
Abstract
Objectives:
The effects of an algorithm for postoperative prescriptions on opioid-prescribing practices, pain-related postdischarge clinical encounters, and patient satisfaction were studied.
Materials and Methods:
A quality-improvement initiative was implemented at a single, tertiary-care, comprehensive cancer center. Perioperative patient education was restructured with detailed verbal and written components. An algorithm for postoperative discharge medications included prescribing nonopioid analgesics to all patients without contraindications. Opioid prescriptions were based on patients' length of stay and inpatient opioids' use. Data on opioids prescribed and postoperative encounters for pain were collected, and surveys at a postoperative visit were taken on patient satisfaction pre- and postintervention. Groups' results were compared.
Results:
The patients (107 preintervention and 90 postintervention) had similar demographics. The postintervention group had a 25% reduction in median number of opioids prescribed at discharge (p = 0.16), with similar patterns of postoperative encounters for pain and frequency of opioid refills. Patient satisfaction, assessed in 29 preintervention and 40 postintervention participants, had significant improvement; 95% postintervention participants answered that they were satisfied with their pain control, compared with 75% preintervention participants (p = 0.03).
Conclusions:
Perioperative education plus an algorithm for postoperative discharge medications in gynecologic oncology patients results in improved patient satisfaction, a trend toward fewer opioid prescriptions, and a similar pattern of postoperative pain encounters. Comprehensive perioperative education is effective for improving patient satisfaction and pairs well with an algorithmic approach to decreasing opioid prescriptions. (J GYNECOL SURG 20XX:000)
Introduction
While the opioid epidemic has required increased scrutiny of postoperative prescribing practices, there remains a need for optimized pain control, especially in an oncologic population. At baseline, ∼6%–8% of opioid-naïve patients undergoing noncancer procedures may develop persistent opioid use. 1 The risk for this long-term sequela appears to be heightened in patients with cancer—as high as 15%–21% in patients receiving curative-intent surgery combined with adjuvant chemotherapy. 1
Other risk factors for persistent opioid use include increased perioperative opioid dosage, postoperative prescription for a longer period of time, 2 and worse physical classification status by American Society of Anesthesiologists (ASA) status. 3 Each of these risks are prevalent among gynecologic oncology patients, and among them, the only modifiable risk factors are the perioperative opioid dosage and number of days opioid supply is prescribed. Additionally, few patients with excess opioids dispose of them appropriately, 4 adding a societal risk of diversion to the individual patient risks. Despite these risks, it is well-known that in gynecologic oncology, as well as across other surgical disciplines, there is a tendency toward overprescribing opioids postoperatively. 5
For these reasons there has recently been great interest in standardizing and reducing the volume of opioids prescribed to patients postoperatively across surgical specialties. Some recommendations and guidelines have been published, 6 and these guidelines recommend a broad range of recommended doses per procedure (i.e., 0–20 doses), leaving room for much variation within those guidelines. In addition, these guidelines are generalized and do not account for the highly complex procedures that are often performed in gynecologic oncology surgery.
Finally, procedure-specific guidelines are limited in that they fail to account for the highly complex mosaic of factors that interact with—and determine—a patient's unique pain experience. These factors include psychosocial processes, demographic variables, and genetic components of the pain experience. Interestingly, an individual's genetic variants can not only affect pain sensitivity and intensity of postoperative pain, 7 but also determine the pharmacokinetics of a patient's opioid metabolism. In combination, these genetics contribute to the true drug exposure experienced by a patient. 8 These complex factors would presumably influence a patient's pain-medication needs immediately postoperatively; therefore these needs could be accounted for in predischarge opioid requirements. This conceptual approach has been shown to be effective in a general surgical population, 9 and, in 2020, a similar association was identified in post-cesarean–opioid use. 10
After divisional agreement upon an algorithm, a quality-improvement initiative was implemented. It was focused on the perioperative-education program and postoperative discharge opioid prescriptions provided to the current authors' postoperative patients. The study aims included reducing variation within the practice, improving patients' experiences, and assessing the effects on opioid prescribing.
Materials and Methods
Patients
The study population consisted of postoperative patients for whom a gynecologic oncology faculty member was the primary surgeon, whether for malignant indications or otherwise. Surgeries performed in the study population included minor outpatient procedures (such as cervical excisional procedures), minimally invasive staging procedures, and extensive debulking procedures and bowel surgeries (Table 1).
Demographics for Pre/Postintervention Chart Reviews
Any complications within 30 days of surgery, included emergency-room visit, readmission, surgical-site infection, return to the operating room, ileus, thromboembolism, and neuropathy.
ASA physical classification score.
Medi-Cal insurance: Patient receives free or low-cost health coverage (for California residents who meet eligibility requirements based on federal poverty levels).
LND, lymph-node dissection; SD, standard deviation; ASA, American Society of Anesthesiologists; LOS, length of stay; hrs, hours; BMI, body mass index; IQR, interquartile range.
Peripartum patients were excluded if their discharges were managed by the obstetric team involved or if patients had multiple surgeries. Patients who were discharged to skilled nursing facilities were also excluded as their facility providers took responsibility for pain-control prescribing.
For assessment of opioid prescribing, the a preintervention cohort included patients who underwent surgery from July 1 through September 30, 2019. The discharge-medication algorithm (Fig. 1) was designed and implemented starting on October 7, 2019, and the comprehensive perioperative educational program was implemented on October 14, 2019. Allowing for a timeperiod of implementation and normalization of this algorithm, the postintervention cohort included patients who underwent surgery from December 7, 2019, until March 1, 2020.
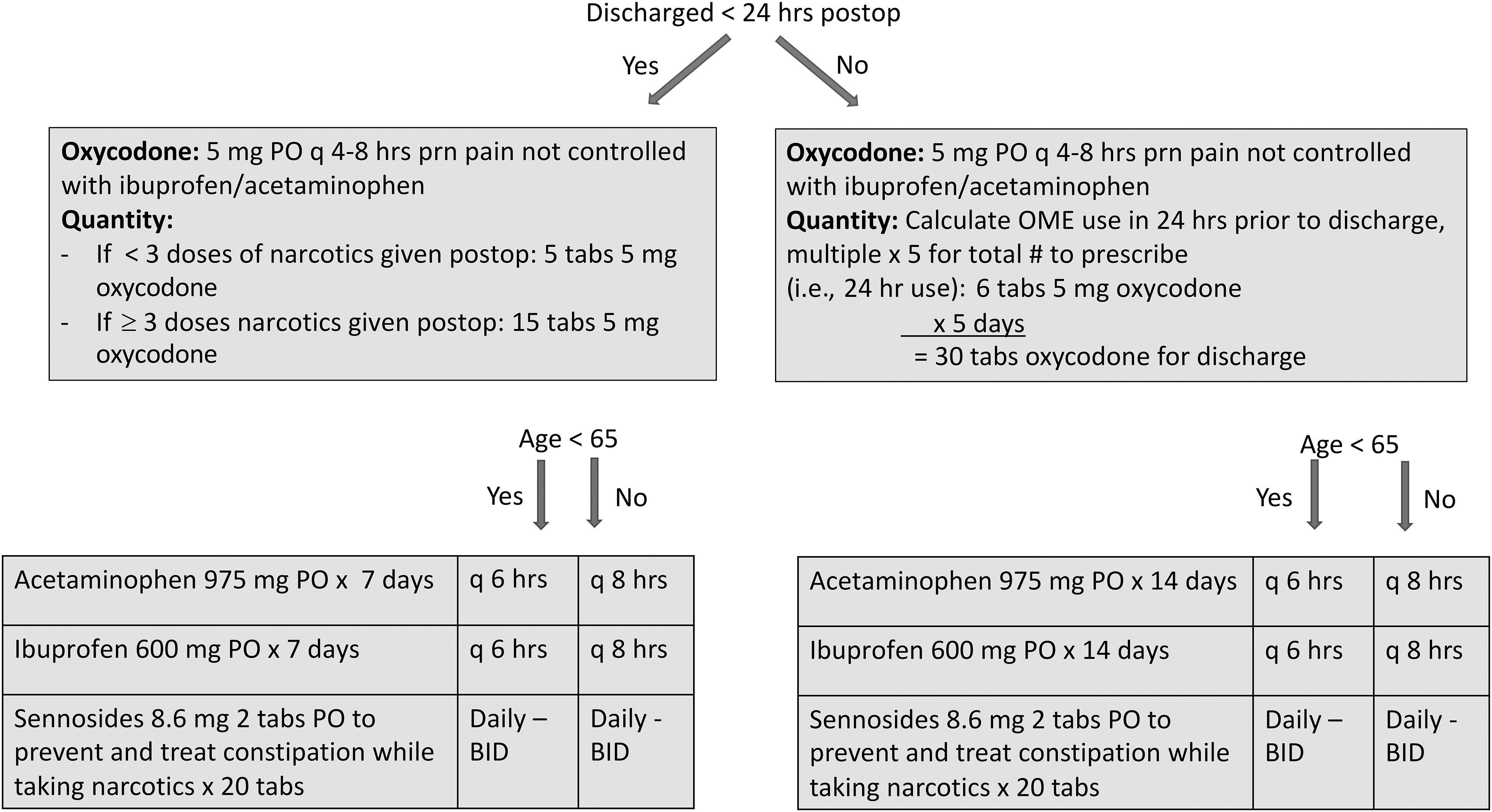
Algorithm for opioid prescriptions. Note: If any patient was intolerant to oxycodone or otherwise required alternatives, equivalent OMEs were calculated and prescribed. hrs, hours; postop, postoperative; PO, per os (orally); prn, pro re nata (as needed); tabs, tablets; q, quarterly; OME, oral morphine equivalent; BID, bis in die (twice per day).
For the patient-satisfaction component of the assessment, the eligible preintervention cohort included patients who underwent surgery between September 1 and October 7, 2019. Allowing for a timeperiod of implementation, the postintervention cohort included patients who underwent surgery from December 7, 2019, until March 1, 2020. This analysis also excluded patients who had multiple surgeries/admissions—and, therefore, may have filled out more than 1 survey—and patients who chose not to fill out a survey.
Intervention design
The quality-improvement initiative was implemented at a single tertiary-care comprehensive cancer center and involved significant changes in patients' perioperative care. First, the schedule and quantity of nonopioid analgesics prescribed upon discharge were standardized. Nonopioid prescriptions were intended as primary methods of pain control and were modified based on the duration of postoperative stays and patients' ages. Second, preceding literature regarding opioid prescribing practices were reviewed, and the idea incorporated that an individual's discharge pain-control needs could be predicted by that patient's immediate inpatient pain-control requirements.9,10 The algorithm was then modified as needed to obtain a faculty consensus (Fig. 1). Those needs were calculated by the resident physician on the gynecologic oncology service at the time of discharge after teaching by the primary author (Dr. Owens).
Third, the preoperative patient education program was overhauled to highlight scheduled nonopioid analgesics, appropriate expectations, and appropriate opioid disposal at home. A detailed booklet about the perioperative experience was provided to each patient and was reviewed during a preoperative visit. Finally, postoperative patient surveys were implemented at postoperative visits to assess patient satisfaction at that time (Supplemental Material 1).
Data-collection methods
The data analysis department provided chart extractions for patients in the requested time intervals. The chart extractions included much of the demographic information about the patients. A manual chart review was then performed to ascertain the following additional demographic components: surgical components; postoperative clinical encounters for pain control; pathology categorization; presence of postoperative complications; and prescribed oral morphine equivalents (OMEs) at discharge. A Centers for Medicare and Medicaid Services chart on opioid oral morphine mg equivalent calculations was used to calculate discharge OMEs (dcOMEs). 11
For some survey questions, several responses were aggregated into binary groups (e.g., responses “satisfied” and “highly satisfied” were aggregated into a “satisfied” group). Surveys included written responses explaining how leftover opioid medications would be disposed. A physician manually evaluated such responses and categorized the responses as “appropriate” or “not appropriate” according to the U.S. Food and Drug Administration (FDA) guidelines. 12 Figures and graphs were generated with R statistical computing software (R Core Team, 2020).
Statistical-analysis methods
Intervention-group comparisons were compared using a χ 2 or Fisher's exact test for categorical variables and analysis of variance or Wilcoxon rank-sum tests for numeric or ordinal variables. A linear mixed-effects model was used to assess the intervention, length of stay (LOS), and interaction between the 2 on dcOME. SAS® software version 9.4 for Windows® was used in all analyses.
Results
A total of 107 preintervention and 90 postintervention cases were assessed via chart reviews for the quantitative components of this analysis. Patient demographics and characteristics between the 2 cohorts were similar (Table 1). The postintervention group had a 25% reduction in the median amount of opioids prescribed at discharge (p = 0.16; Table 2). This reduction was mostly accounted for in the <24-hour stay group, which had a 50% reduction in the median amount of opioids prescribed. In the multivariable model accounting for length of stay and interaction with intervention, there were no significant effects of the intervention (Table 3). There was no evidence of an increase in 30-day postoperative encounters for pain (15.89% versus 11.11%; p = 0.33) or opioid refills (6.54% versus 8.89%; p = 0.536) after implementation of this algorithm.
Discharge Oral Morphine Equivalents
p = 0.16.
Discharge Oral Morphine Equivalents analysis by Length of Stay
p = 0.13.
LOS, length of stay; hrs, hours.
Subjective data, including patient satisfaction and pain, were compared between the pre- and postintervention groups with voluntary patient surveys. Again, patient demographics and characteristics between the 2 cohorts were similar (Table 4). A total of 30 preintervention and 41 postintervention patients completed the survey, corresponding to a total survey response rate of 52%.
Demographics of Patient-Survey Respondents
Any complications within 30 days of surgery, included emergency-room visit, readmission, surgical-site infection, return to the operating room, ileus, thromboembolism, and neuropathy.
ASA physical classification score.
Medi-Cal Insurance: Patient receives free or low-cost health coverage (for California residents who meet eligibility requirements based on federal poverty levels).
LND, lymph-node dissection; SD, standard deviation; ASA, American Society of Anesthesiologists; LOS, length of stay; hrs, hours; BMI, body mass index; IQR, interquartile range.
Patient satisfaction regarding pain control and management was compared between the pre- and postintervention groups. The pre- and postintervention groups felt similarly prepared to manage their pain prior to surgery (88% versus 83%; p = 0.73; Fig. 2 ). More postintervention patients were satisfied with their pain control after discharge, compared to preintervention patients (95% versus 76%; Fig. 2), with a statistically significant improvement in satisfaction (p = 0.03).

Patient satisfaction and readiness to manage pain.
The amount of unused opioid pills was compared between the pre- and postintervention groups. In patients with postoperative stays <24 hours, more postintervention-survey respondents indicated that they had 6 or more unconsumed opioid pills than the preintervention group (88% versus 44.4%; p = 0.30; Fig. 3), despite being prescribed fewer opioids overall. However, with longer postoperative stays (> 24 hours), both patient cohorts had similar numbers of unused opioid pills (Fig. 3). In addition, patients were asked to assess if they were prescribed appropriate amounts of pain medication. Regardless of postoperative LOS, most pre- and postintervention patients described their prescribed amounts as “just right” (Fig. 4).
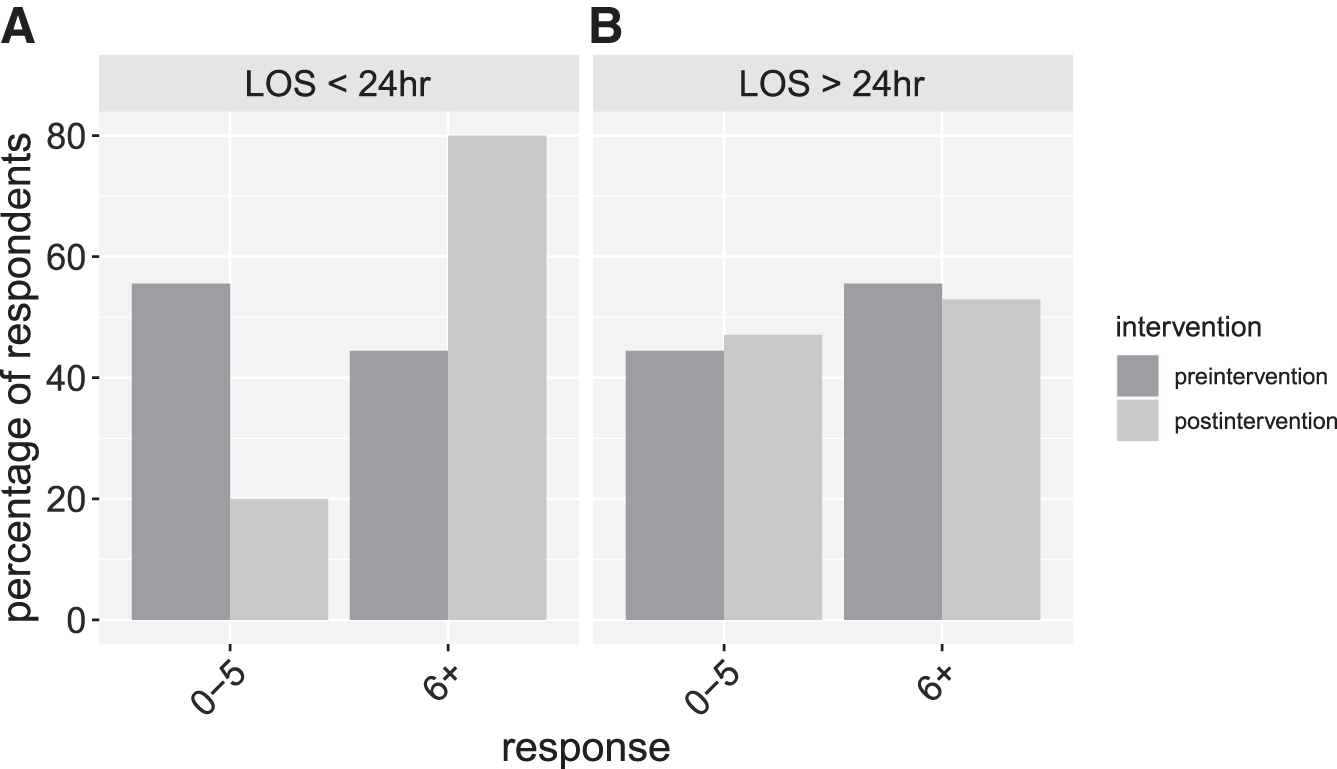
Number of remaining opioid pills, stratified by length of stay after surgery. Patients were asked: “If you received opioids and no longer need them, how many pills are left over?” Responses were divided between patients with

Patients' perception of opioid prescription amounts stratified by length of stay after surgery. Patients were asked: “How do you feel about the number of pills you were prescribed (even if none were prescribed)?” Responses were divided between patients with
Part of the intervention protocol included preoperative education about appropriate disposal of opioid medications. To assess if the intervention was associated with changes in patients' behaviors, patients were asked to indicate their plans for disposal of their unused opioid medications. These written responses were evaluated by a physician and categorized as appropriate or inappropriate according to U.S. FDA guidelines. 12 Similar proportions of preintervention (23.5%) and postintervention (18.2%) patients reported appropriate disposal plans for unused medication (p = 0.71), indicating that the intervention protocol did not improve the likelihood of appropriate opioid disposal.
Discussion
This analysis showed that implementation of a personalized discharge-medication algorithm and an enhanced perioperative education process resulted in a trend toward reduced opioid prescriptions with improved patient satisfaction and without a significant difference in clinical encounters for postoperative pain.
Although statistical significance was not reached in reduction of opioid prescriptions, it is also notable that the preintervention mean prescribed OME was relatively low at 124.71, in contrast to a previously published work on a similar population that described a preintervention mean dcOME nearly double that of the current study.
13
A substantially larger sample size would likely be needed in the current study to reach statistical significance if the trend continued. For perspective, this OME correlates to prescribing a baseline mean of 16.63 5-mg tablets of oxycodone versus a postintervention mean of 109.78 OME, correlating to prescribing 14.64 5-mg tablets of oxycodone. It is unlikely that a difference of 2 5-mg tablets of oxycodone has any clinically significant benefit. Additionally, a recent article reported lower dcOME, but after only minimally invasive surgery
Of note, no inpatient practices were changed for this project, although a formalized ERAS [Enhanced Recovery After Surgery] order set had been implemented several months prior to the study timeperiod. The timing of this change could have been a confounding factor, but this was less likely, as the inpatient pain regimen was not changed from previous practices.
After completion of this intervention, there were several areas identified for further improvement. First, for patients with a discharge from the post-anesthesia care unit (PACU), assessment of PACU opioid use proved to be somewhat cumbersome, as for any likely PACU discharges it is the standard workflow for team members to write the discharge medications upon completion of the case. Awaiting assessment of PACU medication use was an additional burden on the team and could result in delay of discharge due to awaiting medications being filled by the discharge pharmacy.
Therefore, the current authors would consider use of a standard prescription for all same-day discharges (i.e., 5–10 tablets) for improved workflow, while still keeping opioid prescriptions at a low volume. In 2021, Straubhar et al. published their work, which was conducted during a similar time frame as the current study and that utilized their own unique algorithm to determine the opioids prescribed postoperatively. 15 The current authors suspect that there could be a variety of effective approaches toward an optimized solution and agree with Straubhar et al.'s conclusion that “tailored algorithms can aid surgeons in balancing the societal risk of prescription opioids with individual needs for acute pain control postoperatively.” 15
A venue for high-volume and high-variance opioid prescribing that was not accounted for was postoperative opioid refills. Although this was a factor in only a small percentage of patients, many refills were prescribed by individuals not involved in the patients' operative care (i.e., outpatient nurse–practitioners or overnight-resident call team members), and had wide variance in the prescription refills. This is an area for further investigation, as enhanced education of the care team may be another area for improvement.
Based on the survey data, patient satisfaction was improved postintervention (Fig. 1). Interestingly, both intervention groups believed that they were prescribed the appropriate quantity of pills, even with the trend toward reduction in prescription quantities for postintervention patients (Fig. 3). Collectively, these data suggest that patients can be satisfied with lower dosing regimens and that other variables, such as perioperative education, may improve satisfaction. In addition, a high proportion of patients in both intervention groups indicated that they had more than 6 opioid pills remaining (Fig. 2). This suggests the possibility of overprescription across both groups, despite the trend toward reduction in opioid prescriptions in the postintervention patients.
Perioperative education did not improve disposal behavior of unused opioids. More than 75% of both pre- and postintervention patients reported inappropriate disposal plans for their unused medication. Similar studies have found that patient education and literature did not change the way opioids are disposed. 16 However, drug-disposal products, such as drug-disposal bags with activated charcoal, have improved proper disposal behavior. 17 These products represent a promising avenue for future research with respect to gynecologic surgery.
Conclusions
Perioperative education paired with a standardized algorithm for postoperative discharge medications in gynecologic oncology patients results in improved patient satisfaction, a trend toward lower opioid prescriptions, with similar needs for postoperative pain encounters. A comprehensive perioperative educational program does not add clinical burden, is effective for improving patient satisfaction, and pairs well with the trend toward decreasing opioid prescriptions.
Footnotes
Authors' Contributions
All of the authors contributed to the design and implementation of the research, analysis of the results, and writing the article.
Author Disclosure Statement
No financial conflicts of interest exist.
Funding Information
This research was supported by the National Center for Advancing Translational Sciences, of the National Institutes of Health, through grant number UL1 TR001860 (to Drs. Ponzini and Wilson). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.