
Abstract
Abstract
Bates, Matthew G.D., A.A. Roger Thompson, Kenneth Baillie, Andrew I. Sutherland, John B. Irving, NikhillHirani, and David J. Webb. Sildenafil citrate for the prevention of high altitude hypoxic pulmonary hypertension: double blind, randomized, placebo-controlled trial. High Alt. Med. Biol. 12:207–214.—Exaggerated hypoxic pulmonary vasoconstriction is a key factor in the development of high altitude pulmonary edema (HAPE). Due to its effectiveness as a pulmonary vasodilator, sildenafil has been proposed as a prophylactic agent against HAPE. By conducting a parallel-group double blind, randomized, placebo-controlled trial, we investigated the effect of chronic sildenafil administration on pulmonary artery systolic pressure (PASP) and symptoms of acute mountain sickness (AMS) during acclimatization to high altitude. Sixty-two healthy lowland volunteers (36 male; median age 21 years, range 18 to 31) on the Apex 2 research expedition were flown to La Paz, Bolivia (3650 m), and after 4–5 days acclimatization ascended over 90 min to 5200 m. The treatment group (n=20) received 50 mg sildenafil citrate three times daily. PASP was recorded by echocardiography at sea level and within 6 h, 3 days, and 1 week at 5200 m. AMS was assessed daily using the Lake Louise Consensus symptom score. On intention-to-treat analysis, there was no significant difference in PASP at 5200 m between sildenafil and placebo groups. Median AMS score on Day 2 at 5200 m was significantly higher in the sildenafil group (placebo 4.0, sildenafil 6.5; p=0.004) but there was no difference in prevalence of AMS between groups. Sildenafil administration did not affect PASP in healthy lowland subjects at 5200 m but AMS was significantly more severe on Day 2 at 5200 m with sildenafil. Our data do not support routine prophylactic use of sildenafil to reduce PASP at high altitude in healthy subjects with no history of HAPE.
Introduction
Sildenafil citrate is an orally active, potent and selective phosphodiesterase type-5 (PDE-5) inhibitor (Michelakis et al., 2002; Weimann et al., 2000). PDE-5 affects the NO pathway as it is the predominant enzyme responsible for degradation of cyclic guanosine monophosphate (cGMP) in the lung (Ahn et al., 1991; Beavo, 1995). Inhibitors of PDE-5 therefore prolong the actions of NO that are mediated through cGMP. In a small study at 760 m, Zhao et al. demonstrated that pretreatment with sildenafil nearly completely abolished the pulmonary vasopressor response to breathing 11% oxygen for 30 min in healthy humans (Zhao et al., 2001). More recently, studies at altitude have also shown reductions in pulmonary artery systolic pressure (PASP) in subjects taking sildenafil, (Faoro et al., 2007b; Ghofrani et al., 2004; Richalet et al., 2005) and reduced elevation of PASP from sea level values in subjects taking tadalafil, an alternative PDE-5 inhibitor (Maggiorini et al., 2006).
Headache, one of the main side effects of sildenafil, is also a defining symptom of acute mountain sickness (AMS) (Pfizer, 2006). It is therefore possible that regular administration of sildenafil at altitude may worsen symptoms of AMS. We conducted the largest double-blind randomized, placebo-controlled trial of regular sildenafil administration at altitude to date, to assess the effect of sildenafil on PASP and Lake Louise Consensus AMS symptom score (LLS).
Materials and Methods
Design overview
This parallel-group, double blind, randomized placebo-controlled trial was conducted concurrently with a similar trial of an oral antioxidant vitamin supplement, addressing a different aspect of altitude illness (Baillie et al., 2009). 103 participants were recruited for the Apex 2 research expedition to achieve an adequate sample size for each trial; of these 62 participated in this trial.
This study was approved by the Lothian Research Ethics Committee and informed consent was obtained from each subject after full written and verbal explanation of the study, prior to participation.
Setting and participants
Data are presented from the 62 healthy native lowlanders (36 male; median age 21 years, range 18 to 31) who were randomized to receive either active sildenafil (20 subjects) or placebo (42 subjects). Sea level data were collected at the Wellcome Trust Clinical Research Facility in Edinburgh, Scotland before the expedition. The expedition group was split into five teams of 20–25 participants who travelled to Bolivia in series, following an identical ascent profile. Subjects flew to La Paz, Bolivia (3650 m, 11,975 ft) and spent 4 or 5 days there before ascending in 90 min by off-road vehicles to the Chacaltaya laboratory (5200 m, 17,060 ft) for a 9-day sojourn. The ascent to Chacaltaya was staggered over 2 days for logistical reasons, including transport availability and access to echocardiography within 6 h of arrival at 5200 m.
Randomization and intervention
All 103 Apex 2 expedition participants were randomly assigned to three groups using a computer programme operated by an independent statistician (Dr Bill Adams, University of Edinburgh), as determined by the power calculations for each intervention: placebo/placebo (n=42); sildenafil/placebo (n=20); and placebo/antioxidant (n=41).
The sildenafil/placebo group received 50 mg oral sildenafil citrate (Pfizer, UK) three times daily (8 AM, 1 PM, and 10 PM). In an attempt to minimize side effects, a 50 mg dose was initially administered once daily commencing at sea level on the day the subjects left the UK for Bolivia, then increased over 3 days to total 150 mg daily. All subjects had taken sildenafil for 5 days before the first echocardiographic study at 5200 m and had received a dose of 150 mg daily for 48 h before this study. Trial drug administration was continued for 7 days at 5200 m.
Supplies of sildenafil and masked placebo were obtained directly from the manufacturer. Packs of these tablets were identically packaged in the UK under the supervision of the Head of Clinical Trial Facility, Western General Hospital, Edinburgh, and distributed to the trial participants for personal administration. All researchers and participants were unaware of the group assignments and independent of the individual responsible for the randomization process. De-coding of the study groups took place after all data collection.
Outcomes and follow-up
Baseline physiological and anthropometric data were collected at sea level before the expedition. The primary outcome was PASP assessed by transthoracic echocardiography at 6 h, 3 days, and 1 week following high altitude exposure at 5200 m. Echocardiographic measurements (Acuson Cypress, Siemens Medical Solutions, UK) to assess PASP were made by a single experienced echocardiographer as previously described and validated at high altitude, using the modified Bernoulli equation and an assumed right atrial pressure of 5 mmHg (Allemann et al., 2000). Measurements of the pressure gradient across the tricuspid valve were obtained using a portable real-time, phased-array scanner with an integrated color Doppler system. The echocardiographic data were stored and reviewed by an independent investigator at sea level after the expedition. Reported values represent the mean of at least three measurements.
Secondary outcomes were oxygen saturations by pulse oximetry, severity of AMS using the LLS for the first 7 days at high altitude, and proportion of subjects with LLS>3 on day 2 at 5200 m. This is the time of peak AMS incidence in previous studies with a similar ascent profile (Baillie et al., 2004; Baillie et al., 2009). Oxygen saturations (Sp
Statistical analysis
Sample size was calculated a priori based on previous results (Zhao et al., 2001). Zhao et al. demonstrated a 9 mmHg difference in mean PASP with sildenafil treatment in healthy subjects exposed to normobaric hypoxia. Sildenafil treatment improves clinical parameters in patients with symptomatic pulmonary arterial hypertension and is associated with a reduction in mean pulmonary artery pressure of 5 mmHg (Galie et al., 2005). In this study with healthy subjects, we calculated a required sample size of 16 participants in each group based on 80% power to detect a 9 mmHg difference in the primary endpoint with a type 1 (two-sided) error of 5%, correcting for multiple comparisons as below.
For the primary endpoint, unpaired t-tests were used to analyze differences in mean PASP between sildenafil and placebo groups at sea level and the three time-points at 5200 m. Bonferroni's correction for multiple comparisons was used and a level of p<0.013 was accepted as significant. This statistical approach was adopted in favor of repeated-measures ANOVA in order to maximize the number of subjects included at each time point. For the secondary endpoints, parametric variables including Sp
Times from sildenafil ingestion to echocardiogram were categorised into four groups (0–2, 2–4, 4–6, and >6 hours) and the Kruskal-Wallis test was used to assess the influence of time on mean PASP. All analyses were performed using GraphPad Prism 5 (GraphPad Software Inc., La Jolla, CA).
Results
Figure 1 shows the flow of participants through the trial. One participant in the placebo group developed HAPE while at 3650 m, did not ascend to the high altitude laboratory, and was excluded from the trial. Throughout the trial, it proved technically impossible to obtain satisfactory PASP measurements in seven participants (all from the placebo group) and they were excluded from all the PASP analysis. Twelve further subjects were evacuated from the high altitude laboratory because of severe symptoms of acute mountain sickness and thereby withdrew from the trial (five in sildenafil group, seven in placebo group). PASP and AMS data for these subjects are included until their evacuation. Eight further individual PASP measurements (all at 5200 m, two in sildenafil group, six in placebo group) were rejected as technically unsatisfactory following independent review after the expedition. All AMS data and PASP data from these participants at different time-points are included in the analysis.
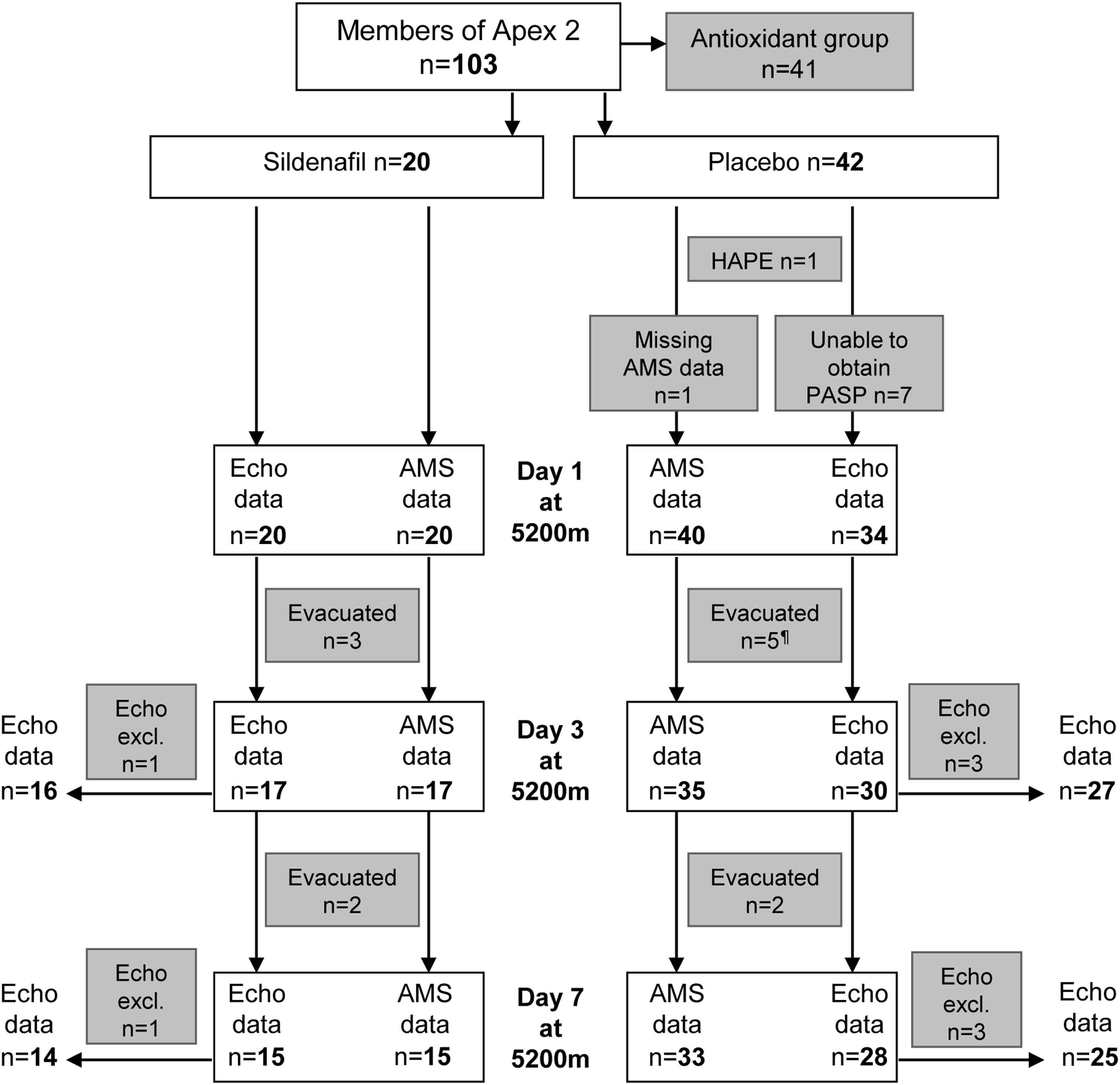
Flow of participants through the trial. ¶One subject evacuated with symptoms of severe AMS was one of the 7 subjects in the placebo group on whom PASP could not be obtained.
Baseline sea level anthropometric, echocardiographic, and pulmonary function data are given in Table 1. There were no significant differences between the sildenafil and placebo groups.
Table shows means±SD. Data were analyzed using unpaired t-tests or †Fisher's exact test.
PASP was elevated at high altitude in both groups (Tables 1 and 2). However, there was no significant difference in PASP between sildenafil and placebo groups at any time-point. There was also no detectable treatment effect on secondary endpoints of Sp
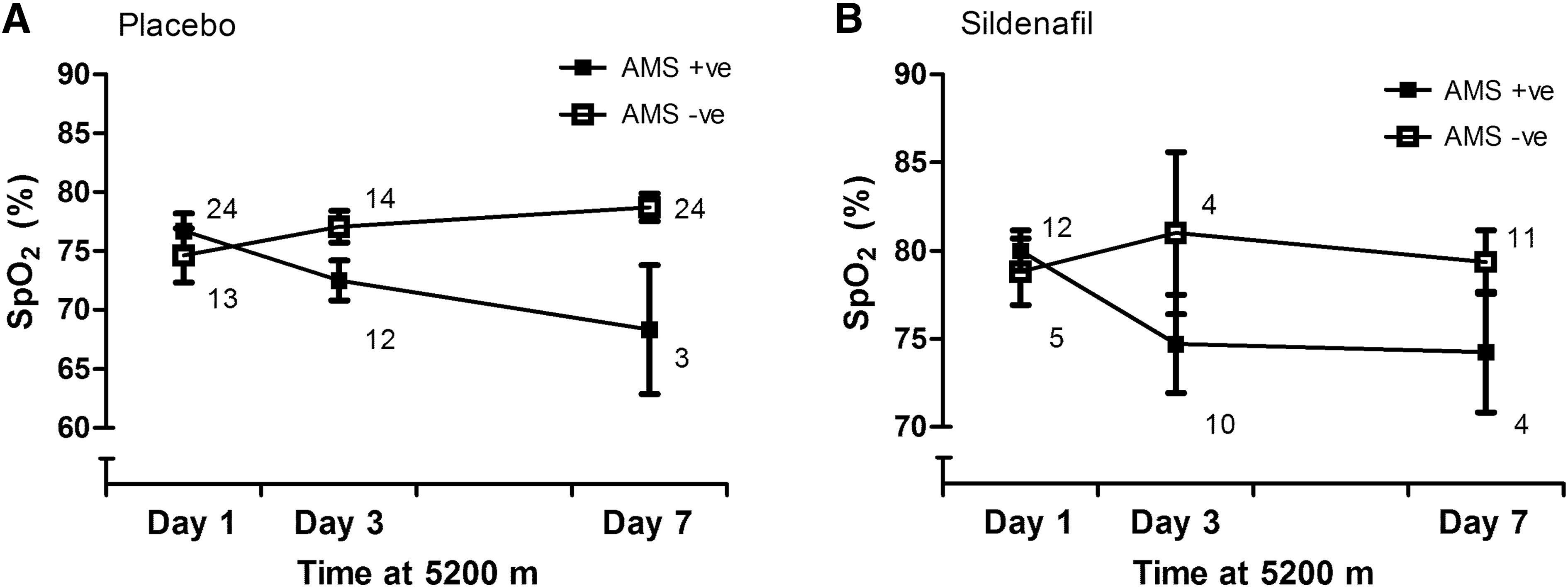
Mean peripheral oxygen saturation (±SEM) in subjects with and without AMS in
Standard errors of the means or interquartile ranges for median data are shown in parentheses. Mean data were compared using unpaired t-tests and median data using Mann-Whitney U-tests.
indicates statistical significance when corrected for multiple comparisons.
To address the possibility that the absence of a drug effect was due to the delays between drug administration (in our thrice-daily regimen) and PASP measurement, we conducted a post-hoc analysis, which showed no detectable effect of time between trial drug administration and echocardiographic assessment on mean PASP in either group (Day 1, p=0.79; Day 3, p=0.72; Day 7, p=0.41). Additionally, compliance was assessed following the expedition by a count of unused tablets at the end of the trial or on subject exit from the trial. Data were available for 37 placebo group subjects and 19 sildenafil subjects. Compliance was good and there was no significant difference between placebo and sildenafil groups (94.2% placebo vs. 88.2% sildenafil, p=0.20).
Data regarding AMS severity as assessed by LLS scale are presented for Days 2–7 at high altitude (Fig. 3). Day 1 was omitted as scores were artificially low since sleep for the preceding night was not at high altitude. Median AMS score on Day 2 at 5200 m was significantly higher in the sildenafil group than the placebo group (p=0.004) with no difference between groups at any other time-point. This difference at Day 2 was not exclusively due to headache. There was a trend toward each symptom score of the LLS to be higher in the sildenafil group as shown in Figure 4. However, there was no difference between the groups in incidence of AMS at the predetermined comparison point of Day 2 at 5200 m; 83 % of the sildenafil group (15/18) and 63 % of the placebo group (24/38) had AMS as defined by LLS criteria (p=0.21). There was no significant difference in the number of subjects in each drug group who withdrew from the trial with severe symptoms of AMS.
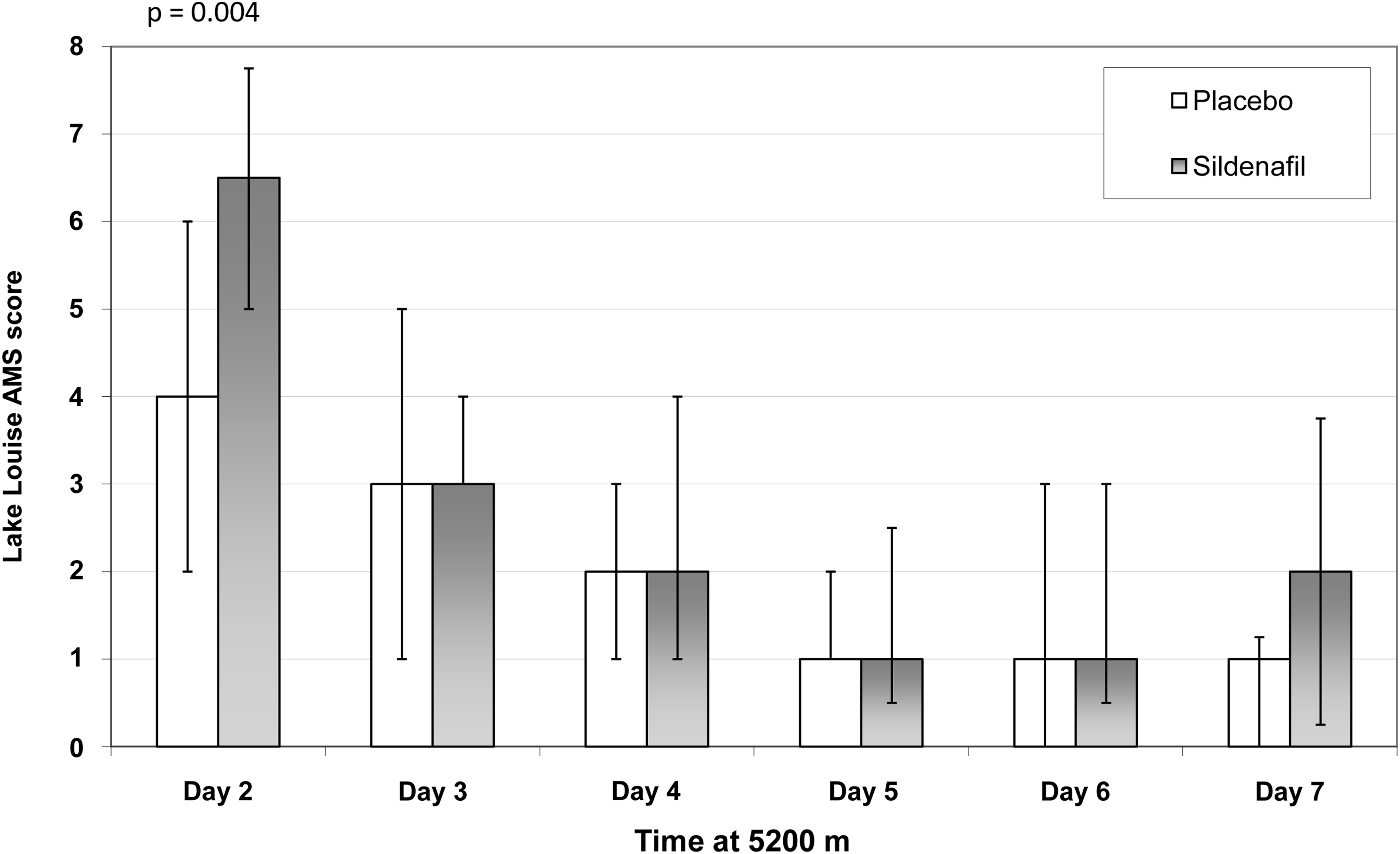
Graph showing medians and interquartile ranges of Lake Louise AMS scores on each day at 5200 m in subjects taking either sildenafil or placebo.
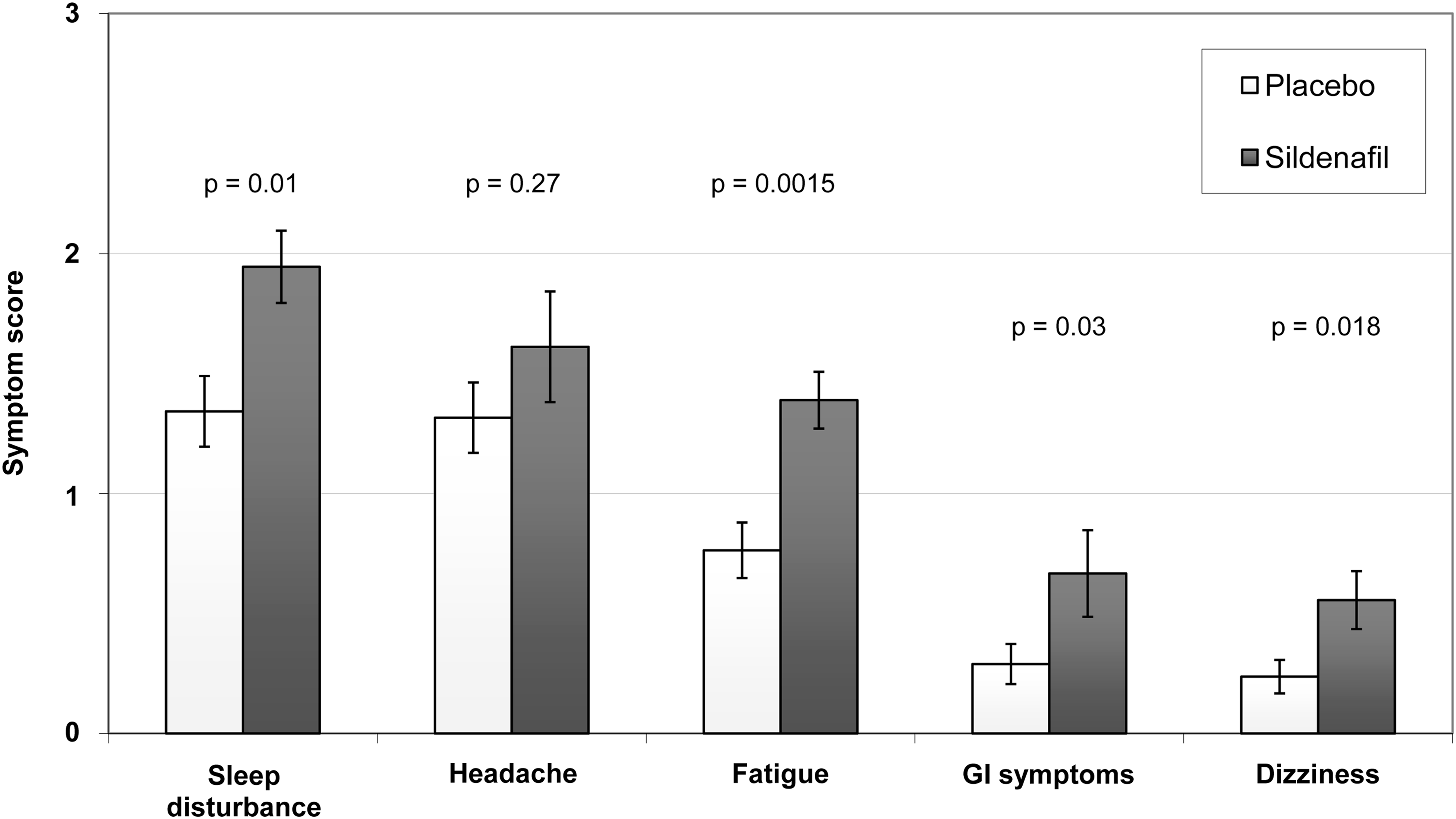
Graph showing mean scores (±SEM) in each self-assessment category of the Lake Louise Score on Day 2 at 5200 m in subjects taking sildenafil or placebo.
Discussion
Daily sildenafil administration had no significant effect on PASP in healthy subjects who had ascended to 5200 m following a period of acclimatization at 3650 m. Our study was powered to detect a reduction in PASP in the range of magnitude demonstrated in previous trials of the effect of PDE-5 inhibitors on PASP (Ghofrani et al., 2004; Maggiorini et al., 2006; Richalet et al., 2005). Although there was also no effect on heart rate, systemic blood pressure, or peripheral oxygen saturation at 5200 m, AMS severity was significantly increased on Day 2 at 5200 m in the treatment group.
Sildenafil and PASP
Our findings contrast with some other published work showing that administration of PDE-5 inhibitors in healthy volunteers significantly reduces PASP at high altitude. In a small crossover study of 14 trained and acclimatized mountaineers, Ghofrani et al. showed that a single oral dose of sildenafil 50 mg significantly reduced PASP after 2 h, with a median reduction of 5.2 mmHg (1.7–8.0 mmHg) (Ghofrani et al., 2004). Richalet et al. studied 12 healthy volunteers with no history of HAPE randomized to receive sildenafil (40 mg three times a day) or placebo. In this study, unacclimatized subjects were flown to 4350 m by helicopter and treatment was started 6 to 8 h after arrival. Pooled echocardiography data from Days 2 and 3 at 4350 m demonstrated a significantly lower PASP in the sildenafil group and the reduction persisted over 5 days of treatment at altitude (Richalet et al., 2005).
There are several possible explanations for these discrepancies. First, our trial is the first to provide data on 10 days of continuous sildenafil use in the setting of altitude hypoxia. Differences in findings between studies in acute hypoxia versus more prolonged hypoxic exposure have also been found with the use of acetazolamide as a pulmonary vasodilator. A significant attenuation of hypoxic pulmonary vasoconstriction by acetazolamide has been demonstrated in dogs and humans exposed to acute hypoxia for up to 4 h (Hohne et al., 2007; Teppema et al., 2007), but no effect was observed on pulmonary artery systolic pressure in trials of this drug during longer exposures to altitude hypoxia (Basnyat et al., 2008; Faoro et al., 2007a). Consistent with our findings, Faoro et al. found no effect of sildenafil on PASP at 5000 m after a 10-day period of acclimatization above 3800 m, but they did demonstrate an effect on mean pulmonary artery pressure and pulmonary vascular resistance (Faoro et al., 2007b).
Second, chronic sildenafil administration commencing before ascent to altitude could theoretically reduce the responsiveness of our subjects to the drug. While we cannot exclude an early effect of sildenafil administration on PASP, for example, during the first 4 days at 3650 m, tachyphylaxis occurring during this period is a theoretical explanation for our findings, In vitro studies suggests a mechanism by which tachyphylaxis could occur, showing upregulation of PDE-5 in cavernous smooth muscle cells after 7 days of sildenafil treatment (Lin et al., 2003). Although studies of chronic sildenafil treatment in pulmonary arterial hypertension argue against this phenomenon (Ghofrani et al., 2003; Michelakis et al., 2003), the mechanism of action in the context of sea-level disease may not be exclusively pulmonary vasodilatation, as sildenafil significantly reduces vascular remodeling in nonhypoxic animal models of pulmonary hypertension (Schermuly et al., 2004).
Third, Hsu et al. have suggested that there may be responders and nonresponders to sildenafil (Hsu et al., 2006). They identified 4 out of 10 trained male subjects who improved their 6 min time trial performance during 12.8% oxygen administration by an average of 39% after treatment with sildenafil. This compared with an average improvement of 1% in the other 6 subjects. The authors speculate that because the decrement in stroke volume during hypoxic exercise was significantly larger in the four responders, that these subjects had a significant increase in either pulmonary artery pressure or pulmonary vascular resistance in response to hypoxia. Administration of sildenafil may therefore have attenuated the pulmonary vasoconstriction, leading to an improvement in performance and an increase in cardiac output. Hsu et al. suggest that differences in the effect of sildenafil on exercise performance and peripheral oxygen saturation in other studies of sildenafil during hypoxic exercise may be explained by their hypothesis (Ghofrani et al., 2004; Hsu et al., 2006; Ricart et al., 2005; Richalet et al., 2005). It is possible that our sildenafil group may have had, by chance, a large proportion of subjects who were less responsive to treatment with sildenafil.
Finally, our subjects were a previously healthy group with no known susceptibility to altitude illness. HAPE-susceptible subjects are known to have an exaggerated pulmonary artery pressor response to hypoxia and are thought to have a deficiency in NO synthesis at altitude (Busch et al., 2001; Duplain et al., 2000). It is conceivable that such subjects may benefit from PDE-5 administration even if, as our study suggests, the effect of sildenafil on healthy subjects is not significant. Indeed, if the hypothesis of Hsu et al. is correct, it is individuals who have exaggerated hypoxic pulmonary vasoconstriction who are likely to benefit most from sildenafil (Hsu et al., 2006).
However, our study also had several limitations. Only 60% (37/62) of all study participants provided a complete data set for analysis of the primary endpoint due to difficulty in obtaining echocardiographic images and the high number of subjects evacuated from the laboratory. Although the trial was adequately powered a priori, this loss of subjects limits the power of the study to detect smaller changes in PASP. Nonetheless, echocardiographic data are available for 87% (54/62) of all study participants on Day 1 at 5200 m, making this study the largest high altitude sildenafil trial to date, and there is no drug effect on PASP at this time-point.
Second, we did not assess the effect of treatment on PASP during exercise. Ghofrani et al. found a larger drug effect during exercise (Ghofrani et al., 2004) and studying participants under these conditions may also have improved the echocardiographic detection rate of triscuspid regurgitation. Finally, it is possible that poor compliance may have adversely affected our ability to detect an effect of drug administration. However, post-hoc analysis of compliance by unused tablet count revealed good compliance with drug administration overall with no difference between the groups.
Sildenafil and AMS
The incidence of AMS in this study was comparable with previous studies following a similar ascent profile (Baillie et al., 2009). Median AMS score was significantly higher in the sildenafil group on Day 2 at 5200 m. Day 2 was the peak of AMS severity, making any drug effect easiest to detect, and was identified a priori for time-point for comparisons. Although no significant difference in AMS severity was detected at other time-points, a possible mechanism for this effect exists as there is considerable overlap between the symptoms of AMS and the known side-effect profile of sildenafil, particularly with regard to headache. Indeed, it has been reported that sildenafil administration influences cerebral vasomotor reactivity (Rosengarten et al., 2006) and increases the incidence of migraine episodes in patients who are prone to them (Kruuse et al., 2003). This finding may have important implications for the use of sildenafil as a prophylactic medication for HAPE or as a potential exercise performance enhancer in healthy subjects at altitude. Although no significant differences in incidence or severity of AMS have been found in other trials of PDE-5 inhibitors, Ghofrani et al. found that 2 of 14 subjects taking a single oral dose of sildenafil 50 mg reported severe headache during exercise, limiting trial participation in 1 subject (Ghofrani et al., 2004). Furthermore, 1 of 11 subjects (Hsu et al., 2006) and 2 of 17 subjects (Ricart et al., 2005) reported headache in other trials of PDE-5 inhibitors in hypoxia. Two of the 10 subjects treated with tadalafil withdrew from Maggiorini et al.'s trial due to severe AMS (Maggiorini et al., 2006). While these results were not statistically significant when compared to the placebo group, headache does appear common in trials of PDE-5 inhibitors at high altitude. Additionally, we have demonstrated a trend towards every symptom of the Lake Louise self-assessment score sheet being higher in the sildenafil group. This raises the possibility that sildenafil may worsen AMS by an unknown mechanism, rather than merely exacerbating headache.
Limitations
As discussed above, this study had several limitations. Most importantly, to investigate the potential utility of sildenafil as a prophylactic medication to control altitude-induced pulmonary hypertension in the real-world, we conducted this study in healthy subjects with no history of HAPE. Our results should therefore not be extended to known HAPE-susceptible patients, in whom there may be differences in the pulmonary vascular response to both hypoxia and PDE-5 inhibition.
Conclusions
Our data demonstrate no effect of sildenafil administration on PASP following ascent to 5200 m in healthy individuals. AMS was more severe in subjects taking the drug. Further work investigating the use of sildenafil as a prophylactic medication or altitude performance enhancer must carefully consider possible deleterious effects of sildenafil on AMS symptoms.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Acknowledgments
We thank the volunteers and researchers who took part in the Apex 2 expedition; the Wellcome Trust Clinical Research Facility, Edinburgh; the Instituto de Investigaciones Fisicas, Universidad Mayor de San Andres; and the Instituto Boliviano de Biología de Altura, La Paz, Bolivia. We are very grateful to Dr. Catherine Labinjoh, Western General Hospital, Edinburgh, for reviewing our raw echocardiography data, Hazel Milligan for packaging the trial drugs, and Dr. Mark Toshner for reviewing the manuscript.