
Abstract

This year is the 50th anniversary of the Silver Hut Expedition that took place in 1960–1961. It was a landmark in high altitude physiology as the first major study to take place at a very high altitude after World War II. The leader of the expedition, Sir Edmund Hillary, had made the first ascent of Everest with Tensing Norgay Sherpa just seven years before, and so extreme altitude was very much in the news. In fact between the first ascent of Everest and the Silver Hut Expedition, there were only two successful ascents of Everest, the Swiss from the south in 1956, and the Chinese from the north in May of 1960 (although some people were reluctant to accept the latter). Expeditions to Everest in those days were much more formidable undertakings than they are today.
The Silver Hut Expedition was planned by Hillary and the British physiologist, Griffith Pugh, when they were together in Antarctica in 1957. The official name of the expedition was the Himalayan Scientific and Mountaineering Expedition indicating that it had a dual purpose. A group of physiologists spent up to five months at an altitude of 5800 m studying the acclimatization process at a higher altitude, and for a much longer period of time, than had previously been attempted (Fig, 1). Then in the Spring, the climbers attempted to ascend Makalu, altitude 8481 m, without supplementary oxygen. They were unsuccessful, but if they had been this would have been the highest peak achieved to that date without added oxygen. While the climbers were on Makalu, the physiologists made additional measurements there including maximal oxygen consumption in two subjects at an altitude of 7440 m on the Makalu col.
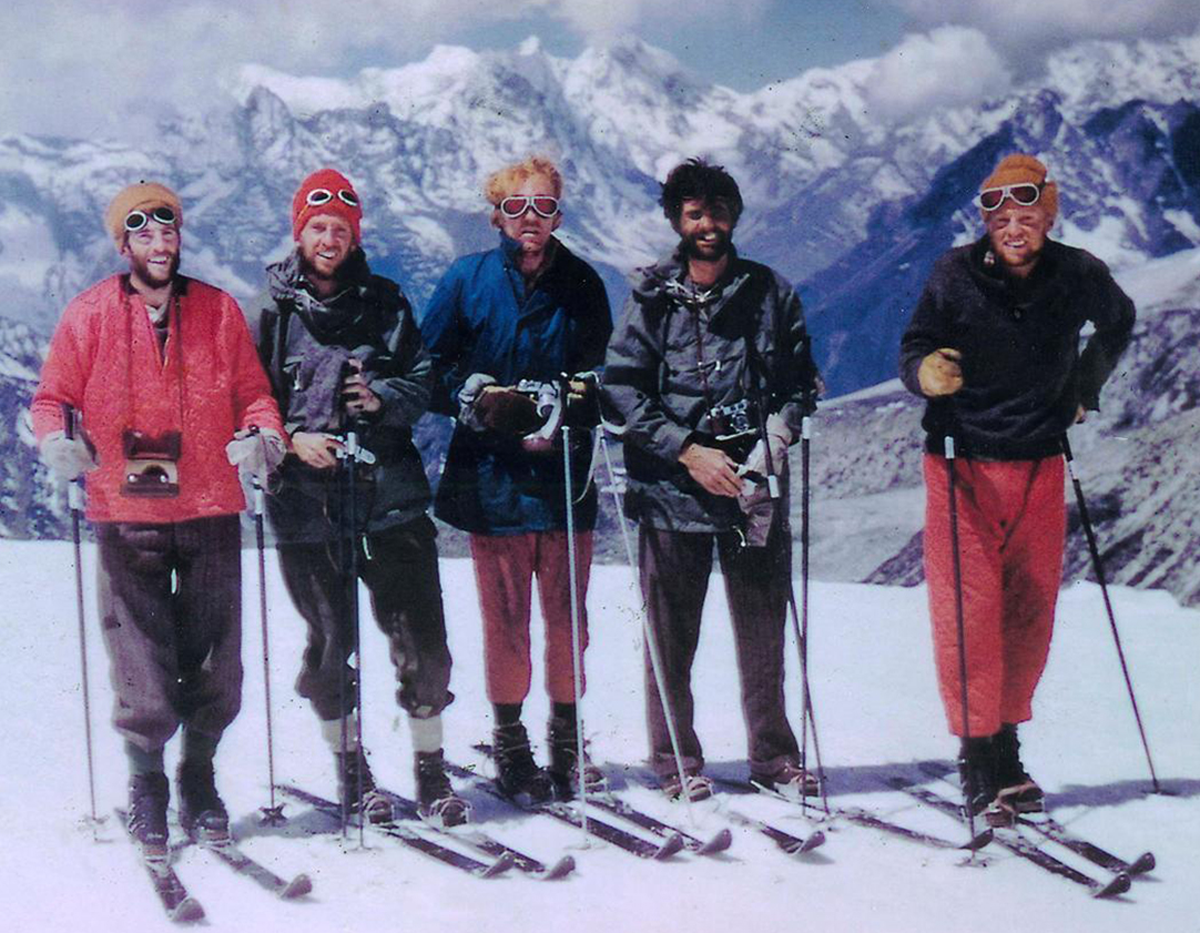
The physiologists who worked in the Silver Hut Expedition during the winter of 1960–1961. Left to right: James S. Milledge, John B. West, L. Griffith, C. E. Pugh, Michael P. Ward, and Michael B. Gill. Not shown are Barry C. Bishop, geologist, and Wally Romanes, building constructor. In addition Sukhamay Lahiri and Thomas Nevison worked in the Hut for short periods.
The Silver Hut Expedition is described in this issue by Jim Milledge, and we have taken advantage of its 50th anniversary to include mini-reviews of four subsequent major experiments at extreme altitude: The American Medical Research Expedition to Everest in 1981, Operation Everest II in 1985, Operation Everest III in 1997, and the Caudwell Xtreme Everest Expedition in 2007.
The Silver Hut Expedition was responsible for many firsts and, as is pointed out in the Milledge article, essentially all of the findings have subsequently been confirmed. It could be argued that 5800 m is no longer regarded as “extreme altitude,” but at that time it was not known whether lowlanders could tolerate such an altitude for such a long period of time. Indeed the relentless loss of weight of the participants indicated that they were probably not able to spend very much longer at that altitude. In addition, the measurements made at an altitude of 7440 m on Makalu, and some alveolar gas samples taken even higher, assured the Silver Hut Expedition of its place in history.
The primary aim of the American Medical Research Expedition to Everest (AMREE) was to obtain the first human physiological measurements at the highest point on earth. In this, the expedition was successful, although necessarily the volume of data was limited. Having said this, essentially no measurements have subsequently been made on the summit in the last 29 years except for confirming the barometric pressure. AMREE was partly stimulated by measurements made at 7440 m altitude on the Silver Hut Expedition that raised anew the question of whether humans could ever reach the summit of Everest without supplementary oxygen. However in the late planning stages of the expedition, Rheinhold Messner and Peter Habeler provided the answer to be an emphatic yes as a result of their “oxygen-less” ascent in 1978. Among many results, AMREE emphasized the critical importance of extreme hyperventilation at these great altitudes.
Operation Everest II (OEII) took a different tack as described in this issue by Peter Wagner. A simulated ascent of Everest was carried out in a very sophisticated low pressure chamber facility in Natick, Massachusetts, owned by the U.S. Army, and a wealth of data were obtained. Some eight subjects were exposed to increasing high simulated altitudes up to the Everest summit. A major advantage of a chamber study like this is that much more invasive experiments can be carried out than in the field because subjects can be quickly removed from the chamber if serious problems arise. A great deal of new information was obtained on the pulmonary circulation at extreme altitude using cardiac catherization. In addition, very sophisticated measurements of pulmonary gas exchange were made, many muscle biopsies were taken, and there were other procedures that would be almost impossible to carry out in the field. Finally OEII was a triumph of logistics with a very large number of investigators and projects.
Operation Everest III (OEIII) was similar to OEII in many respects. This time, French investigators used a sophisticated low-pressure chamber facility owned by COMEX in Marseille. One interesting difference in the logistics was that prior to entering the chamber, the participants spent several days at the Observatoire Vallot, altitude 4350 m, on Mont Blanc where they acclimatized to that altitude. They were then rapidly transported to the chamber in Marseille. As was the case for OEII, a large amount of new data were obtained. For example, in a study of metabolism, it was shown that there was a negative energy balance essentially caused by a reduced appetite in spite of the traditionally excellent French fare. A particularly interesting finding was transient neurological symptoms in three subjects. One suddenly had difficulty with speaking and writing, and another become dizzy and could not recognize his friends in the chamber. Both subjects were removed as a result. A third subject developed back pain, paralysis of the left leg, aphasia and facial paralysis, but he was given oxygen and was able to proceed with the experiment.
The Caudwell Xtreme Everest Expedition (CXE) of 2007 was a field expedition that approached Everest from the south and was highly successful in that no less than 8 members reached the summit. A unique feature of the logistics was that the expedition was preceded by two expeditions to Cho Oyu, altitude 8153 m, to ensure that the participants could tolerate extreme altitude. A major accomplishment was taking arterial blood samples from four subjects at an altitude of 8400 m when they were descending from the summit. This was done by puncture of the femoral artery in a small tent, a veritable tour de force. Paradoxically, however, much of the effort of the expedition was directed at studying some 200 volunteers who trekked into the Everest Base Camp. The expectation was that extensive studies of these subjects will shed light on the characteristics that allow people to operate effectively at altitudes up to 5400 m.
Other important studies have been done at high altitude, for example, a 1973 Italian expedition in which a large laboratory was set up at the Everest Base Camp and studies were performed on climbers returning from the summit. These and the five extreme altitude projects described here changed our understanding of the physiological and medical responses to extreme altitude out of all recognition during the last 50 years. Not only were they responsible for a sea change in our understanding of severe hypoxia but they also represent a monument to human endeavor under extremely difficult conditions.