
Abstract
Abstract
Elsensohn, Fidel, Inigo Soteras, Oliver Reisten, John Ellerton, Hermann Brugger, and Peter Paal. Equipment of medical backpacks in mountain rescue. High Alt. Med. Biol. 12:343–347.—We conducted a survey of equipment in medical backpacks for mountain rescuers and mountain emergency physicians. The aim was to investigate whether there are standards for medical equipment in mountain rescue organizations associated with the International Commission for Mountain Emergency Medicine (ICAR MEDCOM). A questionnaire was completed by 18 member organizations from 14 countries. Backpacks for first responders are well equipped to manage trauma, but deficiencies in equipment to treat medical emergencies were found. Paramedic and physicians' backpacks were well equipped to provide advanced life support and contained suitable drugs. We recommend that medical backpacks should be equipped in accordance with national laws, the medical emergencies in a given region, and take into account the climate, geography, medical training of rescuers, and funding of the organization. Automated external defibrillator provision should be improved. The effects of temperature on the drugs and equipment should be considered. Standards for training in the use and maintenance of medical tools should be enforced. First responders and physicians should only use familiar tools and drugs.
Introduction
Aims and Methods
A standardized questionnaire was distributed and collected in 2006 among ICAR MEDCOM representatives. This study analyzed only the contents of medical backpacks and did not ask how frequently technical and medical devices are used. The results and recommendations were discussed among the authors, and presented at the ICAR MEDCOM meetings in Chamonix, France, in October 2008 and in Bansko, Bulgaria, in March 2009. Finally, the ICAR MEDCOM approved the recommendations in Zermatt 2009. Nominal data are given as counts (percentages). Figures were arranged with Excel 2008 (Microsoft, Seattle, WA).
Results
Eighteen mountain rescue organizations from 14 countries in North America and Europe returned the questionnaire (Table 1). Sixteen organizations provide a special medical backpack for mountain rescuers who are acting as first responders, whilst all 18 organizations provide a special medical backpack for mountain rescue physicians. The contents of the mountain rescuers' medical backpacks are shown in Figure 1. Eight of 16 (50%) backpacks are equipped with oral nitroglycerin, five (33%) contain oral analgesics, but seven (43%) backpacks contain no drugs. Medical equipment in medical backpacks of mountain rescuers is defined by law in two (12%), by internal or national standards in 10 (63%), and by no specific standards in four (25%) organizations.
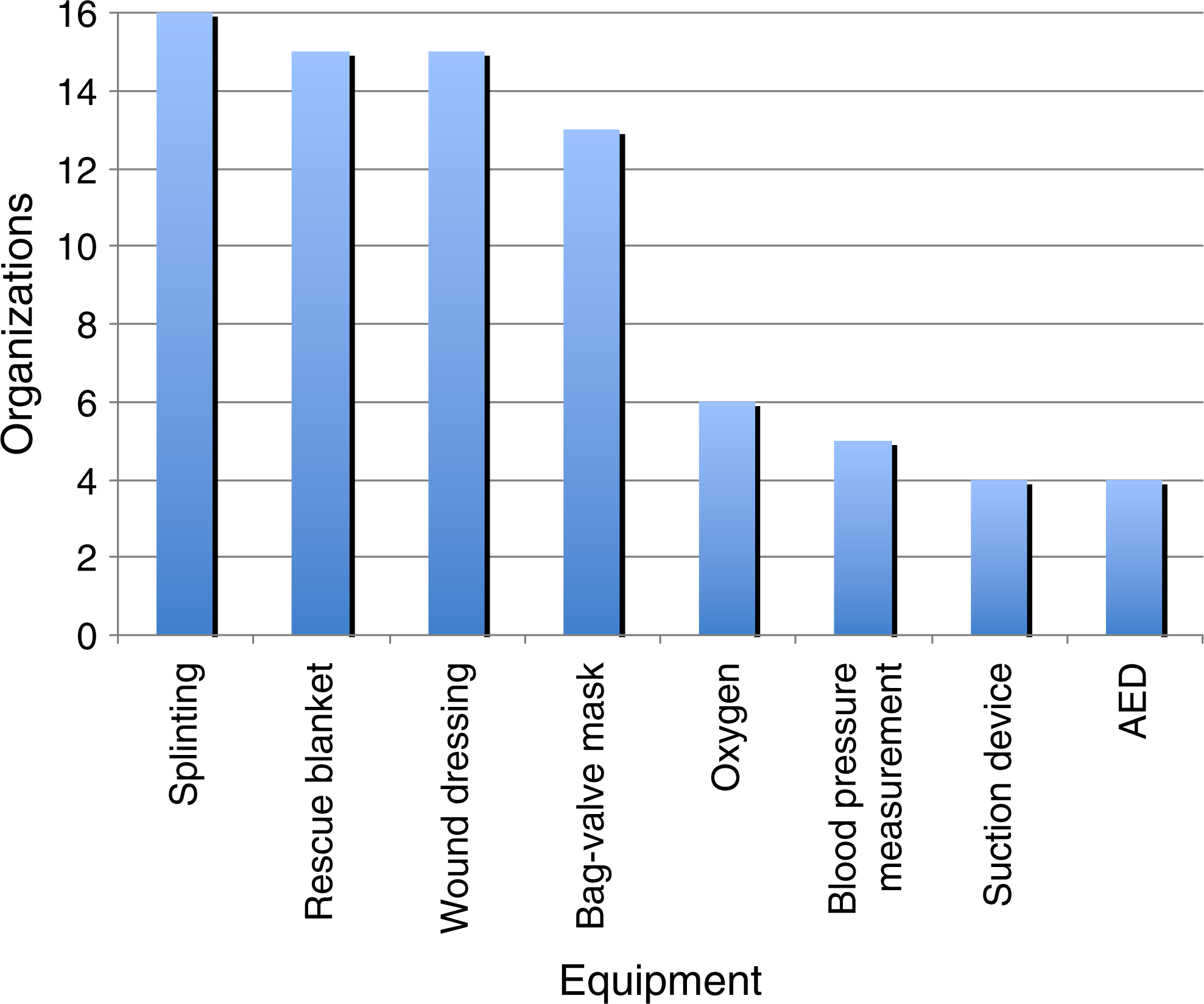
Medical equipment of first responders' backpacks (organizations n=16; chart limited to equipment with >1 item).
The contents of the mountain rescue physicians' medical backpacks are shown in Figures 2 and 3. Their content is defined by law in three of 18 (17%), by internal standards in 13 (72%), and by no specific standards in two (11%) organizations. These backpacks always stay with the mountain rescue physician in 12 (67%) organizations, whilst in the remaining six (33%) organizations the backpack is brought to the scene independently of the mountain rescue physician, just in case another physician reaches the scene first. Drugs are provided and maintained by the mountain rescue physician in 13 (72%) organizations.

Medical equipment of physicians' backpacks (organizations n=18; chart limited to equipment with >1 item)
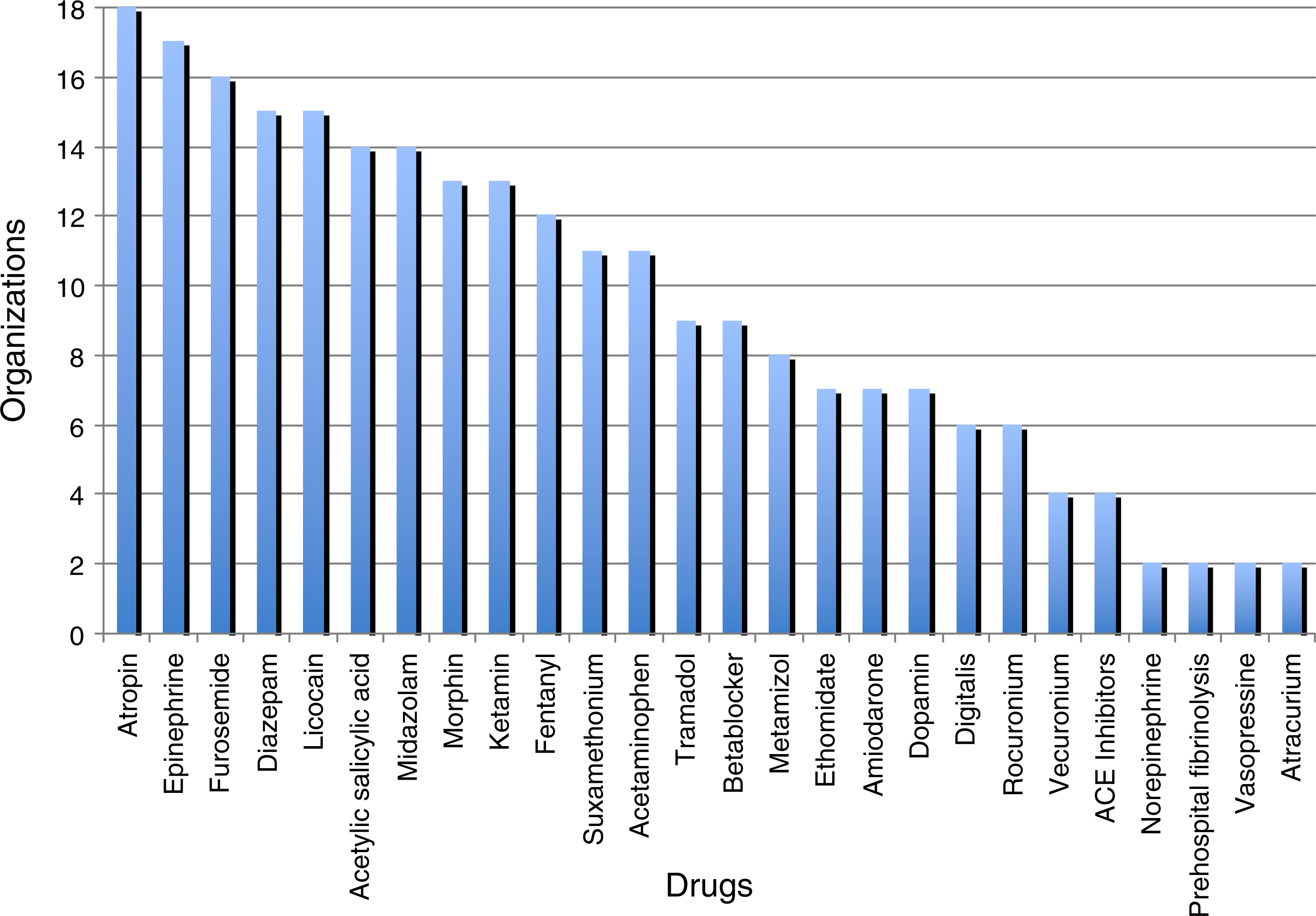
Drugs in physicians' backpacks (organizations n=18; chart limited to equipment with >1 item)
Discussion
In terrestrial rescue, the physician is frequently not the first rescuer on the scene. Trained mountain rescuers, acting as first responders, will perform the initial assessment and maneuvers such as BLS, splinting, wound dressing, and protecting the patient from further heat loss. In some countries these first responders may be paramedics, mountain guides (e.g., in North America) or casualty care certified mountain rescuers (e.g., in United Kingdom) able to give a restricted range of drugs.
In such a circumstance, these drugs may become part of the mountain rescuer's backpack (Arntz et al., 2010; Ellerton, 2006). Thus, most organizations have tailored their medical backpacks into one for trained mountain rescuers and one for physicians. The degree to which these backpacks are complimentary, thus avoiding weighty duplication, will depend on the organization's necessities. All monitored medical backpacks for mountain rescuers are equipped with medical equipment for trauma therapy. In contrast, only eight of 16 (50%) organizations provide an Automated External Defibrillator (AED) thus, potentially compromising the management of a primary cardiac arrest. At mass events, rescue missions in frequented ski resorts, or remote villages with long access time for ALS providers an AED may potentially save lives (Elsensohn et al., 2006).
In addition to the mountain rescuers' backpacks, the physicians' medical backpacks have equipment to give oxygen, cannulate a peripheral vein, and administer intravenous fluids. All backpacks for physicians are equipped with ALS material according to the International Liaison Committee On Resuscitation (ILCOR) guidelines (Morrison et al., 2010; Nolan et al., 2010).
Blood pressure measurement devices are part of all backpacks and pulse-oximetry in 13 out of 18 (72%). The additional weight of a blood pressure cuff must be evaluated against other ways of monitoring and clinical findings and the less weight of a pulse oximetry. However, in cases such as traumatic brain injury (TBI) or permissive hypotension treatment (Sumann et al., 2009), accurate blood pressure measurement is mandatory.
Seventeen out of 18 (94%) of the physician's backpacks have equipment for tracheal intubation or a supraglottic airway device (Cook et al., 2006). Mirroring the finding of the rescuers' backpacks, an AED or a manual defibrillator is less frequently part of the equipment (8/18, 44%). An ECG is included only in 7/18 (40%) of physicians' backpacks. A monitoring device with the possibility of defibrillation should be considered to be part of every physicians backpack to detect and immediately treat arrhythmias or other cardiac dysfunctions. This should also be fact for all medical helicopter operations.
Drugs are limited because of weight and available space. A minimum drug equipment should include acetylic salicylic acid, a strong opioid (e.g., morphine) and nitroglycerin (to treat an acute coronary syndrome) (Arntz et al., 2010); cristalloids/colloids and a vasopressor for shock (Sumann et al., 2009), and ketamine/midazolam for analgesia/sedation during procedures (Bredmose et al., 2009; Ellerton et al., 2009). Hyperosmotic solutions so far did not show improved outcome of traumatic hypovolemic shock and severe TBI (Bulger et al., 2011; Rockswold et al., 2009) but may reduce weight. Also their considerable volume effect may be advantageous in mountain rescue missions (Kreimeier et al., 2002; Nolan, 2001). The storage and operating environmental temperature of equipment and drugs should be considered (Kupper et al., 2006). The specialization of a physician influences the backpack contents in many instances. For example, an anesthesiologist's backpack, when compared to one of a general physician, may contain more advanced airway management equipment, hypnotics, and muscle relaxants.
Oxygen is a universal part when treating patients with medical and trauma emergencies, yet only six of 16 mountain rescuers' backpacks contain it. Frequently, oxygen is in limited supply because of its weight, even when lightweight high-pressure cylinders are used (Ellerton, 2006). Techniques to employ oxygen efficiently such as a Venturi mask with a reservoir (Murphy et al., 2001) or an Oxymizer® (www.chadtherapeutics.com/usa/Disposable-Conservers/Oxymizer.html) allow tailoring the oxygen flow rate to the oxygen saturation as determined by pulse oximetry (Leach et al., 2009).
The weight of backpacks: monitoring devices range from 490 grams (AED with ECG function) and 2100 g for the smallest ECG with complete monitoring functions. Physician's backpacks with all recommended items usually weigh approximately 12 to 20 kg. Backpacks for first responders range from 5 to 8 kg.
Limitations
One limitation of this study should be mentioned. First, only 14 out of 21 member countries participated in this inquiry. The possibility that the questionnaire did not include all drugs or equipment used by the participating organizations in a defined area should also be mentioned. A responder bias may be inherent to this questionnaire. Generalization of our data may be limited, because not all organizations associated with ICAR MEDCOM participated in this study. According to the aims of this study, adequacy and usefulness of technical medical devices and drugs have not been evaluated as this would be a task of another study. We are not recommending a detailed list of contents as there are no scientific data to evaluate a specific pattern of injuries under special circumstances in a given area. Therefore the recommendations are a consensus of experts.
Conclusion and Recommendations
In mountain rescue, medical equipment transported to a casualty has to be restricted to the most essential items because weight in helicopter emergency medical services is at a premium or during terrestrial rescues the equipment has to be carried long distances over a prolonged time (Tomazin, 2003). Medical backpacks should be equipped according to national laws, medical emergencies in a given region, climate, geography, medical training of rescuers, and funding. Backpacks for first responders should contain equipment for BLS (Elsensohn et al., 2006; Paal et al., 2007), splinting (Ellerton et al., 2009), wound dressing, blood pressure, and temperature measurement. Recommendations for mountain rescuer's medical backpacks are shown in Table 2. Backpacks for physicians should enable ALS, and treatment of trauma, anaphylaxis, pulmonary edema, and hypertensive urgency. Recommendations for physician's backpack in mountain rescue are shown in Table 3. However, the contents of a physician's and paramedic's backpack should be adapted to the skills of a given rescuer. Oxygen, for example, may be the most important drug in AMS; however the weight can exceed manpower and the limited capacity may reduce usefulness. A defibrillator should be considered to be in every physician's backpack. In order to save weight, the physician's backpack should be complementary to the mountain rescuers' medical backpack. Standards for training in the use and maintenance of medical equipment should be enforced (Elsensohn et al., 2009). Mountain rescuers, paramedics, and physicians should only use familiar tools and drugs.
Footnotes
Author Disclosure Statement
This study was not supported financially or materially by any producer of ventilation devices. The authors are not involved in any financial interest and did not get any grants or patents concerning the described devices.
Acknowledgments
These recommendations have been discussed and officially approved at the ICAR MEDCOM at the meeting in Chamonix (Switzerland), Bansko (Bulgaria), and Zermatt (Switzerland) by the following members: Gege Agazzi (I); Fabian Argewone (F); Sara Batista (E); Marc Blancher (F); Jeff Boyd (CDN); Bruce Brink (CDN); Hermann Brugger (I); Vera Buchet (F); Ivana Buklijas (HR); Damien Cabane (F); Ramon Chiocconi (RA); Rik Decker (ZA); Florian Demetz (I); John Ellerton (E&W); Fidel Elsensohn, Vice President (A); Yuuji Hatori (J); Martin Ivanov (BG), Kenji Kimura (J); Tim Kovacs (USA); Xavier Ledoux (F); Werner Mahrlein (D); Marko Majstorovic (SRB); Scott McIntosh (USA); Jose Morandeira (E); Maria Antonia Nerin (E); Peter Paal (I); Mato Poharka (SK); Gula Przemyslaw (PL); Oliver Reisten (CH); Peter Rheinberger (FL); Jose Santos (E); Haris Sinifakoulis (GR); Mirom Sorim (RO); Inigo Soteras (E); Günther Sumann (A); Michael Swangard (CDN); Oleg Tcholakov (BG); Steve Teale (SCO); Masatoshi Teshima (J); Iztok Tomasin (SLO); Claire Vallenet (F); Vlahov Vitan (BG); Karen Wanger (CDN); David Watson (CDN); Eveline Winterberger (CH); Isla Wormalo (Eng); Ken Zaffren, Vice President (USA); and Greg Zen-Ruffinen (CH).