
Abstract
Background:
Cystadenofibromas (CAFs) are defined as benign mixed mullerian tumors. They are diagnosed mainly in the ovary. Nonetheless, extraovarian locations, such as endometrium, uterine cervix, fallopian tube, and parasalpinx, were reported. Clinical course is commonly asymptomatic, and tumors are often diagnosed on histology after adnexal cyst surgery for benign indications.
Case:
A 13-year-old female was admitted into our emergency room with acute lower right abdominal pain as her main complaint. Abdominopelvic ultrasonography showed a right adnexal unilocular cyst with small papillary projections on the inner wall of the cyst, with no apparent solid component.
Result:
During laparoscopy, two cystic masses dependent on the distal region of the right fallopian tube were seen. After fluid aspiration of the first cyst, capsule was opened to see the nodular formations (papillary projections) previously described by ultrasonography. Right salpingectomy was performed due to high suspicion of a borderline tumor. Histopathologic diagnosis was compatible with a serous CAF.
Conclusion:
In our case we tried an intraoperative evaluation of the inner surface of the cyst, observing papillary projections that were regular and well adhered to their wall. However, microscopic pathology assessment of the tumor is mandatory to have definitive diagnosis. Surgical treatment, especially in child and youth population, should be conservative and adnexectomy should be avoided. Laparoscopic approach is often successful and can be considered in these cases. Although previous published cases were diagnosed in an incidental manner, our case highlights the importance of a thorough intraoperative assessment of adnexal tumors in child and adolescent patients.
Introduction
Cystadenofibromas (CAFs) are defined as benign mixed mullerian tumors. Usually they are of a serous type, diagnosed mainly in the ovary. They have been reported in extraovarian locations, such as endometrium, uterine cervix, fallopian tube, and parasalpinx. Unilaterality is a common characteristic. These tumors can arise at any age, although most cases are reported in women between 40 and 50 years of life. Clinical course is commonly asymptomatic, being diagnosed on histology samples after routine adnexal cyst surgery for benign indications. Gross characteristics outline smooth and glistening cystic tumors, sometimes with multiple cavitations filled with serous fluid and partial involvement of the inner surface of the cyst with tendency to form papillary nests.1–3
We present the first published case of a serous CAF of the fallopian tube in a 13-year-old female. Intraoperative assessment and laparoscopic salpingectomy were performed in a successful intervention.
Case Description
A 13-year-old female was admitted into our emergency room with acute lower right abdominal pain. She reported nausea and vomiting at the moment of medical history interview. There was no history of chronic diseases or surgeries. Menarche occurred at age 11 years and the patient reported regular menses with no dysmenorrhea. She denied sexual activity.
Physical examination revealed a body mass index of 31.1 kg/m2; Tanner Stage 4. Abdominal examination revealed a soft abdomen with mild guarding and pain in the right lower quadrant. Rest of the examination was unremarkable. Serum analyses were in normal ranges. Tumor markers (cancer antigen 125 [CA-125], carcinoembryonic antigen [CEA], alpha-fetoprotein [AFP], and lactate dehydrogenase [LHD]) were in normal values.
Abdominopelvic ultrasonography showed a unilocular cystic mass on the right ovary with a size of 71 × 64 × 59 mm with a low-level echogenicity of cyst fluid. Small papillary projections were seen on the inner wall of the cyst, with no apparent solid component. Color Doppler exploration found no vascularization. No free fluid was noted. The uterus and left adnexa appeared normal.
During laparoscopy, two cystic masses dependent on the distal region of the right fallopian tube were seen (Fig. 1). The first one was with a size of 70 × 70 mm, and the second mass was of 15 × 15 mm. The rest of pelvic structures were of normal appearance. After fluid aspiration of the first cyst, the capsule was opened to see the nodular formations (papillary projections) previously described by ultrasonography. After noticing a compromise >50% of the internal surface of the cyst (Fig. 2), right salpingectomy was performed due to high suspicion of a borderline tumor.
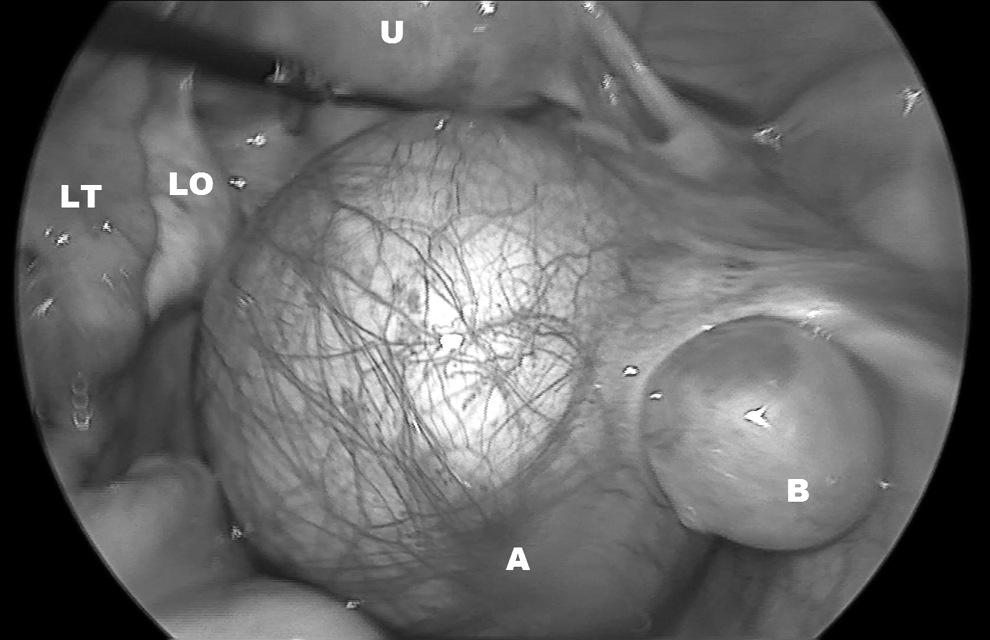
Laparoscopic view of right adnexal mass, fallopian tube dependent. A, cystadenofibroma; B, simple cyst; LO, left ovary; LT, left tube; U, uterus.
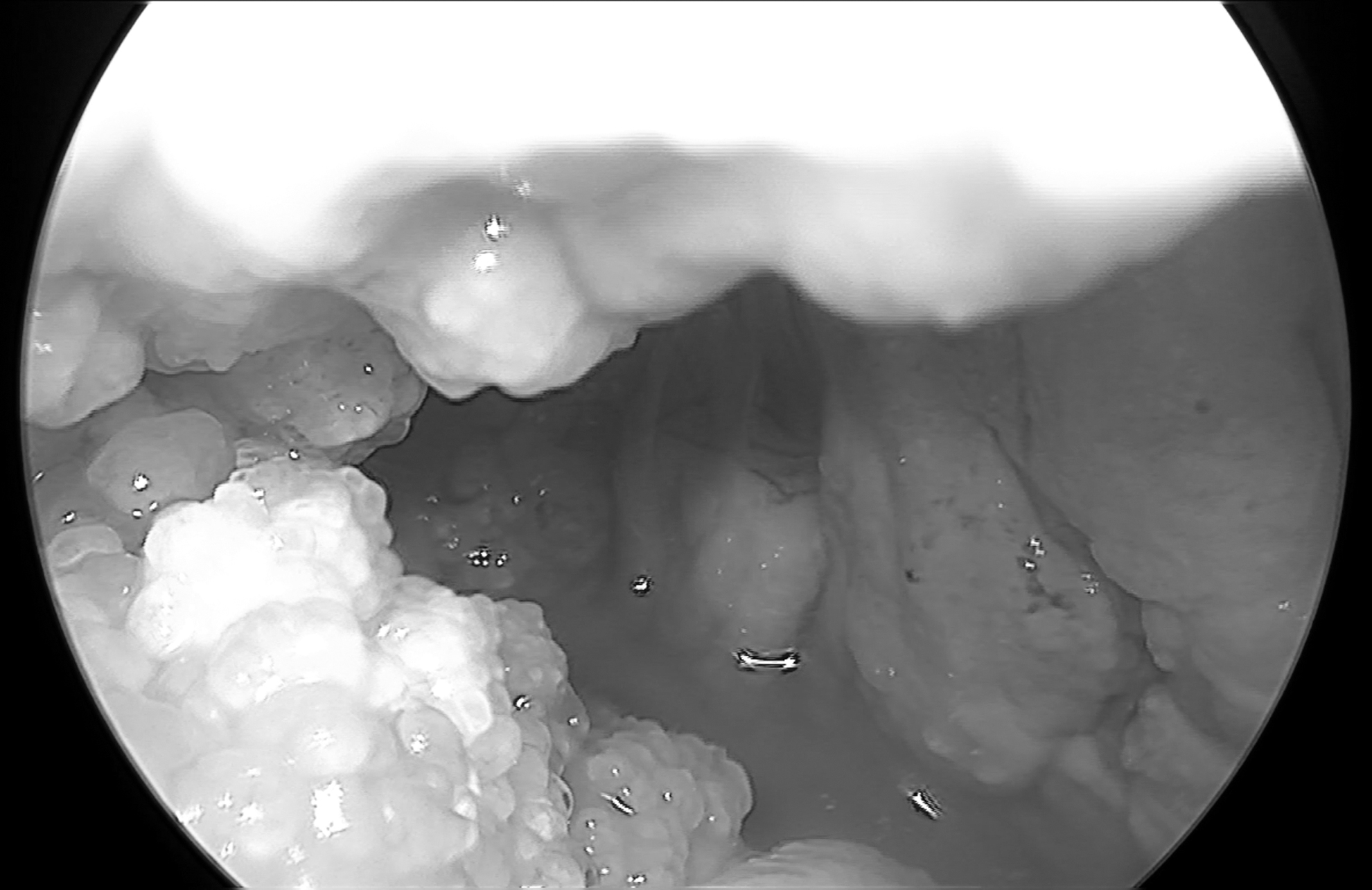
Intraoperative evaluation of inner surface of adnexal mass, nodular formations occupied >50% of the surface.
Gross pathology of the larger mass was reported as a cystic empty tumor of 60 × 40 × 10 mm, with a smooth external surface and grayish brown. Internal surface exhibited hard excrescences (papillary projections) in ∼60% of its surface. Histopathologic diagnosis was compatible with a serous CAF. The smaller mass was reported as a serous cystadenoma.
The patient was discharged after 24 hours from surgery. Follow-up at 1 week and at 1 month were uneventful.
Discussion
CAF is a rare benign tumor diagnosed in women. Fallopian tube localization is extremely rare, with just 20 cases published so far.1,2 They usually appear as a solitary mass located at the fimbriae, but they can also be intraluminal. As previously described, they usually go asymptomatic until an ultrasonography or an elective gynecologic surgery is performed. Age of presentation varies between 19 and 73 years old. Our case is the first known case of serous CAF of the fallopian tube in a 13-year-old female.
These tumors can be predominantly cystic, cystic with a variable percentage of solid component or predominantly solid. They usually are small masses, but atypical presentations in size were reported, being 180 mm of diameter the biggest one published so far. One common characteristic is the presence of papillary projections in the inner surface of the cyst. It has been described that at lower ages, CAFs show small papillary projections and as age increases papillae become fibrotic nodules.4,5
Presurgical and intraoperative diagnosis of CAF can be difficult, as both ultrasonography and intraoperative visualization give impression of malignancy. Some authors have tried to identify patterns that suggest benign pathology in these kinds of adnexal masses, such as fine and regular vegetations, usually observed at ultrasonography. Complete preoperative work-up of our patient showed a low potential for malignancy. Therefore, we tried an intraoperative evaluation of the inner surface of the cyst to decide for a cystectomy-only procedure. We observed papillary projections that were regular and well adhered to their wall. Nonetheless, compromise of >50% of the inner surface of the cyst plus the high chance of a nonfunctional remaining fallopian tube moved us toward salpingectomy. Ultimately, microscopic pathology assessment of the tumor is mandatory to have definitive diagnosis.3,5
Histology of these tumors show a proliferative connective tissue stroma of variable density, also groups of edematous papillae on the inner surface of the cyst upholstered by a monolayer of cuboidal or columnar cells. 6 In addition, hard firm papillary projections are best related to benign masses in gross pathology. Hence, intraoperative visualization of such characteristics could help in the decision of future cases.
Surgical treatment, especially in child and youth population, should be conservative 7 and adnexectomy should be avoided. Laparoscopic approach is successful and ideal for cases like ours. Although previously published cases were diagnosed in an incidental manner, our case highlights the importance of a thorough preoperative and intraoperative assessment of adnexal tumors with a low potential of malignancy in child and adolescent patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.