
Abstract
Abstract
Karinen, Heikki, Juha E. Peltonen, Mika Kähönen, and Heikki O. Tikkanen. Prediction of acute mountain sickness by monitoring arterial saturation during ascent. High Alt. Med. Biol. 11:325–332, 2010.—Acute mountain sickness (AMS) is a common problem while ascending at high altitude. AMS may progress rapidly to fatal results if the acclimatization process fails or symptoms are neglected and the ascent continues. Extensively reduced arterial oxygen saturation at rest (R-Sp
Introduction
Many researchers have looked for ways to predict AMS. Low hypoxic ventilatory response (HVR) has been proposed as a marker of susceptibility to AMS (King and Robinson, 1972; Moore et al.,1986), but some field studies have found no connection between HVR and AMS (Sutton et al., 1976; Hohenhaus et al., 1995; Bärtsch et al., 2002). Very high HVR has been reported in successful climbers at extreme altitudes (West, 2000), but high HVR is not necessary for successful climbing after acclimatization to extreme altitudes (Bernardi et al., 2006). In addition, low end-expiratory P
There is a need for a noninvasive, specific, and simple enough method for the evaluation of inadequate acclimatization and impending AMS in field conditions. Thus, the aims of the present study were (1) to investigate if postexercise oxygen saturation (Ex-Sp
Methods
Location
The study was conducted in 2001–2009 during eight expeditions to Denali (Denali 1, Denali 2, Alaska), Shisha Pangma (Tibet), Ulugh Muztagh (Tibet), and Island Peak and Mount Everest Base Camp (Nepal). We predicted AMS during ascent at altitudes of 2400 to 5300 m, which were considered critical altitudes for acclimatization during ascent.
Subjects
A total of 83 ascents made by 74 (64 men, 10 women) different climbers were evaluated. Only healthy, nonsmoking climbers participated in this survey. Their mean (SD) age during the ascents was 35 ± 9 yr, and maximal oxygen uptake was
Measurements at sea level
Before the expeditions, all members were examined by a physician, and only healthy subjects were selected for the study. All subjects performed a graded clinical exercise test on a cycle ergometer (Ergoline 800S, Ergoline GmbH, Bitz, Germany). They started cycling at 20 W, and the work rate was increased stepwise 20 W/min up to volitional fatigue. During the exercise test, a 12-lead electrocardiogram (ECG) was obtained, and alveolar gas exchange was measured breath by breath by a mass spectrometer (AMIS 2000, Innovision, Odense, Denmark) and a volume turbine (Triple V, Jaeger, Mijnhardt, Bunnik, The Netherlands). Arterial saturation was recorded by pulse oximetry from the fingertip (Nonin 8600, Nonin Medical, Inc., Plymouth, MN, USA). The details of participants and ascent for each expedition are presented in Table 1.
Values for age and
Measurements during ascent
Adaptation of the climbers to altitude was evaluated by measuring HR and Sp
p < 0.05, *p < 0.01.
One researcher took all the measurements and AMS scoring by interviewing subjects and looking for clinical signs. When the Denali 1 and Denali 2 groups were at different camps, a trained medical advisor took the measurements and AMS scoring. During all expeditions, HR, R-Sp
Symptom score
The Lake Louise Self-Report Score (LLS) was used for diagnosis of AMS (Hackett and Oelz, 1992). AMS was diagnosed according to a recent gain in altitude, the presence of headaches, and at least one of the following symptoms: gastrointestinal (GI) upset, fatigue, dizziness, or insomnia. The symptoms were graded from 0 to 4, with 0 meaning no symptoms at all and 1 to 4 meaning mild, moderate, severe, and extremely severe symptoms, respectively. A 3-point sum of symptoms or above indicated the presence of AMS. One aim of the study was to generate a tool for nonmedical persons in field conditions to estimate the risk for AMS. We chose to use an LLS score of 3 or more for the diagnosis of AMS, even though this cut point may result in too many climbers being pronounced at risk, but who did not subsequently develop AMS. At high altitude, the consequences of false positives are still minor.
Data analysis
Each data form was reviewed by the principal investigator for completeness. Differences in R-Sp
Results
LLS scores
There were no AMS (LLS ≥3) cases at altitudes of 2400 or 3000 m. Prevalence of AMS at an altitude of 3500 m was 10% (8 of 83 subjects); at 4300 m, 21% (17 of 83 subjects); and at 5300 m, 37% (27 of 73 subjects). The total prevalence of AMS at altitudes 2400 to 5300 m was 47% (39 of 83 subjects) in the whole study group. Ten climbers had AMS at two altitudes and 2, at three altitudes. In detail, in the Denali 1 and 2 groups (AMS in 20 of 31 subjects), 3 climbers had moderate AMS (LLS 6 to 7), required assistance with descent, and were evacuated (2 subjects from 4300 m and 1 from 5300 m). In the Shisha group, 5 of 6 climbers suffered mild AMS (LLS 4 to 5), but they continued climbing after 2 days' rest. In the Ulugh group (AMS in 6 of 10 subjects), 5 had mild AMS and 1 had severe AMS with ataxia (LLS 8) at 5300 m. The subject with severe AMS had to be evacuated with the assistance of a doctor. Trekking groups at Island Peak and Mount Everest Base Camp had three mild AMS cases at 4300 m and seven at 5300 m (10 of 36 subjects).
Aerobic capacity, BMI, heart rate, and arterial O2 saturation responses
In this study, subjects with AMS had better aerobic capacity (
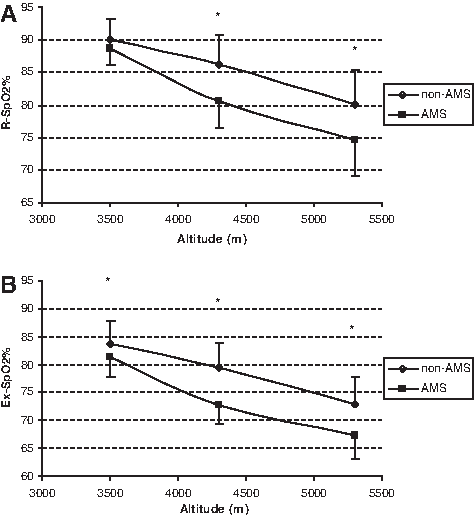
Arterial O2 saturation at rest and during exertion for climbers with no AMS and those experiencing AMS at that altitude is presented in Fig. 1. AMS scores (LLS) at different altitudes and Spearman's correlation coefficients between HR, R-Sp
Oxygen saturation (mean, SD) at different altitudes (
Prediction of AMS by arterial O2 saturation and heart rate measurements
We had no AMS cases at the altitude of 3000 m or below. The climbers experiencing AMS at 3500 m (n = 8) had higher HR at rest at 3000-m altitude than the non-AMS group (n = 75) (82 ± 11 vs. 74 ± 10, p < 0.05). However, at 3000 m, arterial O2 saturation did not differ between the groups: R-Sp
At 3500 m, the difference between subjects subsequently suffering AMS at 4300 m (n = 17) and the non-AMS group (n = 66) was obvious: both R-Sp
The subjects who subsequently developed AMS at 5300 m (n = 27) had lower R-Sp
The potential of screening for AMS by measuring R-Sp
Sp

The difference between R-Sp
The first cut-off value is mean saturation of all climbers at that altitude and we have compared subjects with AMS at that altitude and subjects with no AMS. The second cut-off value is chosen so that all AMS patients are identified.
Discussion
The most important finding in the present study was that Sp
Arterial O2 saturation
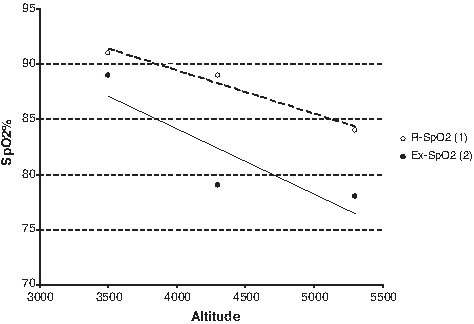
Arterial O2 varies over a range in normal individuals at a given altitude. It is usually lower on first arrival at a given altitude and rises somewhat with acclimatization (Mason et al., 2000; Botella de Maglia and Compte Torrero, 2005; Compte-Torrero et al., 2005). The predictive value of Sp
In our study we found a correlation between Sp2 and AMS. The correlation was significantly higher between Ex-Sp
The current recommendations are to ascend only 300 to 600 m per day and to take an acclimatization day for every 600- to 1200-m altitude gain (Hackett and Rabold, 2000; Basnyat and Murdoch, 2003; Gallagher and Hackett, 2004). Expeditions or individual climbers may ascend faster than the recommendations owing to the conditions of the route or climate. Our study tried to create a method for mountaineering expeditions to use saturation measurements at different altitudes to predict AMS if the ascent continues without extra acclimatization days. There was considerable variation in saturation levels; some climbers developed AMS and some did not at a given altitude. If we want to estimate a safe saturation level at different altitudes, the specificity of the mean saturation of the non-AMS group is not optimal. Because the variation among saturation levels is very large, it is difficult to estimate a 100% safe saturation level, and too many climbers will be classified into the AMS risk group (see Table 3). Thus, at saturation levels where sensitivity to AMS is 100%, the number of those who are declared to be at risk, but who do not subsequently develop AMS, is too high. However, this type of “safeline” approach provides an estimate of a safe saturation level during a 3500- to 5300-m expedition, which can help to identify a population that does well at altitude from those who may need an extra acclimatization day. Further, at high altitude the consequences of false positives are still minor. Those whose saturation levels are the lowest could be monitored more intensively, or an extra acclimatization day could be recommended. On the other hand, we had approximately equal numbers of false positives and correct predictions when taking the mean Ex-Sp
Obesity and heart rate
Obesity has been shown to be associated with the development of AMS, which may be partly related to greater nocturnal desaturation with altitude exposure (Ri-Li et al., 2003). In the present study, we found an association between BMI and weight and AMS (BMI and weight were higher in the AMS groups than in the non-AMS groups, p < 0.01), a finding that appears to be similar to the results reported earlier (Ri-Li et al., 2003). Elevated HR has also been shown to be associated with the presence of AMS (Maggiorini et al., 1990; O'Connor et al., 2004; Roach et al., 1995). The HR response seen in our study was similar to that found by O'Connor and colleagues (2004), but the correlation between elevated HR and AMS was weak. Thus, HR did not predict the future manifestation of AMS above 3000 m and therefore does not appear to be a useful tool in the prediction of AMS.
Study strengths and limitations
The strengths of the present study were that the rate of ascent, altitude of origin, and time of the day of testing could be controlled, because in each group every climber had a similar diet and physical background, and they climbed the same route on mountains over a restricted period of time with essentially the same snow and weather conditions. Barometric pressure varied from day to day, but during individual measurements it was stable. The limitations of our study include relatively few data points during varying degrees of acclimatization with different rates of ascent. As subjects who have experienced the symptoms of AMS presumably tend to participate in medical studies more eagerly than those without symptoms, this may lead to a slight overestimation of the prevalence of AMS. On the other hand, because no one wants to be the weakest link in the expedition, there could be a tendency to hide symptoms of AMS. There may have been some underestimation of symptoms because of group dynamics or the competitive spirit inside the groups. Also, it is possible to manipulate Sp
Conclusions and practical implications
The most important finding was that climbers who maintain their oxygen saturation at rest, especially with exercise, most likely do not develop AMS. The results suggest that daily evaluation of Sp
Footnotes
Disclosures
The authors have no conflicts of interest or financial ties to disclose.