for the entire vaginal cuff closure.
The knotting technique was also standardized. For the EndoStitch, figure of eight sutures of 2-0 polyglycolic acid were used with the number of sutures placed left to the discretion of the surgeon. The EndoStitch sutures were tied with intracorporal technique. On the RD-180 a 2-0 polydioxanone suture was utilized in a figure of eight manner. Although the RD-180 has a tool that applies a metal crimp to speed knot tying, it was our practice to use an extracorporeal knotting technique to improve the experience for the surgeons in training and reduce the overall cost of the procedure. Use of the suturing device was left to the discretion of the attending. Many of the EndoStitch cases were performed in the beginning of the series and the RD-180 in the later series but considerable overlap occurred in the interest of training the resident physicians on both devices. Toward the end of the study period all cases were converted to unidirectional barbed suture for cuff closure. Demographic information was collected, including patient body mass index (BMI), details of surgery, and level of resident training.
Patients were routinely discharged within 24 hours of surgery. After surgery patients were instructed to restrict lifting >5 kg for the first 2 weeks. After the 2 week postoperative check they were instructed to resume normal activities as tolerated, but were advised to maintain pelvic rest for a total of 6 weeks after surgery. All patients were instructed to call the office in case of any postoperative complications and were directed to one of the health care system emergency rooms if a complication occurred.
Standard statistical methods were used to analyze the data. JMP 5.01 (SAS Institute, Cary, NC) was used for all statistical calculations. Data from the two closure groups were compared using a t-test for parametric data, a Wilcoxon rank test for nonparametric data and analysis of variance for categorical data. Statistical significance was set at a p-value of 0.05.
Results
A total of 105 laparoscopic cases met our inclusion criteria. None of the cases that were video recorded using these suturing devices were converted to open procedures. The EndoStitch was used to close the vaginal cuff in 46 cases and the RD-180 in 59 cases. The demographics of the two groups are shown in Table 1. There was no difference between the two groups with respect to age or BMI. There was no significant difference in the experience level of the residents between the two types of vaginal cuff closure. However, the group of patients where the cuff was closed with the RD-180 had a larger mean uterine size, and trended toward a larger uterine weight and a higher blood loss. This likely reflects a change in types of cases referred for the study period. The average total time to complete vaginal cuff closure was 17.2 minutes for the EndoStitch and 20.1 minutes for the RD-180 (p = 0.046). The trends over time for the two devices are shown in Figures 1 and 2. The learning curve was relatively flat for the two devices with total closure times trending up slightly for the EndoStitch and only slightly down over time with the RD-180. Closure times were comparatively longer than the 56 cuff closures with barbed suture identified during a review of the cases. Using conventional suturing techniques vaginal cuff closure times averaged 9.9 minutes.
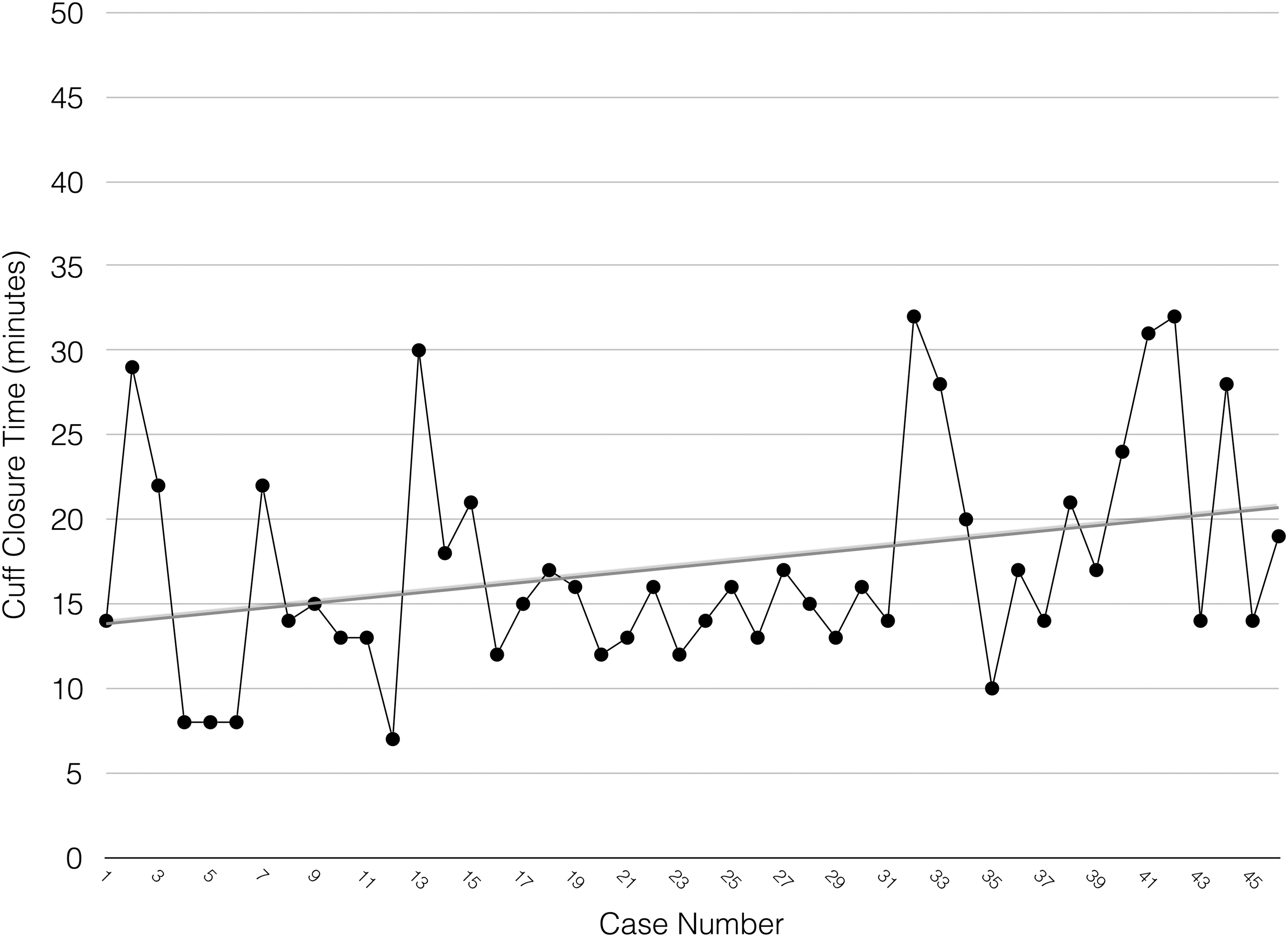
Cuff closure times with EndoStitch. Average closure time is shown as a linear trend line.
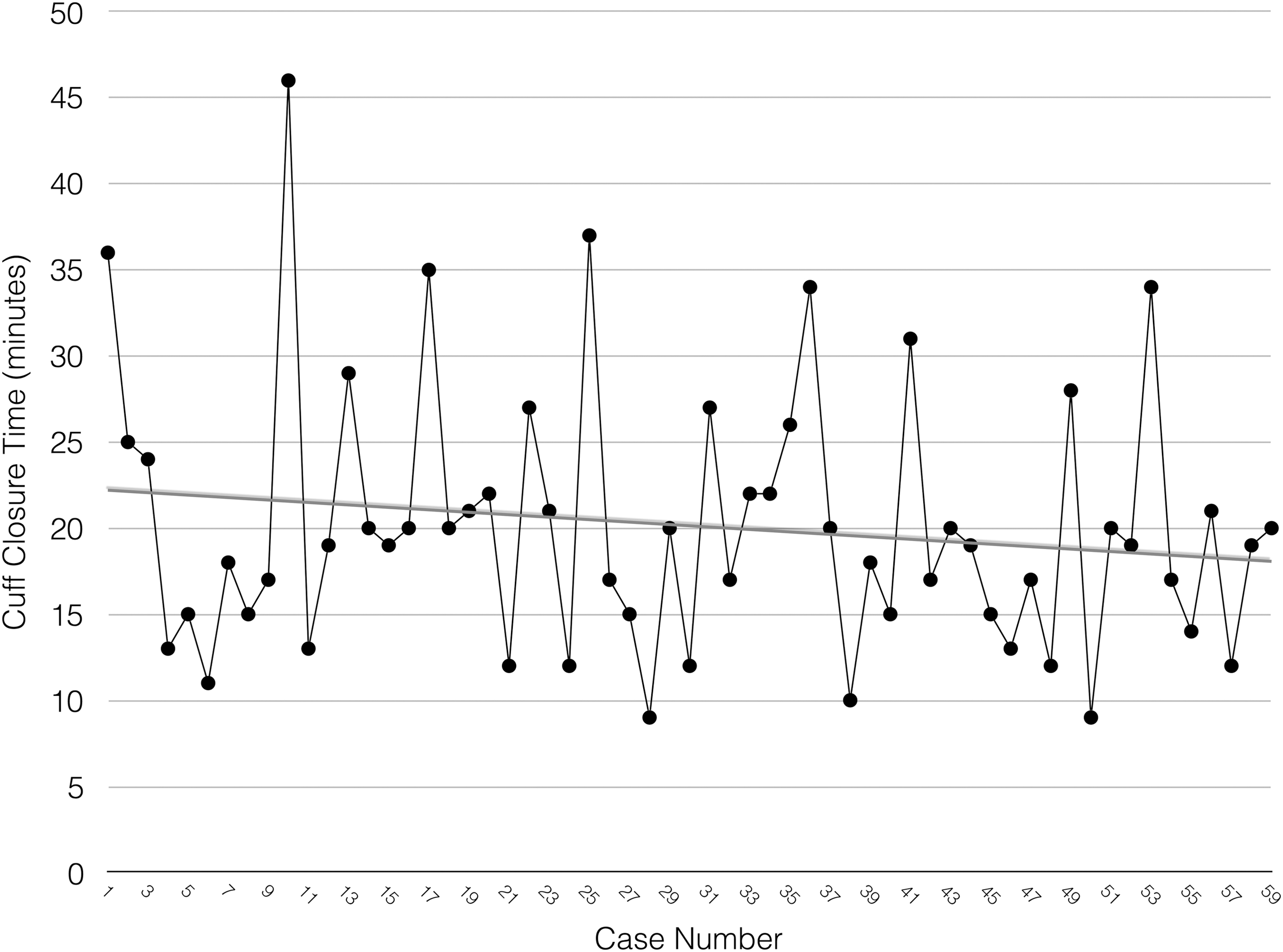
Cuff closure times with RD-180. Average closure time is shown as a linear trend line.
Demographics Between the EndoStitch and RD-180 Vaginal Cuff Closure Groups
Although the cuff closure time was shorter with the EndoStitch, the per stitch times were almost identical between the two devices with 5.66 minutes per stitch with the EndoStitch, and 5.56 minutes per stitch with the RD-180 (p = 0.78). The reason for the difference in total time for vaginal closure between the two devices was that on the average, fewer sutures were used when the EndoStitch device was used. (3.02 vs. 3.63, p < 0.001). These data are summarized in Table 2.
Closure Times and Per Stitch Times for EndoStitch and RD-180
Eighty-two percent of patients were discharged within 24 hours of surgery and 14% stayed up to 3 days due to social issues or medical comorbidity. A hospital stay beyond 3 days was noted in four cases (4%); one for bleeding from an omentectomy for ovarian cancer that did not require surgical intervention, two for an ileus, and one for an intraoperative bowel injury that required reoperation. There were no complications related to the cuff closure and no cuff dehiscences were observed in either group in this series. No patients were readmitted within 30 days of surgery.
Other correlates to cuff closure and per stitch time were reviewed. The time per stitch increased with higher patient BMI (p = 0.048). However, the correlation was weak with an R2 value of 0.04. Although no difference in per stitch time was observed by level of resident surgeon (p = 0.72), the closure times were significantly longer when a junior attending was closing the cuff when compared with the fourth year residents (22.9 minutes vs. 17.4 minutes, p = 0.03). However, there was no significant difference between the EndoStitch and RD-180 groups with respect to closure times when analyzed by experience of the resident surgeon as shown in Table 3.
Closure Times (95%tile) by Resident Level and Type
The cost of the cuff closure was higher with the RD-180 as compared with the EndoStitch ($341.16 vs. $279.87). These prices represent the cost to the hospital and take into account the number of sutures used. The cost of the RD-180 would increase by another $320.20 if the suture-crimping tool was used to tie the knots. In contrast, the cost of the barbed suture was only $21.69.
Discussion
A comparison between the EndoStitch and the RD-180 suturing devices shows little difference in the functionality or speed of suturing, with the only difference being influenced by the number of sutures used. Both devices had a relatively flat learning curve suggesting that they are easily mastered, even by less experienced surgeons. There was a slightly longer closure time for inexperienced attending surgeons, but this may be due to the fact they had less laparoscopic experience than the residents that were performing the cases, or the cases they were involved in were more difficult. The RD-180 was only slightly more expensive as long as the crimping tool was not used to close the vaginal cuff.
Early reports of laparoscopic hysterectomies were associated with a significant incidence of vaginal cuff dehiscence over other types of hysterectomy. 5 This is likely due to a combination of surgical technique and the way the vaginal cuff was sutured. The dehiscence rate was alarmingly high in early series, with rates approaching 5%. 5 However, experience has lessened the initial high rate with much lower rates of vaginal dehiscence reported in more recent series. 6 Despite the improvement in cuff dehiscence rate, the rate of 0.61% for laparoscopic hysterectomy is higher than that the 0.21% rate for abdominal hysterectomy or the 0.13% rate for vaginal hysterectomy. 7 Interestingly, the rate of cuff dehiscence is lower after transvaginal suturing at laparoscopic hysterectomy (0.24%) as compared with laparoscopic suturing (0.83%). Cuff dehiscence did not appear to be altered by the use of monopolar energy for colpotomy or the energy setting used during colpotomy when comparing transvaginal and laparoscopic cuff closures. This would raise the possibility that the suturing technique is an important aspect of cuff integrity.
The cuff closure also appears adequate with both devices, as there were no cuff complications reported in this series. Although the EndoStitch requires a 10 mm port size and a change to a 5 mm camera in a different port, the bite size on the EndoStitch is larger and it was felt that this may protect against cuff dehiscence. However, this did not appear to be measurable in this series since there were no cuff dehiscences and the reported rate for experienced surgeons is too low to directly compare the cuff dehiscence rate between the two devices. The only possible observed advantage of the EndoStitch is the larger bite, compared with the 5 mm device and this may have been responsible for the fewer number of sutures required to close the cuff resulting in a shorter closure time. Conversely, the RD-180 is a 5 mm device and does not require a larger port at the umbilicus or a camera change if a 10 mm camera is being used. This study was not randomized and most of the cases using the RD-180 were after those where the EndoStitch was used. Although the experience of the surgeons may have improved times in the later group, we do not believe this had a significant impact on the outcome of this study since the learning curve for both instruments was flat over time and there was no significant difference noted between the level of experience of the resident performing the procedure (Table 3).
These suturing devices appeared to have a flat learning curve and were easily mastered. However, one of the more challenging aspects of laparoscopic suturing was the knot tying. Since these data were collected, significant changes have been made to the EndoStitch with the addition of barbed suture that does not require an intracorporeal knot. In addition, the RD-180 has a knot tying device that can speed suturing. However, both of these innovations are more expensive and must be weighed against the amount of time saved in the operating room. A less expensive alternative to suturing devices is to use conventional suturing with intracorporal knot tying. The use of a laparoscopic running cuff closure with a unilateral barbed suture has been associated with a decreased operative time and no increase in complications and this has become the procedure of choice for resident training in our hospital. 8 In cases that were identified in our series where barbed suture was used, the average closure time was significantly less than either of the automated devices at 9.9 minutes. However, conventional suturing is a skill that needs to be practiced and used frequently to master and it is our observation that devices to assist with suturing are still used in >40% of cases in our hospital system.
It appears that both the EndoStitch and RD-180 are easy to learn based on the flat learning curve. These devices allow for effective vaginal cuff closure with reasonable surgical times. These devices can be used by gynecologic surgeons who want to close the vaginal cuff laparoscopically but are not comfortable using traditional suturing techniques, or in situations where conventional suturing might be very challenging as with single port surgery. It appears that both of these devices are an option and appear to offer comparable closure times and outcomes.
Footnotes
Authors' Contributions
Study concept, design, and acquisition of data by R.W.N., A.R.N., and R.A.H. Analysis and interpretation by R.W.N. and A.R.N. Study supervision by R.W.N.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.