
Abstract
Abstract
Wu, Tian Yi, Shou Quan Ding, Sheng Lin Zhang, Jin Qing Duan, Bao Yu Li, Zhong Yan Zhan, Qin Li Wu, Suolung Baomu, Bao Zhu Liang, Shu Rang Han, Yu Ling Jie, Gang Li, Lin Sun, and Bengt Kayser. Altitude illness in Qinghai–Tibet railroad passengers. High Alt. Med. Biol. 189–198, 2010.—It takes ∼24 h to travel the ∼3000-km-long Qinghai–Tibet railroad of which 85% is situated above 4000 m with a pass at 5072 m. Each year about 2 million passengers are rapidly exposed to high altitude traveling on this train. The aim of this study was to quantify the occurrence of altitude illness on the train. Three subject groups were surveyed: 160 Han lowlanders, 62 Han immigrants living at 2200 to 2500 m, and 25 Tibetans living at 3700 to 4200 m. Passengers reached 4768 m from 2808 m in less than 1.5 h, after which 78% of the passengers reported symptoms, 24% reaching the Lake Louise criterion score for AMS. AMS incidence was 31% in nonacclimatized Han compared to 16% in Han altitude residents and 0% in Tibetans. Women and older subjects had a slightly greater risk for AMS. Most cases of AMS were mild and self-limiting, resolving within days upon arrival in Lhasa. Some cases of more severe AMS necessitated medical attention. To curb the health risk of rapid travel to altitude by train, prospective travelers should be better informed, medical train personnel should be well trained, and staged travel with 1 to 2 days at intermediate altitudes should be suggested to nonacclimatized subjects.
Introduction

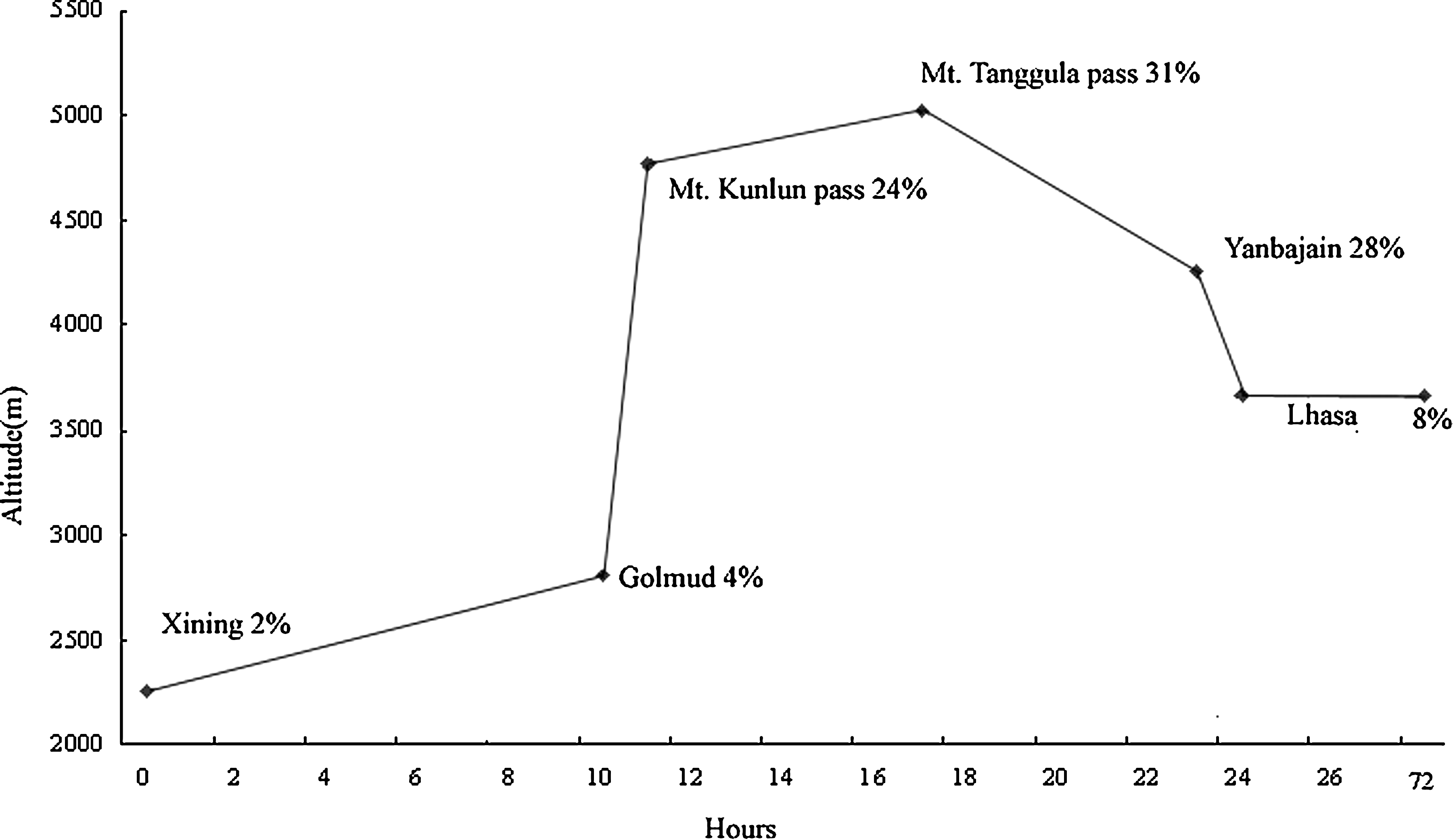
Altitude versus travel time from Golmud to Lhasa. Indicated are the main railway stations and the distance traveled from Xining. *Sites where measurements were performed.
Methods
Subjects and groups
Three subject groups were surveyed (Table 1). The first concerned 160 Han lowlanders (39% female). Average age was 41 ± 14 yr (mean ± SD), range 22 to 69 yr. This group consisted of 114 Han lowlanders randomly chosen from the 868 passengers boarding the first train in Beijing in 2006 and 46 Han lowlanders recruited from 46 passengers boarding a train in Xining in 2007. The latter had traveled to Xining by air, arriving in the morning, before boarding the train to Lhasa, and spent 4 h in Xining prior to departure on the train. Ninety-six percent of the subjects were from regions close to sea level; the remaining 4% were from places located below 1000 m; none were acclimatized. The second group consisted of 62 Han immigrants (40% women) who permanently had resided at moderate altitude (2200 to 2500 m) around Xining for 5 to 10 yr. Average age was 40 ± 11 yr, range 21 to 56 yr. The third group consisted of 25 native Tibetans (40% female) who resided at altitudes between 3700 and 4200 m in the neighboring areas of northern Qinghai. Average age was 38 ± 11 yr, range 18 to 62 yr.
There were no significant differences among groups for sex, age, and BMI.
Acute mountain sickness (AMS) prophylaxis with Rhodiola (a Tibetan herb) was reported by 19 (7%) of all subjects; none reported taking acetazolamide or dexamethasone, except one person with a history of asthma.
Physical examination and laboratory studies
All participants were seen in Xining before departure for a baseline survey that included physical examination and laboratory studies. AMS was assessed with the Lake Louise Scoring System (LLSS) (Roach et al., 1993). The LLSS is a 5-item self-administered questionnaire, which is based on the most frequent symptoms of AMS: headache, gastrointestinal events (anorexia, nausea, or vomiting), insomnia, weakness or fatigue, and dizziness or light-headedness. Every item is scored by the subject on a scale between 0 and 3, with each integer having a specific descriptor. The minimum score is 0, and the maximal score is 15. The score can be complemented by a question on the functional status of the subject (reduction in activity because of symptoms) and, if a knowledgeable person is present, by a standardized clinical assessment (change in mental status, ataxia, and peripheral edema). The clinical assessment was completed by physicians familiar with AMS and its assessment with the LLSS. Cumulative AMS scores were calculated as the sum of the self-, functional, and clinical scores. The presence of AMS was defined as presence of headache and a cumulative score ≥3. Severity of AMS was defined as follows: 0 to 2, no AMS; 3 to 4, mild AMS; 5 or more, severe AMS. Since our subjects had not yet spent the night at altitude when filling out the questionnaire in Xining prior to departure, the question on sleep was irrelevant; but since the subjects then spent the night on board the train, the remaining questionnaires took sleep into account. The LLSS was complemented with extra questions related to potential risk factors of AMS and preexisting medical conditions, such as a previous history of disease, previous exposure to altitude, exercise and physical activity habits, and alcohol and cigarette consumption.
Subsequently, the subjects underwent a physical examination. After 10 min of quiet rest in a supine position, resting pulse rate (PR) and arterial oxygen saturation (Sa
During the train journey to Lhasa, ECG, BP, PR, Sa
Altitude exposure
The journey from Xining to Golmud takes approximately 10 h (from 8:00
All train carriages are outfitted with oxygen supply from a molecular sieve system (West, 2008). Between Golmud and Lhasa, oxygen content in carriages is maintained at 23% to 24%, reducing the effective altitude by about 600 to 1000 m. Even though the windows are sealed, opening of doors at the intermediary railway stations inevitably leads to oxygen loss. In addition, at the higher altitudes the oxygen sieves are limited in their enrichment levels. Further limiting factors are the large number of passengers per carriage (ranging from 40 persons in soft sleeping carriages to 150 in seating carriages) and the subsequent large volumes of extra oxygen to be generated and ventilated.
Statistical analysis
We used 2 by 2 tables, odds ratios, χ2 tests, and Cornfield confidence limits for categorical data, where adequate. One-way analysis of variance (ANOVA) and Kruskal–Wallis tests were used for continuous or ordinal variables, respectively. Data are presented as the mean ± SD. p < 0.05 was considered significant.
Results
Incidence and severity of AMS
The three groups were not significantly different for age, sex, stature, and body mass or BMI (Table 1). There were no differences for any of the measurements between the two subgroups in the lowlander group (train travel from Beijing to Xining for 26 h, of which 2 h was above 2000 m vs. air travel for 2 h 10 min with a cruising cabin pressure equivalent to ∼2400 m), hence their grouped reporting. At baseline in Xining (2261 m), only 3 of the 160 (2%) Han lowlanders presented mild symptoms and reached the criterion score for AMS. On the first stretch from Xining to Golmud (between 2260 and 3700 m), 15 (6%) out of all 247 subjects presented symptoms, but only 6 (2%) had AMS. Further on, between Golmud and Lhasa, the lowest incidence of AMS (4%) was observed at the lowest site (Golmud, 2808 m). After passing Golmud, the train rapidly climbs up (within ∼1.5 h) from 2808 to 4768 m to the Mt. Kunlun Pass, with the oxygen-enriching system maintaining an oxygen concentration of 22% to 23%, equivalent to a decrease in altitude between 300 to 600 m, so the passengers were exposed to effective altitudes just above 4000 m. On this stretch, 187 of 247 passengers (76%) reported symptoms of AMS, while 62 (25%) reached the criterion score for AMS. After the Mt. Kunlun Pass, the train travels between 4500 and 4900 m for about 7 h to reach the highest point (Mt. Tanggula Pass, 5072 m), where AMS incidence reached 31%. The train then gradually descends to Yanbajiang at 4251 m over a period of ∼13 h, and incidence of AMS dropped to 28% (Fig. 2).
Incidence of AMS on the train along the points of measure during the journey.
Among the three passenger groups, Han lowlanders experienced the highest incidence of AMS at 31%, with a mean LLSS of 4.8 ± 0.44, range 3 to 8. Incidence was 16% in the Han altitude immigrants (score 3.8 ± 0.32, range 3 to 5), while there was no AMS in the Tibetan natives (score 0.38 ± 0.12, range 1 to 2). The incidence of AMS was significantly higher in the Han lowlanders than in the Han highlanders (χ2 = 5.18, p = 0.025). The severity of AMS (assessed by the mean AMS score) was also greater among Han lowlanders than Han immigrants (p < 0.05). However, of the 71 AMS subjects, most (60, 85%) appeared to have mild AMS and only 11 (15%) had more severe AMS.
No significant preventive effect of the use of Rhodiola was reported by 19 (7%) of subjects.
Symptoms and signs
On the Golmud–Kulum Pass section, the median time to the onset of symptoms was 2±0.5 h, with an earliest onset of symptoms within the first hour after the train ascended above 3500 m in 7 individuals. Headache was the most frequent (82%) and sometimes only symptom (20 subjects, 7%, of which 5 had a headache score of 3). Nausea (29%) was also a frequent symptom, in 4% accompanied by vomiting; 16% were short of breath. Five persons developed facial edema; feet and ankle edema was found in 12 subjects, both of which might have been influenced by prolonged time spent sitting. Frequency of symptoms and signs in the 71 cases of AMS are given in Table 2. Overall, 66 subjects of the 247 passengers (23%) developed three or more of symptoms with headache and a score ≥3, thus fulfilling the diagnostic criteria for AMS. One hundred seventy-seven of 284 (62%) had one or two symptoms or signs, even if most of them (172, 61%) did not reach the AMS criterion score, except for the 5 persons who had only a severe headache. Nobody had crackles or rales over the lungs. Nobody developed high altitude pulmonary edema (HAPE) or high altitude cerebral edema (HACE). One 52-yr-old male reported severe headache with ataxia and difficulty maintaining balance when walking in the passageway. He was put on oxygen, which quickly alleviated his symptoms. Upon arrival in Lhasa, he was hospitalized. A chest X ray showed clear lung fields, and a CT scan showed no signs of cerebral edema. After 1 day of observation in hospital, being treated intermittently with oxygen, he was discharged and joined a touring party to visit Lhasa without any further medical problems.
Risk factors
Sex
Women were slightly more affected by AMS than men. Excluding the Tibetans, 30 of 87 (34%) females had AMS compared with 30 of 135 (22%) males (χ2 = 5.82, p < 0.0025).
Age
Mean age of the 71 subjects with AMS was 43.5 ± 13.5 yr compared with 37.8 ± 12.7 yr for that of the 213 subjects without AMS (p < 0.01). In 131 passengers under the age of 40, 24 had AMS, whereas among 153 individuals aged more than 40 yr, 47 had AMS (18% vs. 31%, χ2 = 5.79, p < 0.025). Of the elderly group, 12 people with AMS were older than 60, of which 3 were older than 70 yr.
Acclimatization
Mean AMS case rates for the Han lowlanders and for the Han immigrants were significantly different. Fifty of the 160 Han lowlanders had AMS (31%), whereas only 10 of the 62 Han immigrants living at moderate altitudes between 2200 and 2500 m had AMS (16%). Han lowlanders were thus significantly more susceptible to AMS than altitude-acclimatized Han (odds ratio, OR 3.12; confidence interval, CI 1.24 to 8.86; p < 0.01). Of the 25 native Tibetans normally living above 3500 m, 6 persons developed one or two symptoms, but none met the diagnostic criteria of AMS. The difference in AMS rates in these three populations was statistically significant (χ2 = 35.96, p < 0.001) (Fig. 3).

Pulse rate and blood pressure
Resting pulse rate was lowest in Xining and increased with altitude A higher resting pulse rate increased the odds for AMS (OR 1.5, CI 1.1 to 2.1, p < 0.05), and higher pulse rates were correlated to more severe AMS symptoms (r2 = 0.21, p < 0.01) (Fig. 4).
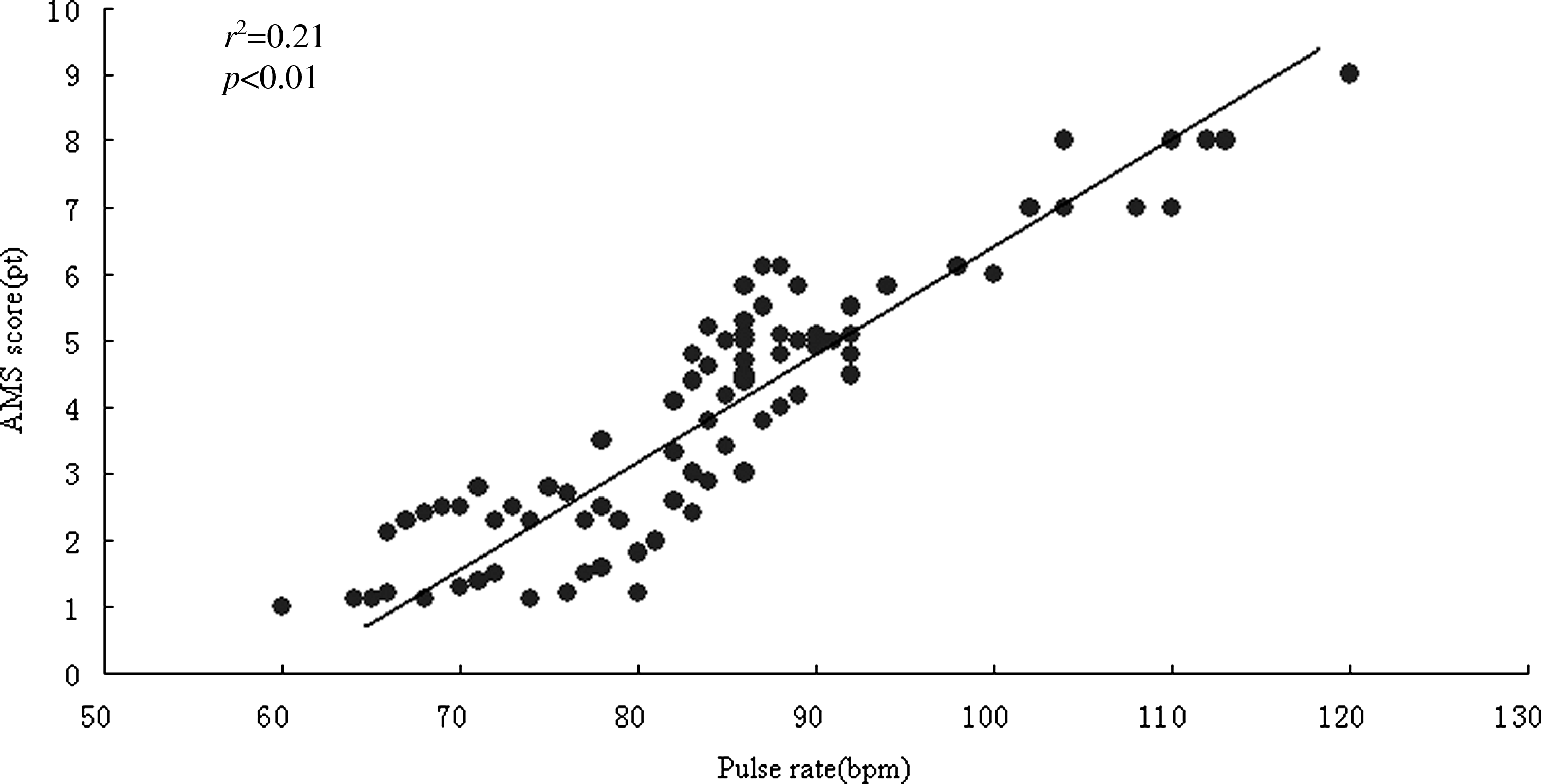
Relationship between pulse rate and LLSS AMS score at the different points of assessment during the train journey.
Before departure from Xining, systolic (SBP) and diastolic blood pressure (DBP) were normal in most subjects. There was a moderate increase in SBP upon arrival in Golmud. While the train ascended to an altitude between 4768 and 4905 m, BP increased in 43 of 176 (24%) subjects without AMS. Mean resting SBP rose from 122 ± 14 mmHg to 146 ± 16 mmHg, and mean diastolic pressure rose from 728 mmHg to 92 ± 12 mmHg (p < 0.05). Passengers who developed AMS had higher BP than subjects who did not develop AMS (mean SBP 142 ± 14 mmHg vs.126 ± 12 mmHg, p < 0. 05; mean DBP 96 ± 10 mmHg vs. 78 ± 6 mmHg, p < 0.025), but there was no correlation between the changes in BP and AMS scores. Figure 5A and B illustrates the changes of systolic and diastolic blood pressure during the train journey in passengers with and without AMS.

Systemic arterial pressure was higher in subjects older than 40 yr compared with those younger than 40 yr (mean SBP 144 ± 14 mmHg vs. 122 ± 12 mmHg; mean DBP 86 ± 10 mmHg vs.74 ± 8 mmHg, both p < 0.05).
Oxygen saturation
Oxygen saturation decreased with increasing altitude (Fig. 6). At altitudes between 4768 and 5072 m, in 176 passengers without AMS, mean Sa

Comparison of oxygen saturation between subjects with (n = 71) and without AMS (n = 176). Oxygen saturation decreased with increasing altitude by train ascent in both groups, but desaturation in subjects with AMS was more pronounced than in the normal persons (*p < 0.05). NS, not significant.
In the 71 passengers who developed AMS, mean Sa
Smoking is not allowed on the QTR. The 32 smokers, who only smoked at the railway stations when the train stopped, had no more symptoms of AMS than nonsmokers and had similar Sa
Electrocardiogram
Before departure from Xining, 23 persons (8%) had abnormal resting ECGs. On the train, cardiac rhythm abnormalities were not uncommon, especially in the elderly passengers at altitudes above 4000 m, but there was no statistically significant difference between the normal younger and older age group (Table 3). Han low-altitude subjects presented abnormal resting ECGs (27/160 or 17%), which tended to be more than in the 9/87 (10%) in the highlanders (χ2 = 1.93, p > 0.05). There was no difference in the prevalence of arrhythmia between AMS subjects and non-AMS subjects (14% vs. 12%, χ2 = 0.17, p > 0.05).
A–V = Atrioventricular heart block; BBB = bundle branch block.
Sinus arrhythmia and sinus bradycardia were frequently seen in healthy young adults, while sinus tachycardia was more common in the elderly. Atrial extrasystoles occurred in three symptom-free individuals and in two subjects with AMS. Ventricular extrasystoles occurred in one drunken person. S-T segment depression (≥0.5 mm) was more common in the elderly subjects (6/99, 6%) than in the younger (2/88, 2%). All except 2 of the 176 subjects for whom an ECG was obtained on the train did not show any evidence of cardiac ischemia on their ECG.
Follow-up in Lhasa
Two days after arrival in Lhasa (3658 m), 34 (52%) of the 65 subjects who had AMS on the train still had AMS symptoms, but the majority had sufficiently improved to join a touring party. Just two subjects were confined to bed rest; they were intermittently treated with oxygen and recovered slowly. All subjects were advised to refrain from exertion during the first 2 days in Lhasa. Mild AMS did not interfere with normal activity, and symptoms had subsided within 2 days.
Discussion
Boarding a train on the QTR is like entering a moving hypobaric chamber. Its variable barometric pressure obviously depends on the altitude reached, and passengers are exposed to a nonsteady state since ascent alternates with descent, depending on local geography. The speed of ascent is imposed, and train passengers are physically inactive. In addition, the increase in oxygen to 23% to 24% on the higher stretches partially attenuates the effect of actual altitude, limiting the exposure to an equivalent never exceeding ∼4000 m while traveling. This ensemble thus presents a different pattern of altitude exposure compared with that for mountaineers or trekkers, who can limit their speed of ascent and who are physically active. If the former decreases risk for altitude illness, the latter may increase it (Roach et al., 2000). On the other hand, sleep medication, alcohol, prolonged immobility, and sleep may lead to relative hypoventilation, potentially exacerbating hypoxemia on the train. Train travel to Lhasa thus represents a unique type of hypoxia exposure for which the subjects are physically inactive and the imposed rate of exposure is very high.
Incidence and severity of AMS
The incidence of AMS increased with speed of ascent and with altitude reached. It was 4% at 2808 m, 24% at 4768 m, and 31% at 5072 m. AMS can occur in some people at as low as 2500 m, but serious symptoms usually do not occur until over 3500 m. Even then it is not just the actual altitude reached that is important, but rather the speed of ascent. Speed of ascent on the QTR is rather high, reaching 1300 m/h while traveling from Golmud (2808 m) to the Mt. Kunlun Pass (4768 m) within 1.5 h. It is thus not surprising that 78% of the passengers developed mild symptoms and that 24% reached the LLSS criterion score of AMS ≥3. Rapid gain of altitude is well known from cable cars like the one joining the Venezuelan town Merida (1680 m) to a subsummit of Pico Bolivar at 4760 m in about 45 min. Most of those going up to the top already feel unwell upon arrival, and symptoms become worse with a prolonged stay (Hultgren, 1997). Rapid access by road is possible on Mauna Kea (4205 m), where it only takes 1.5 h to drive up to the summit, which leads to a majority (80%) of workers developing AMS during the first day at the research facility on top (Forster, 2000). But AMS also needs time to develop, and the rather modest incidence of AMS in our study suggests that for many subjects the duration of exposure to effective altitudes not higher than 4000 m while traveling on the QTR is short enough to prevent AMS from fully developing.
Symptoms
Headache was the most frequent symptom. Around 4905 m, 126 of 247 (51%) passengers had at least a score of 1 for headache, even though for many the total score remained below the criteria for AMS. During the follow-up in Lhasa, headache resolved spontaneously within a few days with acclimatization. There were no cases of HACE, although one subject with a strong headache and ataxia may have been a case of severe AMS evolving toward HACE. We also found no clear cases of HAPE, which probably is owing to the fact that exposure was short; HAPE usually requires about 48 h to develop.
Risk factors
Age
Several studies have suggested that the young are at greater risk for AMS (Hackett et al., 1976; Roach et al., 1995; Gaillard et al., 2004). Honigman and colleagues (1993) reported that subjects over the age of 60 have a lower incidence of AMS than persons below 40 yr. In our study, the group above 40 yr had an incidence of AMS of 31%, which was significantly higher than the 18% in the group below 40 yr. Two potential explanations can be proposed for this discrepancy. First, in studies on mountaineers and trekkers, physical exertion is an important contributing cause of AMS (Hackett et al., 1976; Roach et al., 2000), whereas in our study the subjects were physically inactive. Second, in our cohort the older passengers were generally in a rather unconditioned state resulting from a sedentary life-style (Maggiorini et al., 1990).
Sex
Whether sex is a relevant risk factor for AMS remains uncertain. In most studies, the frequency of AMS is similar in men and women (Hackett et al., 1976; Maggiorini et al., 1990; Schneider et al., 2002; Gaillard et al., 2004). Only two studies found a difference, one in trekkers going over the Thorong Pass in Nepal (5400 m), with 69% of women having AMS versus 57% of men (Kayser, 1991), and another reporting higher incidence of AMS in women pilgrims trekking in Nepal at 4300 m (OD 3.15; 95% CI 1.62 to 6.12) and also a higher incidence of HACE (Basnyat et al., 2000). We found that more female passengers had AMS than males (36% vs. 22%, p < 0.025). But since all AMS scoring systems rely on subjective symptom-intensity reporting, it remains unclear if there is any actual difference in the pathophysiology, incidence, and severity of AMS between the sexes.
Acclimatization
Lowland Han had the highest incidence of AMS. Han living at moderate to high altitude had less AMS, whereas none of the native Tibetans experienced AMS. These observations are in agreement with the results of Honigman and colleagues (1993), who reported that Colorado altitude residents who go to higher altitude have less severe symptoms of AMS than those who come directly from sea level, and data from Schneider and colleagues (2002), who reported that prior acclimatization protects against AMS. It follows that advice to prospective train passengers should be adapted to their state of acclimatization.
Clinical assessment on the train
We used the LLSS questionnaire, which proved to be well adapted for the purpose of screening for AMS in train passengers. Apart from symptoms of AMS, we also screened pulse rate and oxygen saturation, which are correlated to AMS (Roach et al., 1998; O'Connor et al., 2004). We found that subjects with a higher pulse rate and a lower Sa
Health education and physical examination
To prevent health problems on the QTR, passengers should be made aware of the risks associated with rapid exposure to altitude. Those with preexisting health problems should realize that their condition may worsen and should consult their physician prior to travel. Such passengers should inform the train physician of their condition on boarding the train. As a result, guidelines for altitude train travel on the QTR have been drawn up by one of the authors and are made available to prospective passengers.
Gradual ascent
Rapid ascent is one of the principal risk factors for the development and severity of AMS. Its occurrence is inversely related to the time taken to acclimatize (Smart and Hunter, 1984). In trekkers going toward Everest base camp, AMS risk decreased by 19% for each additional day spent between the airstrip at Lukla (2804 m) and the place of survey at Pheriche (4243 m) (Basnyat et al., 1999). Rapid ascending by train on the QTR implies increased risk for AMS. As a general rule, it would be preferable to plan a staged gradual ascent, spending a few days at an intermediate altitude in Xining (2261 m) or Golmud (2808 m) to provide sufficient acclimatization. Even though AMS on the QTR is mostly moderate and self-limiting, ∼100 cases of HAPE and/or HACE were identified among the 6 million passengers on the QTR during the last 3 yr. Recent observations (unpublished data) indicate that if passengers stay 1 to 2 days in Xining, travel on and again stay 1 to 2 days in Golmud, the incidence of AMS drops from 31% to 22%.
Pharmacological prevention
Interestingly, Chinese people going to high altitude traditionally use only Chinese or Tibetan herbs for prophylaxis against AMS and only rarely use acetazolamide or dexamethasone. We found that subjects who used Rhodiola were not protected from AMS. Since this use was not controlled and only concerned a small number of subjects, no conclusions can be made. The prophylactic use of acetazolamide to prevent AMS may be of use for sensitive subjects and should perhaps be proposed to prospective passengers.
Conclusions
Passengers on the train from Xining to Lhasa are at risk for AMS, mostly of mild nature and not incapacitating for most. Nevertheless, caution is warranted since altitude-sensitive subjects, older subjects, and those with preexisting disease are at risk for health problems that are potentially life threatening.
Because the number of passengers traveling by rail to Qinghai–Tibet is increasing (from July 1, 2006, up to July 1, 2009, the train transported ∼6.0 million passengers to Lhasa), AMS represents a sizable public health problem. Well-trained medical personnel on board, improved oxygen supply systems, and information campaigns for prospective travelers are necessary to control this health risk.
Footnotes
Acknowledgments
We are much obliged to Dr. John West for giving us important and instructive suggestions on high altitude problems connected with the QTR. We also thank all the workers and the train crew of the first train (Qing-1), the 27 Beijing–Lhasa, the 178 Xining–Lhasa, and the 907 Golmud–Lhasa, for their assistance in collecting the data.
Disclosure
The authors have no conflicts of interest of financial ties to disclose.