
Abstract
Abstract
Stewart J. Jackson, James Varley, Claudia Sellers, Katherine Josephs, Lucy Codrington, Georgina Duke, Marina A. Njelekela Gordon Drummond, Andrew I. Sutherland, A. A. Roger Thompson, J. Kenneth Baillie. Incidence and predictors of acute mountain sickness among trekkers on Mount Kilimanjaro. High Alt. Med. Biol. 217–222, 2010—. We investigated the incidence of AMS amongst a general population of trekkers on Mount Kilimanjaro, using the Lake Louise consensus scoring system (LLS). Additionally we examined the effect of prophylactic acetazolamide and different ascent profiles.
Climbers on 3 different ascent itineraries were recruited. At 2743 m we recruited 177 participants (mean age 31, range [18-71]) who completed LLS together with an epidemiological questionnaire. At 4730m participants (n = 189, male = 108, female = 68, mean age 33, range [1871]) completed LLS, 136 of whom had been followed up from 2730 m.
At 2743 m, 3% (5/177) of climbers were AMS positive, and 47% (89/189) of climbers from all itineraries were AMS positive at 4730 m. Of climbers attempting the Marangu itineraries, 33% (45/136) were taking acetazolamide. This group had a similar rate of AMS and no statistical difference in severity of LLS when compared with those not taking prophylactic drugs. We also did not demonstrate a difference between the incidence of AMS in climbers who did or did not take a rest day at 3700 m. However, there was a significant reduction in the incidence of AMS amongst pre-acclimatized subjects.
Consistent with previous work, we found that the rate of AMS on Mount Kilimanjaro is high. Furthermore, at these fast ascent rates, there was no evidence of a protective effect of acetazolamide or a single rest day. There is a need to increase public awareness of the risks of altitude sickness and we advocate a pragmatic “golden rules” approach (http://www.altitude.org/altitude_sickness.php).
Introduction
Although the mechanisms of AMS are still a matter of active investigation, rapid ascent to altitude is a firmly established cause (Singh et al., 1969; Basnyat et al., 1999; Basnyat and Murdoch, 2003; Gallagher and Hackett, 2004). Mount Kilimanjaro combines easy access with a financial imperative to ascend quickly as the significant national park fees induce climbers to ascend at rates of more than one thousand vertical meters per day. At 5895 m, Kilimanjaro is the world's tallest free standing mountain. This provides less opportunity for climbers to acclimatize before arriving at the park entrance because, unlike other high altitude destinations, travel to the start of the climb usually involves no prior altitude exposure. The ascent of Mount Kilimanjaro is generally not considered difficult amongst travelers to Tanzania. In 2007, 41,760 climbers may have attempted the summit (Karinen et al., 2008). Climbers on Mount Kilimanjaro are often naive to the risks of altitude exposure, demonstrated by the fact that only 10% of climbers on the mountain have previous high-altitude experience (Kalson et al., 2009). This combination of large numbers of inexperienced climbers and rapid ascents has led to the need for emergency evacuation teams at camps along the mountain.
Climbers can take several routes to reach the summit of Mount Kilimanjaro. The Marangu route is considered the easiest, with ascent to the summit and back possible over 5 or 6 days. Climbers attempting this route stay in shelters each night, which are located at Mandara Huts (2743 m), Horombo Huts (3760 m) and Kibo Huts (4730 m). On the 6-day itinerary, an extra rest day is taken at Horombo Huts. The Rongai route is considered more challenging, with no fixed shelters and the summit attempt being made on the fifth day of climbing. Including return to the park entrance, the Rongai itinerary takes 6 days.
The aim of this study was to investigate and compare the incidence of AMS on three of the main ascent itineraries on Mount Kilimanjaro. In addition, this study aimed to assess the protective effect, if any, of a rest day at 3760m and prophylactic acetazolamide.
Materials and Methods
This cross-sectional study was approved by the Tanzanian National Institute for Medical Research, the Tanzanian Commission for Science and Technology (2009-175-NA-2009-36) and the Tanzanian National Parks Authority. Written informed consent was obtained from all volunteers recruited from the general population of trekkers ascending Mount Kilimanjaro. Exclusion criteria included non-English speakers, climbers aged under-18 and expedition employees.
Researchers recruited subjects at Mandara Huts (2743 m), and followed up subjects at Kibo Huts (4730 m). Researchers at Kibo Huts also recruited subjects attempting the Rongai route, and any subjects that had previously been missed at Mandara. Subjects from three itineraries were therefore recruited: those attempting the 5-day Marangu itinerary, the 6-day Marangu itinerary and the Rongai itinerary. Figure 1 shows the ascent profile of the different itineraries from the park entrance (night 0) until Kibo Huts.

Ascent profile from the park entrance to Kibo Huts on 3 different ascent itineraries on Mount Kilimanjaro. Data were obtained at 274m3 and 4730m.
Climbers agreeing to take part in the study were asked to complete a LLS self-report questionnaire in an isolated, quiet environment between 1 and 8 hours after arrival at camp. AMS was defined as a total score of 3 or more on the LLS, including the presence of a headache and at least one other symptom (Roach et al., 1993).
Subjects performing the 5-and-6-day Marangu itineraries also completed a short questionnaire concerning age, sex, co-morbidities, smoking status, medications and use of prophylactic acetazolamide. When climbers on the Marangu itineraries arrived at Kibo Huts, we asked whether they had undertaken the 5-or-6-day itinerary.
Statistical analysis
The AMS incidence on the different itineraries on Mount Kilimanjaro was compared using a Chi-squared test (Greenwood and Nikulin, 1996). A Chi-squared test was also use to analyze the efficacy of acetazolamide in preventing AMS, and Fisher's exact test to compare those who had undertaken an acclimatization trek against the remainder of the sample. The Mann-Whitney test was used to compare the severity of AMS between climbers who were or were not taking prophylactic acetazolamide (Armitage, 1971). Probabilities of p < 0.05 were considered statistically significant.
Results
We obtained data from 177 participants attempting the Marangu itineraries at 2730 m. Of these, 41 climbers were lost to follow-up (27 male, mean age 30, range [18 – 63]), 15 (37%) of whom were taking prophylactic acetazolamide. The characteristics of the 136 climbers attempting the Marangu itineraries who were successfully followed up from 2730 m are shown in Table 1. Comorbities were present in some of the climbers, the most common of which was asthma (5% of climbers).
In addition to the 136 participants followed up from 2730 m, we recruited another 13 subjects on the Marangu itineraries at the high camp at Kibo Huts. Of these 149 subjects at 4730 m, 82 (55%) climbers had chosen to take a rest day at 3760 m.
We recruited 40 climbers attempting the Rongai itinerary at Kibo huts, giving AMS data on a total of 189 subjects at 4730 m (Figure 2). The mean age of climbers at this altitude was 31, range [18 − 71] and 108 (57%) were male.
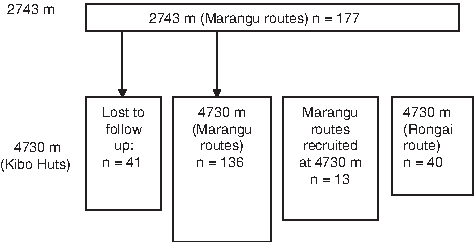
Schematic representation of subject recruitment on Mount Kilimanjaro
The incidence of AMS on Mount Kilimanjaro
At 2743 m 3% of the 177 climbers recruited at this altitude had AMS. Following headache, the commonest symptom reported on LLS sheets was fatigue (38%). At 4730 m, sleep disturbance was the commonest symptom described (82%). 47% of the 189 climbers on all itineraries were AMS positive.
Of all the climbers in the study at 4730m that were attempting the 5-day Marangu itinerary, 42% had AMS at 4730 m, while 46% of all climbers taking the 6-day Marangu itinerary had AMS at 4730 m. 48% of climbers attempting the Rongai itinerary were AMS positive at 4730 m (Table 2). No difference in the rate of AMS was found between climbers attempting any of the three itineraries.
LLS greater than 6 were recorded in 13 of the 189 (7%) subjects investigated at 4730 m. The highest LLS reported was 10. The scores at 4730 m are shown in Figure 3. Analysis of AMS incidence amongst the 136 climbers attempting the Marangu itineraries that were successfully followed up at 4730 m allowed analysis of the extent to which acetazolamide protects climbers from the development of AMS (Table 3). We did not find a significant difference in AMS incidence or severity between subjects taking acetazolamide and those who were not (acetazolamide: 42%; no treatment: 49%; p = 0.89). In addition, there was no significant difference in the severity of LLS in climbers taking prophylactic acetazolamide (median LLS (quartile range): acetazolamide: 3 (2, 4); no treatment: 3 (2, 5); p = 0.77). The distribution of LLS both in climbers taking prophylactic acetazolamide and those who were not is shown in Figure 4. Finally, of the 14 climbers that reported undertaking an acclimatization trek, 1 was AMS positive at 2743 m, while 2 were lost to follow up and a further 2 were AMS positive at 4730 m. Undertaking an acclimatization trek significantly reduced the risk of AMS development (p = 0.03, Fisher's exact test).

The distribution of LLS at 4730m.
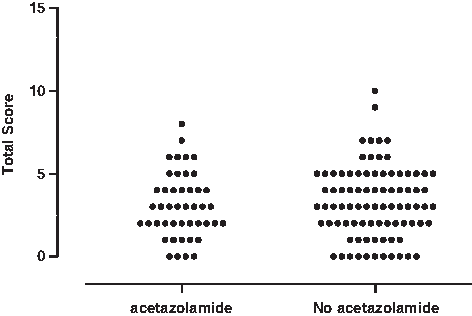
The effect of prophylactic acetazolamide on AMS severity, as scored by the LLS, at 4730 m.
AMS, acute mountain sickness.
Discussion
The incidence of AMS on Mount Kilimanjaro is important because it is one of the world's most popular climbing destinations and many climbers are exposed to risk. Although our results substantiate the findings of one study on Mount Kilimanjaro that reported an incidence of AMS of 41% (Kalson et al., 2009), another cohort study on the mountain found the incidence to be as high as 84% (Kayser et al., 2008). Our study confirms the very high rate of AMS on Kilimanjaro, and importantly found no evidence of protection from AMS among climbers taking prophylactic acetazolamide or taking a rest day during the ascent. Although this is an observational study, these results suggest that it would be unsafe for climbers to assume that either acetazolamide, or a single rest day, will confer protection from altitude illness in the context of an extremely rapid ascent. Our data demonstrates the significant protective effect of an acclimatization trek and supports current guidance (West et al., 2007).
Figure 1 shows that the ascent profiles of the 3 itineraries are similar but the Marangu 5-day itinerary is the fastest. Since rate of ascent affects risk of AMS (Singh et al., 1969; Basnyat et al., 1999; Basnyat et al., 2003; Gallagher and Hackett, 2004; Bloch et al., 2009), it is expected that climbers on this itinerary would have a greater incidence of AMS. Conversely, the Rongai itinerary has the most steady ascent profile. We found no difference in AMS incidence, which may indicate that, despite small differences in the ascent itineraries, the rate of ascent on any itinerary is sufficiently fast to cause AMS in a large proportion of climbers. Our study is consistent with the findings of the smaller study by Kalson et al, who found no protective effect of a rest day at 3760 m (Kalson et al., 2009). Although acetazolamide is known to mitigate symptoms of AMS, (Forwand et al., 1968; Birmingham Medical Research Expeditionary Society Mountain Sickness Study Group, 1981; Larsen et al., 1982; Dumont et al., 2003; Basnyat et al., 2003; Hillenbrand et al., 2006; van Patot et al., 2008), we found no evidence of protection from acetazolamide during the unusually rapid ascent rates on Kilimanjaro. A previous observational study on Mount Kilimanjaro also suggested this possibility (Karinen et al., 2008). Although performed with a smaller number of subjects, Kayser et al. also found that acetazolamide gave less protection from AMS than might be expected, with 50% of climbers taking acetazolamide developing AMS (Kayser et al., 2008). Davies et al. found that acetazolamide was protective against AMS amongst climbers attempting the 6-day Marangu itinerary, but not the more rapid 5-day itinerary (Davies et al., 2009). Some of the previous studies investigating the effect of acetazolamide used conservative ascent profiles. Subjects in the study by Basnyat et al. (2003) ascended at rates of approximately 500 m per day. Other studies allowed considerable time for acclimatization (Birmingham Medical Research Expeditionary Society Mountain Sickness Study Group, 1981), but few of the studies investigating the protective role of acetazolamide used such rapid ascent profiles as those found on Mount Kilimanjaro.
It is possible that the doses taken on the mountain are insufficient to prevent the development of AMS or that climbers on Mount Kilimanjaro exert themselves more than usual. Although this study lacks the statistical power to conclusively exclude a protective effect, it is important for climbers to be aware that AMS is common on standard itineraries, even among climbers taking acetazolamide.
A potentially important limitation of our study is that nearly 25% of subjects in our study who were recruited at Mandara Huts were lost at follow up. This could cause bias since the lost subjects could have been suffering from the most frequent or severe AMS. Importantly, a comparable proportion (37%) of the subjects who withdrew from the study were taking prophylactic acetazolamide.
Antimalarial drugs were taken by over 70% of climbers. Prophylactic regimens included doxycycline, mefloquine (larium), and proguanil with atovaquone (malarone). Side effects of such medications may include headache, nausea, somnolence, gastrointestinal disturbance and dizziness (British National Formulary, 2009). Thus, the common side effects of antimalarial medications may mimic the symptoms of AMS and could account for the high incidence of AMS found on Mount Kilimanjaro. In addition, mefloquine may reduce the efficacy of acetazolamide (Healthline.com/druginteractions).
Another potential problem with this study was that the rate at which each climber made their ascent between camps was uncontrolled. While some climbers spent the majority of the day making the ascent, others made the trip in a matter of hours and are hence at greater risk of developing AMS.
Although nearly 50% of the subjects in our study had AMS, we may have underestimated the incidence of AMS on the mountain. Firstly, as discussed above, a number of subjects were not followed up at 4730 m. Secondly, anecdotal reports of AMS en route to the summit from Kibo Huts were common, but these data were not included in this study. Thirdly, for practical reasons scores were only taken in the late afternoon and evening, and scores in the morning are known to be greater than the afternoon (Kayser et al., 2008). Indeed, a recent cohort study (Karinen et al., 2008) demonstrated that 75% of subjects developed AMS at some point during their time on the mountain.
Nearly 7% of subjects at 4730 m had a LLS ≥ 7, and one subject was found to have a total LLS of 10. These high scores indicate severe AMS and significant risk of complications. Disturbingly, we witnessed numerous climbers continuing to ascend despite severe symptoms of AMS. Previous studies have suggested that the incidence of HACE on Mount Kilimanjaro may be as high as 18% (Karinen et al., 2008), and a larger clinical assessment of HACE and HAPE presence on the mountain would be useful. Figure 3 shows that, although over half of climbers are not suffering from AMS, the vast majority do experience at least some symptoms, even if they are not severe enough to be classified as AMS-positive.
On Mount Kilimanjaro, and other mountains, the presence of AMS is not related to summit success (Pesce et al., 2005; Kalson et al., 2009). Tourists suffering from AMS on the mountain are likely to persevere with their summit attempt despite significant symptoms. However, climbers should be cautioned that ignoring the warning signs of AMS could lead to the possibility of developing HACE and HAPE on the mountain.
Current guidelines propose that at over 3000 m, each night should be spent not more than 300 m above the last, with a rest day every 2-3 days (West et al., 2007). This is so far removed from normal behavior among climbers on Kilimanjaro that we consider it an unrealistic aspiration. However, we believe that the incidence of AMS on Kilimanjaro, and the attendant risks of death from HAPE and HACE, are unacceptably high. Perhaps a more pragmatic emphasis on symptoms might be more popular with climbers, and hence have a better chance of modifying their behavior. The “golden rules” for climbers at high altitude proposed by Shlim and Dietz (2000) seem particularly apt:
If you feel unwell, it is altitude sickness until proven otherwise
Never ascend if you have symptoms of altitude sickness
If you are getting worse then descend immediately.
Better awareness of AMS in climbers can reduce the incidence of AMS (Gaillard et al., 2004). In addition, the benefits of acclimatization treks are well documented (Pesce et al., 2005); Mount Meru (4566 m) is located conveniently close to Mount Kilimanjaro. Climbers must not assume that acetazolamide, route or a single additional rest day can protect them from AMS during an extremely fast ascent. Advice is available from the International Mountaineering and Climbing Federation (www.theuiaa.org). A campaign to raise public awareness of the scale of the problem on Mount Kilimanjaro is overdue.
Footnotes
Acknowledgments
The project was funded by Chest Heart Stroke Scotland. We would like to acknowledge the assistance of the Tanzanian National Institute for Medical Research, the Tanzanian Commission for Science and Technology, the Tanzania Wildlife Research Institute and the Tanzanian National Parks Authority for support and advice.
Disclosures
Mr. Jackson, Mr. Varley, Ms. Sellers, Ms. Josephs, Ms. Codrington, and Drs. Duke, Njelekela, Drummond, Sutherland, Thompson, and Baillie have no conflicts of interest or financial ties to disclose.