
Abstract
Abstract
Baggish, Aaron L., Charles S. Fulco, Stephen Muza, Paul B. Rock, Beth Beidleman, Allen Cymerman, Kibar Yared, Peter Fagenholz, David Systrom, Malissa J. Wood, Arthur E. Weyman, Michael H. Picard, and N. Stuart Harris The impact of moderate altitude on pulmonary arterial hemodynamics after ascent to high altitude. High Alt. Med. Biol. 11:139–145, 2010.—Staged ascent (SA), temporary residence at moderate altitude en route to high altitude, reduces the incidence and severity of noncardiopulmonary altitude illness such as acute mountain sickness. To date, the impact of SA on pulmonary arterial pressure (PAP) is unknown. We tested the hypothesis that SA would attenuate the PAP increase that occurs during rapid, direct ascent (DA). Transthoracic echocardiography was used to estimate mean PAP in 10 healthy males at sea level (SL, PB ≈ 760 torr), after DA to simulated high altitude (hypobaric chamber, PB ≈ 460 torr), and at 2 times points (90 min and 4 days) during exposure to terrestrial high altitude (PB ≈ 460 torr) after SA (7 days, moderate altitude, PB ≈ 548 torr). Alveolar oxygen pressure (P
Introduction
The PAP responses to rapid and more gradual high altitude ascent have been characterized (Kronenberg et al., 1971; Groves et al., 1987; Allemann et al., 2004; Ghofrani et al., 2004). Comparison of data from prior studies suggests that the rate of ascent may be an important determinant of the magnitude of PAP increase for any given target altitude. Specifically, gradual ascent appears to be associated with lower PAP than does rapid ascent, but to date this observation has not been tested in a controlled fashion.
Staged ascent (SA), defined as temporary residence at moderate altitude (1400 to 2400 m) prior to high altitude ascent, is a common strategy employed by recreational and occupational travelers. Although SA has been shown to promote ventilatory acclimatization (Beidleman et al., 2009) and to decrease the incidence of noncardiopulmonary altitude-related illnesses (Evans et al., 1976), its impact on pulmonary arterial hemodynamics is uncertain. We hypothesized that SA would reduce the magnitude of PAP increase associated with ascent from sea level to high altitude. To test this hypothesis, we performed echocardiographic assessment of PAP in the same healthy lowlanders at sea level (SL), after rapid, direct simulated ascent (DA), and again after staged ascent (SA) to terrestrial high altitude.
Materials and Methods
This study used a sequential design in which an echocardiogram and resting oxygenation measurements were obtained from each participant at SL after DA to a simulated altitude of 4056 m in a hypobaric chamber * and again at two time points at 4300-m terrestrial altitude after SA.
Study design
This study was conducted in tandem with a research project directed by the U.S. Army Research Institute of Environmental Medicine (USARIEM, Natick, MA) where participants were first studied at SL (elevation ≈ 10 m, PB ≈ 760 torr, P
Participants
Ten healthy young-adult, active-duty military males gave voluntary and informed consent to participate in this study. The study was approved by the Institutional Review Boards of USAR IEM in Natick, Massachusetts, and Partners Healthcare in Boston, Massachusetts. Investigators adhered to the policies for protection of human subjects as prescribed in Army Regulation 70-25, and the research was conducted in adherence with the provisions of 32 CFR Part 219. Participants were born at altitudes below 1830 m and had a mean (±SD) age of 20 ± 2 yr, height of 176 ± 8 cm, and weight of 78 ± 13 kg. Mean calculated body mass index and body surface area were 25 ± 4 kg/m2 and 1.9 ± 0.2 m2, respectively. All participants had normal baseline vital signs (systolic blood pressure = 121 ± 10 mmHg, diastolic blood pressure = 79 ± 7 mmHg, heart rate = 69 ± 5 bpm), had no history of cardiovascular disease, and were not receiving antihypertensive medication. None of the participants had any contraindication to altitude exposure or to the study procedures.
Assessment of pulmonary arterial hemodynamics
Echocardiographic data were obtained using a commercially available system (Vivid-I, GE Healthcare, Milwaukee, WI, USA) with a 1.9- to 3.8-mHz phased-array transducer. Images were obtained after 10 min of quiet rest by a single trained observer. Two-dimensional (2-D) and Doppler imaging was performed from standard parasternal and apical transducer positions. All data were stored digitally, and poststudy data analysis (EchoPac, Version 6.5, GE Healthcare, Wauwatosa, WI, USA) was performed independently by two study cardiologists (ALB, KY) blinded to the time and conditions under which data were obtained.
PAP was assessed by two methods. First, continuous-wave Doppler imaging was used to measure the peak velocity of the tricuspid regurgitant jet, and the modified Bernoulli equation was used to calculate peak systolic right ventricular to right atrial (RV/RA) pressure gradient, a well-documented surrogate of peak pulmonary artery pressure both at sea level (Berger et al., 1985; Currie et al., 1985) and high altitude (Allemann et al., 2000). Second, pulsed-wave Doppler imaging of pulmonary arterial blood flow, recorded from the parasternal short axis view, was used to measure right ventricular pre-ejection time (PET), right ventricular ejection time (ET), and pulmonary artery acceleration time (AT). Mean PAP was calculated using the method described by Kitabatake and colleagues (1983), utilizing the ratio of pulmonary AT to right ventricular ET.
Pulsed-wave Doppler imaging of pulmonary arterial blood flow was also utilized to estimate stroke volume (SV). Specifically, the pulmonary artery velocity time integral was multiplied by the pulmonary arterial cross-sectional area to determine SV. Cardiac output was calculated as the product of SV and (heart rate (HR). Finally, the presence of patent foramen ovale was assessed by pulsed-wave and 2-D color Doppler imaging of the interatrial septum from the subcostal view.
Assessment of oxygenation
The primary indexes of oxygenation in this study were alveolar oxygen pressure (P
Arterial oxygen saturation (Sa
Statistical analysis
Measurements are presented as mean ± SD. Comparison of data across experimental conditions (SL, DA, SA) was performed using repeated measures ANOVA. Post-ANOVA paired t-testing with Bonferroni correction was used for between-study-condition comparisons. Correlation analysis was performed using the Spearman and Pearson methods as appropriate for data distribution. Data analysis was performed using SPSS (Version 16.0, SPSS Inc., Chicago, IL), and significance was set at p < 0.05 for all calculations.
Measurement variability
Interobserver variability for pulmonary arterial hemodynamic measurements was examined. Measurements were performed in a group of 5 randomly selected subjects at each of the 4 study time points (20 total measurements) by two investigators who were blinded to each other's measurements and to the study time point. Correlation coefficients for each measurement, derived from simple linear regression, were used to quantify interobserver variability and were as follows: right ventricular PET = 0.938, right ventricular ET = 0.878, pulmonary artery AT = 0.943, and peak systolic RV/RA pressure gradient = 0.951.
Results
Estimation of pulmonary arterial pressure
Tricuspid regurgitation was sufficient for the determination of peak systolic RV/RA pressure gradient in 6 of 10 participants at SL, 8 of 10 participants after DA, and 8 of 10 participants after SA (both at SA90min and SA4days). In contrast, pulmonary arterial pulsed-wave Doppler images, and thus estimates of mean PAP, were successfully obtained in all participants at each study time point. For the 30 total study time points (6 at SL, 8 at DA, 8 at SA90min, and 8 at SA4days) at which both peak systolic RV/RA pressure gradient and pulmonary arterial-flow-derived estimated mean PAP were available, a strong direct correlation between these measurements was observed (r2 = 0.94, p < 0.001). Because tricuspid regurgitation was insufficient for determination of RV/RA gradient in 4 of 10 subjects for at least one study time point, estimated mean PAP, as derived from the pulsed-wave Doppler pulmonary arterial flow profile, was used for the comparison of PAP across study time points in subsequent analyses. Pulmonary artery hemodynamic measurements associated with each study condition are shown in Table 1.
Sea level (SL), after direct ascent (DA), and after staged ascent (SA). PET, right ventricular pre-ejection time; ET, right ventricular ejection time; AT, pulmonary arterial acceleration time; RV/RA, right ventricular to right atrial; PAP, pulmonary arterial pressure; NS, not significant.
p-value for repeated measures ANOVA.
p < 0.05 compared to SL.
p < 0.05 compared to DA.
Incomplete data were available at each study point as described in text.
Sea level
Resting gas exchange values (P
Direct ascent to high altitude: DA vs. SL
Resting HR increased (DA = 77 ± 7 bpm vs. SL = 69 ± 5 bpm, p < 0.001); stroke volume and cardiac output increased, whereas systolic and diastolic blood pressures were not significantly changed. Both P

Staged ascent to high altitude: SA90min vs. SL
Heart rate increased (SA90min = 73 ± 6 bpm vs. SL = 69 ± 5 bpm, p = 0.02) significantly, whereas stroke volume, cardiac output, and systolic and diastolic blood pressures were not significantly changed. Both Sa
Impact of staging on high altitude ascent: DA vs. SA90min
When compared to SL values, high altitude ascent resulted in changes in vital signs, oxygenation, and pulmonary arterial hemodynamics after both DA and SA90min. However, the magnitudes of change among these parameters differed significantly between the two altitude ascent conditions. When compared with DA, SA90min was associated with lower heart rate (SA = 73 ± 6 bpm vs. DA = 77 ± 7 bpm, p = 0.04), stroke volume, cardiac output, and improved oxygenation as measured by both Sa
Prolonged exposure after staged ascent: SA90min vs. SA4days
Heart rate, systolic blood pressure, diastolic blood pressure, Sa
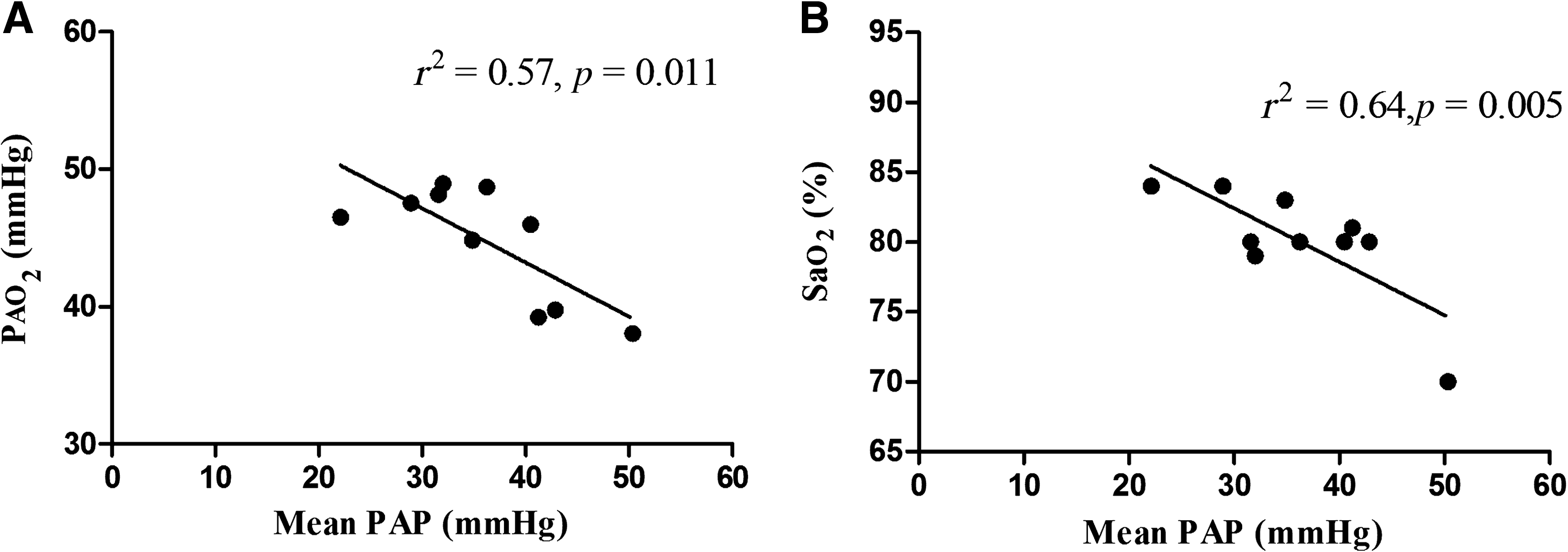
Relationship between mean pulmonary arterial pressure (PAP) and
Relationships between oxygenation and PAP: SL, DA, and SA
Given the assumed importance of hypoxia–hypoxemia in the pulmonary arterial response to high altitude, we examined the association between oxygenation (P
Discussion
The results of this study support the hypothesis that SA leads to a significant attenuation of the PAP increase after ascent to high altitude. This attenuated PAP increase was observed at 90 min and 4 days of high altitude exposure following SA. Further, it appears that SA results in an uncoupling of PAP from oxygenation as measured in both the alveoli (P
The magnitude of PAP increase in the current study is consistent or in excess of that in previous reports of the pulmonary arterial response to rapid DA. Kronenberg and colleagues (1971) performed pulmonary arterial catheterization on a small group of healthy, though older, male subjects (n = 4, age = 34 ± 4 yr) after airplane-facilitated ascent to a lower altitude of 12,470 ft (3800 m) and demonstrated a rise in mean PAP from a baseline of 10 ± 1 mmHg to 21 ± 4 mmHg at altitude. Similarly, Allemann and colleagues (2004) examined PAP among 41 individuals after rapid mixed-modality ascent (cable car and hiking) to 4559 m and documented mean rises in the RV/RA pressure gradient from 16 ± 7 mmHg to 44 ± 15 mmHg.
Data from studies utilizing gradual ascent to high altitude suggest that PAP may increase less than it does during DA (Groves et al., 1987; Ghofrani et al., 2004). Prior observations that the rapidity of ascent appears to dictate the magnitude of the PAP response led us to conduct the current study. SA differs importantly from gradual continuous ascent, and this difference has important practical implications for recreational and occupational high altitude travelers. However, gradual continuous ascent and SA share the common attribute of prolonged exposure to mild to moderate levels of hypoxia prior to the more severe hypoxia of high altitude.
Our data suggest that moderate altitude staging is associated with a marked reduction in the magnitude of PAP increase during subsequent high altitude ascent. This finding suggests that temporary exposure to moderate altitude has the capacity to blunt further hypoxic pulmonary vasoconstriction during subsequent high altitude exposure. The moderate negative correlations that we observed between PAP rise and both P
The physiologic explanations for our finding of attenuated PAP increase with SA are uncertain and constitute an important area for future work. There is mounting evidence that the smooth-muscle cells of the small- to medium-sized resistance arterioles are the key effectors of hypoxic pulmonary vasoconstriction. Specifically, it appears that hypoxia stimulates smooth- muscle cell mitochondrial production of reactive oxygen species that exhibit a paracrine effect on cellular proteins responsible for contraction (Post et al., 1992; Gelband and Gelband, 1997; Chandel et al., 2000; Michelakis et al., 2002). This response appears to be rapid with two distinct vasoconstrictor phases (Dorrington et al., 1997; Talbot et al., 2005). However, prior animal model work has begun to identify important modulatory processes that have the capacity to oppose hypoxic pulmonary vasoconstriction (Brashers et al., 1988; Le Cras et al., 1998; Muramatsu et al., 1999). At the present time, the temporal sequence and what determines the eventual balance between such opposing vasoactive factors are not known. Our findings may reflect the fact that mild persistent hypoxia encountered during the moderate-altitude period of SA has the capacity to upregulate compensatory vasodilatory factors and to thus reduce further vasoconstriction during increasing hypoxia.
Implications
The finding that SA attenuates PAP increase may have important implications for travelers to high altitude. High altitude pulmonary edema (HAPE) is an important cause of high altitude morbidity and mortality, and there is strong evidence that the development of HAPE is related to the magnitude of PAP rise during ascent (Maggiorini et al., 2001; Swenson et al., 2002). Consequently, current recommendations suggest gradual ascent as a means to prevent HAPE (Hackett and Roach, 2001). Findings from this study provide preliminary biological data that suggest that SA may be as effective as gradual ascent for this purpose. Confirmatory field work examining the impact of SA on PAP in HAPE-susceptible individuals is warranted.
Limitations and areas of future work
First, because we studied individuals without prior high altitude experience, we cannot make definitive conclusions about the effect of SA on individuals with known HAPE susceptibility. However, several of our subjects experienced a PAP response of similar magnitude to that reported among individuals with known HAPE susceptibility (Hohenhaus et al., 1995), and these vigorous PAP responders remained significantly sensitive to the effect of SA. Second, our findings do not explain how SA leads to an attenuation of PAP. Elucidating the physiologic mechanisms responsible for our findings is an important area for future work. Third, we studied relatively youthful people and thus our findings may not be applicable to older individuals. Fourth, PAP was estimated using noninvasive techniques that, when inaccurate, tend to underestimate true PAP values. So the true magnitude of the PAP rise associated with both ascent profiles may have been less than reflected in our data. Finally, the direct ascent in this study was conducted in a hypobaric chamber. We cannot exclude the fact that this experimental condition, perhaps due to the psychological stress associated with chamber decompression, contributed to the marked PAP rise that we observed.
Conclusions
Staging at moderate altitude reduces the magnitude of PAP increase associated with subsequent high altitude ascent. Thus this strategy may be an effective means to reduce the incidence of the adverse effects of acute pulmonary arterial hypertension that occur during high altitude ascent. In addition, our data suggest that SA may reduce the importance of hypoxia and hypoxemia as a determinant of PAP after high altitude ascent. Further work is justified to clarify the physiology of staging and to define its role for disease prevention and performance enhancement.
Footnotes
Disclosures
The authors have no conflicts of interest or financial ties to disclose.
Acknowledgments
The study was supported in part by a project grant from the Center for Integration of Medicine and Innovative Technology (CIMIT), Boston, Massachusetts, and funding provided by the U.S. Army Medical Research and Material Command ATO IV.MD.2006.01.
*
Although the actual terrestrial altitude at the summit of Pikes Peak is 4300 m, the average measured barometric pressure of ∼460 torr correlates with an altitude of 4056 m. The simulated altitudes of DA were adjusted to reflect this discrepancy.