Jacobs, Kevin A., Jochen Kressler, Mark Stoutenberg, Bernard A. Roos, and Anne L. Friedlander. Sildenafil has little influence on cardiovascular hemodynamics or 6-km time trial performance in trained men and women at simulated high altitude. High Alt. Med. Biol. 12: 215–222, 2011.—Sildenafil improves maximal exercise capacity at high altitudes (∼4350–5800 m) by reducing pulmonary arterial pressure and enhancing oxygen delivery, but the effects on exercise performance at less severe altitudes are less clear. Purpose: To determine the effects of sildenafil on cardiovascular hemodynamics (heart rate, stroke volume, and cardiac output), arterial oxygen saturation (SaO2), and 6-km time-trial performance of endurance-trained men and women at a simulated altitude of ∼3900 m. Methods: Twenty men and 15 women, endurance-trained, completed one experimental exercise trial (30 min at 55% of altitude-specific capacity +6-km time trial) at sea level (SL) and two trials at simulated high altitude (HA) while breathing hypoxic gas (12.8% FIo2) after ingestion of either placebo or 50 mg sildenafil in double-blind, randomized, and counterbalanced fashion. Results: Maximal exercise capacity and SaO2 were significantly reduced at HA compared to SL (18%–23%), but sildenafil did not significantly improve cardiovascular hemodynamics or time-trial performance in either men or women compared to placebo and only improved SaO2 in women (4%). One male subject (5% of male subjects, 2.8% of all subjects) exhibited a meaningful 36-s improvement in time-trial performance with sildenafil compared to placebo. Conclusions: In this group of endurance trained men and women, sildenafil had very little influence on cardiovascular hemodynamics, SaO2, and 6-km time-trial performance at a simulated altitude of ∼3900 m. It appears that a very small percentage of endurance-trained men and women derive meaningful improvements in aerobic performance from sildenafil at a simulated altitude of ∼3900 m.
Introduction
Exposure to hypoxia reduces oxygen delivery to peripheral tissues, including working skeletal muscle, and impairs the ability to perform submaximal and maximal exercise. Hypoxia-induced impairments in oxygen delivery are due in large part to reductions in arterial oxygen content (CaO2) that result from low atmospheric Po2 and the narrowing of the alveolar–capillary Po2 gradient that drives pulmonary oxygen diffusion. With more pronounced hypoxia associated with high altitude exposure (>4000 m), oxygen delivery may be further impaired by reductions in maximal cardiac output (Q) and peak limb blood flow (Calbet et al., 2003). Hypoxic pulmonary vasoconstriction (HPV) is an additional factor that influences oxygen delivery under hypoxic conditions. At moderate altitudes, regional vasoconstriction of the vasculature surrounding underventilated alveoli improves ventilation/perfusion (VA/Q) matching. However, more pronounced hypoxia results in widespread pulmonary vasoconstriction and significant increases in pulmonary arterial pressure (PAP) that further reduces CaO2 and Q by hindering VA/Q matching and increasing right ventricular afterload, respectively (Ghofrani et al., 2006). Exercise-induced decreases in CaO2 are also thought to be the result of oxygen diffusion limitations and inadequate hyperventilation (Rice et al., 1999). PAP begins to significantly exceed SL values at ∼3000 m (Harris and Heath 1977) and continues to increase with more severe levels of hypoxia (Boussuges et al., 2000; Ghofrani et al., 2004; Groves et al., 1987; Naeije et al., 2010).
At high actual (4350–5245 m) and simulated altitudes (∼5800 m, 10% FIo2), sildenafil has been shown to significantly reduce PAP, improve oxygen delivery, and attenuate hypoxia-induced reductions in maximal exercise capacity compared to placebo (Faoro et al., 2007; Ghofrani et al., 2004; Richalet et al., 2005). Not surprisingly, the beneficial effects of sildenafil appear to diminish at less severe altitudes, resulting in no significant improvement in maximal exercise capacity at simulated altitudes ranging from ∼3500–4130 m (13.5%–12.5% FIo2) (Cisneros et al., 2009; Kjaergaard et al., 2007; Snyder et al., 2008). However, a subset of the population may still derive significant benefits from sildenafil at these less severe altitudes. Our co-author (Hsu et al., 2006) previously classified 6 of 10 male subjects as nonresponders, exhibiting no significant improvement in 6-km time-trial performance with sildenafil compared to placebo at a simulated altitude of ∼3900 m (12.8% FIo2). However, the remaining 4 subjects were responders and had pronounced hypoxia-induced declines in exercise performance compared to the nonresponders that were attenuated with sildenafil allowing them to perform equally as well as nonresponders. Although PAP was not measured, the pronounced hypoxia-induced declines in arterial oxygen saturation (SaO2) and submaximal stroke volume (SV) of the responders led the authors to surmise that sildenafil responders, like individuals susceptible to high altitude pulmonary edema (HAPE), may have had exaggerated increases in PAP upon exposure to hypoxia. Given that the prevalence of HAPE at altitudes ranging from 4243 to 5000 m has been reported to be ∼0.5%–15% (Bartsch et al., 2002; Cremona et al., 2002; Hackett et al., 1976; Wu et al., 2007), it seems likely that the group of subjects studied by our coauthor (Hsu et al., 2006) had more sildenafil responders (40%) than actually exist in the general population, but this has not been investigated in a larger cohort of subjects to date. Additionally, very little is known regarding the effects of sildenafil in women during exercise at high altitude, and no direct gender comparisons have been made on the efficacy of sildenafil at high altitude.
Therefore, the purpose of this study was to determine the effects of sildenafil on cardiovascular hemodynamics, SaO2, and 6-km time-trial performance at a simulated altitude of ∼3900 m (12.8% FIo2) in larger groups of endurance-trained men and women. It was hypothesized that the prevalence of those deriving meaningful improvements in 6-km time trial performance from sildenafil would be similar to the prevalence of HAPE at similar altitudes (<15%) and that the effects of sildenafil on the cardiovascular hemodynamics, SaO2, and exercise performance of men and women would be similar.
Materials and Methods
Subjects
Twenty male and 15 female healthy, nonsmoking, trained cyclists and triathletes between the ages of 18 and 39 years were recruited (Table 1). Subjects were enrolled in the study only if they met the minimum criterion for peak oxygen consumption (Vo2peak) (50 ml•kg−1•min−1 for men and 40 ml•kg−1•min−1 for women), had a body fat percentage less than 30%, had not lived at altitude (>2100 m) for more than 2 years of their lifetime, had not spent more than 2 weeks at altitude in the 6 months before the study, and agreed not to travel to altitude during the study. The procedures and risks were thoroughly explained to the subjects, and their written, voluntary, informed consent was obtained. The University of Miami Medical Sciences Institutional Review Board approved this study.
Subject Characteristics
Variable
Men
Women
Age, yr
26.3±1.2
25.5±1.4
Height, cm
176.6±1.4
166.8±1.4
Weight, kg
74.4±1.4
60.7±1.6
Body fat, %
15.3±1.2
25.2±1.6
Values are means±SE; n=20 men and 15 women.
General experimental design
Subjects completed a Vo2peak test at SL and a test of peak work capacity (Wpeak) at simulated high altitude (HA; 12.8% FIo2 or ∼3900 m) (Fig. 1). After a SL experimental exercise trial and a HA practice trial, subjects completed 2 experimental exercise trials at HA after ingestion of either placebo or 50 mg sildenafil in double-blind, randomized, and counterbalanced fashion.
Experimental design. HA, simulated high altitude; SL, sea level; SS, 30 min steady state exercise at 55% altitude-specific Wpeak; TT, 6-km time trial; Vo2peak, peak oxygen consumption; Wpeak, peak work capacity.
Screening
During baseline screening, subjects completed PAR-Q and health history questionnaires, a seven-site skin-fold test, and measurements of heart rate (HR), blood pressure (BP) (Dinamap, GE Medical Systems Information Technology, Inc., Milwaukee, WI), and electrocardiographic activity (Max-1, Viasys SensorMedics, Conshohocken, PA) at rest. Female subjects completed a urine pregnancy test before continuing with the study, and women who were pregnant or planning on conceiving during the course of the study were excluded.
Exercise capacity
Vo2peak was assessed at SL during baseline screening using a continuous progressive exercise test to volitional exhaustion (Hsu et al., 2006) on an electromagnetically braked cycle ergometer (Monark Ergometric 829e, Vansbro, Sweden). Wpeak was calculated as described previously (Jeukendrup et al., 1996) to account for work performed in partially completed stages. Expired respiratory gases were collected continuously and analyzed with an online open-circuit metabolic cart (Sensormedics Vmax 229, Viasys Healthcare, Palm Springs, CA). HR, SV, and Q were measured continuously with a noninvasive impedance cardiography device (PhysioFlow PF05 L1, Manitec Biomedical, Macharen, France) described in detail previously (Hsu et al., 2006). Briefly, the PhysioFlow device emits a low-amperage (3.6 mA), high frequency (75 KHz), alternating electrical signal between two sets of electrodes on the supraclavicular fossa of the left side of the neck and the middle of the back at the level of the xiphoid process. SV is calculated from the measurement of changes in transthoracic electrical impedance during the cardiac cycle while simultaneous measurements of ECG activity (V1 and V6) allow for the measurement of HR and the calculation of Q. The PhysioFlow device has been shown to be highly reliable (r=0.95, mean difference for Q of 0.009 L•min−1) with clinically acceptable accuracy (r=0.85–0.94, mean difference for Q of 0.07–0.58 L•min−1) compared to the direct Fick method at rest and during submaximal and maximal incremental exercise (Charloux et al., 2000; Richard et al., 2001). The coefficient of variations for SV and Q from the PhysioFlow across repeated cycle ergometer Vo2peak tests in healthy, trained men was reported to be 3.6% and 3.4%, respectively (Hsu et al., 2006). SaO2 was measured continuously using a portable dual wavelength pulse oximeter placed over the index finger of the left hand (PulseOx 300i, Konica Minolta Sensing, Inc., Osaka, Japan). The pulse oximeter had an operating range of 70%–100% SaO2 and an accuracy of±2% as stated by the manufacturer.
Wpeak at HA was determined at least 48 h after the SL Vo2peak test. Subjects breathed hypoxic gas (12.8% FIo2 or ∼3900 m) for 30 min immediately before and throughout the HA Wpeak test. Hypoxic generators (HYP-123, Hypoxico, New York, NY) equipped with high altitude adapters were used to provide the normobaric hypoxic condition of this test and subsequent experimental exercise trials. Rather than breathing from a large reservoir, the hypoxic gas was delivered to the subject via a sealed facemask covering the nose and mouth at a rate that exceeded VE. The oxygen composition of the hypoxic gas was checked before and after each trial with a portable oxygen monitor (Handi O2, Maxtec, Salt Lake City, UT) that was frequently calibrated. The same protocol as the SL Vo2peak test was used except that respiratory gas measurements were not possible due to the high rate of hypoxic gas delivery through the facemask preventing accurate measurement of VE, FEO2, and FECO2.
Experimental exercise trials
Subjects completed a total of four exercise trials (1 SL experimental, 1 HA practice, 2 HA experimental) with at least 48 h between trials. Each trial consisted of 60 min of rest, 30 min of steady-state exercise at 55% of altitude-specific Wpeak, a 5-min rest, and a 6-km time trial, but the SL and HA practice trials excluded placebo/sildenafil supplementation. Sildenafil supplementation (50–100 mg) has previously been shown to not affect metabolic, cardiovascular, or exercise performance parameters at SL (Faoro et al., 2007; Hsu et al., 2006).
Subjects recorded their diet for 24 h before the first experimental exercise trial at HA and repeated this diet before the second experimental exercise trial. Subjects were asked to refrain from alcohol consumption and exercise for 36 h before testing and not to consume caffeine on the day of testing. Subjects arrived at the laboratory fully hydrated, having consumed 500 ml of water 1 h before testing. One hour before exercise, subjects ingested a capsule containing either placebo (lactose monohydrate) or 50 mg of sildenafil with 200 ml of water in double-blind, randomized, and counterbalanced fashion. An independent pharmacist prepared the placebo and sildenafil using dark blue capsules, making the conditions indistinguishable to both subjects and investigators. Subjects rested and breathed hypoxic gas simulating HA for 60 min immediately after ingestion of the capsule. Sildenafil is rapidly absorbed, reaches peak concentrations in the blood ∼1 h after ingestion, and has a short half-life of ∼4 h (Boolell et al., 1996; Nichols et al., 2002; Walker et al., 1999).
After the rest period, subjects were seated on the electromagnetically braked cycle ergometer and continued to breathe hypoxic gas while electrodes were placed on the chest for PhysioFlow measurements, as described previously (Hsu et al., 2006). The workload on the ergometer was progressively ramped over a period of 5 min until the subject reached 55% of HA Wpeak. HR, SV, and Q were recorded continuously and averaged every 15 sec by the PhysioFlow. BP measured by auscultation and RPE were recorded every 10 min, while SaO2 was recorded continuously as described previously. Subjects were asked to rest the left hand on top of the handlebar as much as possible to prevent occlusion and faulty SaO2 measurements. Subjects drank 200 ml of water while stretching for 5 min upon completion of the steady-state ride and continued to breathe hypoxic air in preparation for the time trial.
The time trial was performed on an electromagnetically braked cycle ergometer (Velotron Dyna-Fit Pro, RacerMate, Seattle, WA) with adjustable road bike geometry and a gearing switch that allowed the subjects to alter the resistance on the flywheel. Therefore, subjects' speed and power output were a function of their self-selected resistance and pedaling cadence. Subjects completed the time trial in the fastest time possible and received no verbal encouragement and no feedback other than the distance covered every km until 4 km and then every half km until the finish. HR, SV, Q, and SaO2 were recorded continuously as previously described. The ergometer software continuously recorded power output, speed, and pedaling cadence, and time to completion was recorded to the nearest second.
In order to decide whether an individual subject in this study exhibited a meaningful improvement in exercise performance, we chose to take into account not only their individual improvement, but also the smallest worthwhile improvement for cycling time trials (1%) and the typical error for a time trial of this distance that is preceded by a steady state moderate intensity exercise bout (3.5%) (Hopkins et al., 1999; Jeukendrup et al., 1996). Therefore, improvements equal to or greater than 4.5% were taken to represent meaningful improvements in 6-km time-trial performance with sildenafil compared to placebo at HA.
Statistics
All data are represented as means±SE. Multiple regression analyses were performed on factors that may explain the hypoxia-induced decrease in Wpeak from SL to HA. The significance of differences in Wpeak and peak cardiovascular data between SL and HA was assessed by paired t-tests. The significance of differences in performance time, average power output, and cardiovascular hemodynamic data between the two HA 6-km time trials was assessed by paired t-tests. The significance of within- and between-condition mean differences of all other data was assessed by ANOVA with repeated measures followed by post hoc analyses using the least significant difference test. Significance was set a priori at α<0.05.
Results
Peak exercise capacity
Exposure to HA resulted in significant 3%–24% declines in Wpeak, Qpeak, HRpeak, and SaO2 at peak in both men and women compared to SL (Table 2). The 23% decline in Wpeak at HA compared to SL for men was significantly greater than the 18% decline for women. The decline in Wpeak from SL to HA was significantly correlated to SL Vo2peak and Wpeak, but not the change in SaO2 at peak from SL to HA, lean body mass, or gender (Table 3).
Peak Exercise Capacity and Cardiovascular Data at Sea Level and Simulated High Altitude
HA, simulated high altitude; HRpeak, peak heart rate; Qpeak, peak cardiac output; Sao2, arterial oxygen saturation at test termination; SL, sea level; SVpeak, peak stroke volume; Vo2peak, peak oxygen consumption; Wpeak, peak work capacity.
Significantly different from SL (p<0.05). ‡Significantly different from corresponding value for women (p<0.05). Significant main effect of gender for Q and SV (p<0.05).
Summary Statistics for the Multiple Regression Analysis of the Dependent Variable, Decline in Wpeak from SL to HA
Independent variable
R
R2
ΔR2
F Change
p
SL Vo2peak
0.777
0.603
0.603
33.470
0.000
SL Wpeak
0.843
0.711
0.684
7.586
0.011
ΔSao2
0.848
0.719
0.008
0.576
0.457
LBM
0.849
0.721
0.001
0.101
0.754
Gender
0.857
0.734
0.013
0.910
0.353
HA, simulated high altitude; LBM, lean body mass; ΔSao2, absolute decline in arterial oxygen saturation at peak from SL to HA; SL, sea level; Vo2peak, peak aerobic capacity; Wpeak, peak work capacity.
Steady-state cardiovascular hemodynamics and SaO2 at SL and HA
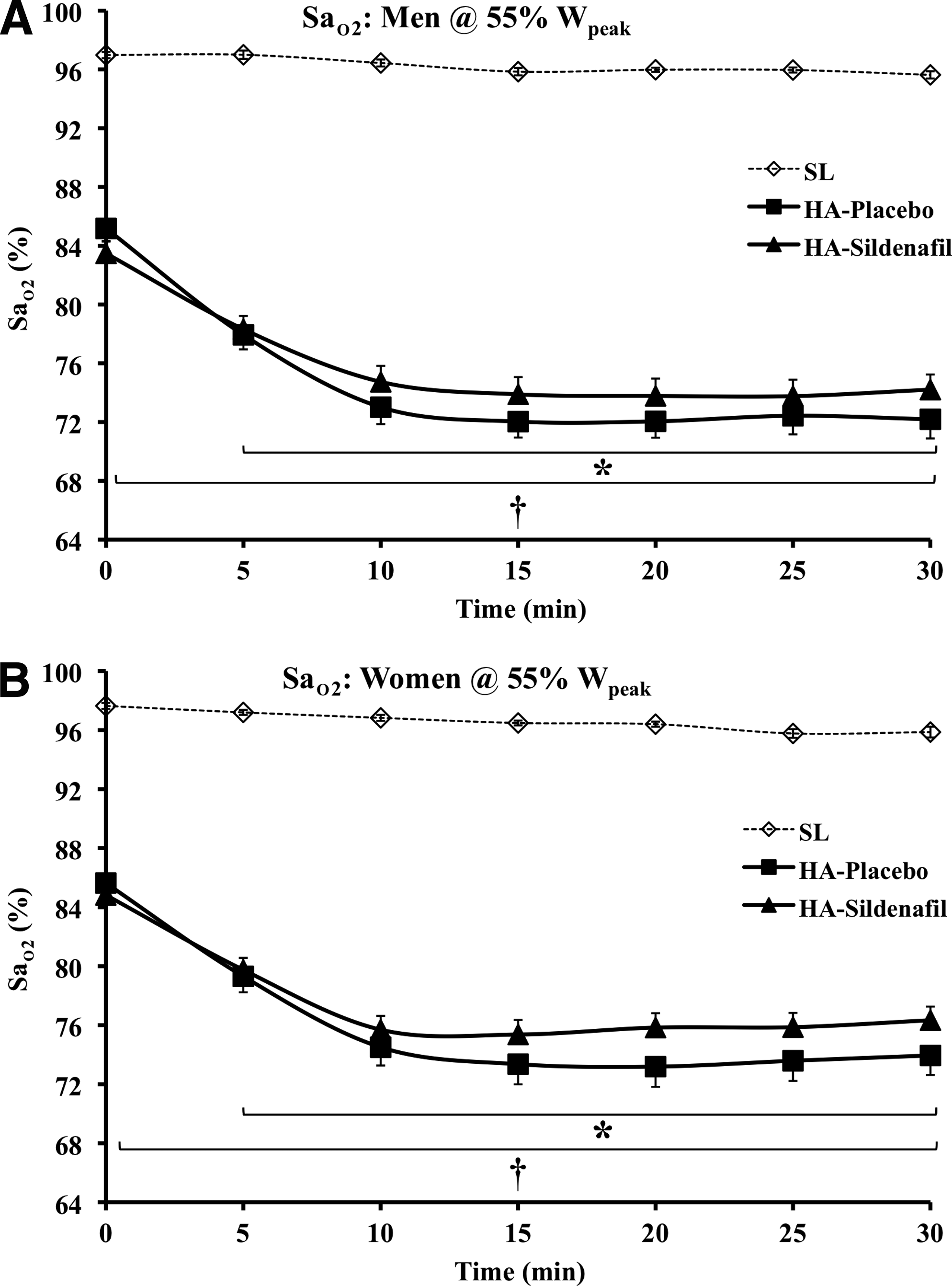
All steady-state data changed significantly from rest to exercise except for SaO2 at SL and diastolic BP in all conditions (Table 4, Fig. 2 and 3). SaO2 was lower at rest and during exercise at HA compared to SL and decreased significantly from rest to exercise at HA in both men and women. Sildenafil resulted in significantly higher SaO2 values in women during exercise at HA compared to placebo, but did not significantly affect any of the other cardiovascular hemodynamic variables at rest or during exercise in men or women
Cardiac output during steady state exercise at 55% of altitude-specific Wattspeak at sea level (SL) and simulated high altitude (HA) for men (A) and women (B). Values are means±SE; n=20 men and 15 women. *Significantly different from 0 min (p<0.05).
Arterial oxygen saturation during steady state exercise at 55% of altitude-specific Wattspeak at sea level (SL) and simulated high altitude (HA) for men (A) and women (B). Values are means±SE; n=20 men and 15 women. *Significantly different from 0 min (p<0.05). †Significantly different from SL (p<0.05).
Steady-State Data at Sea Level and Simulated High Altitude
Values are means±SE; n=20 men and 15 women. 30 min, mean of minutes 20–30.
BP, blood pressure; HA, simulated high altitude; HR, heart rate; Q, cardiac output; RPE, rating of perceived exertion; Sao2, arterial oxygen saturation; SL, sea level; SV, stroke volume; Wpeak, peak work capacity.
Significantly different from SL (p<0.05).
Sildenafil significantly different from placebo (p<0.05).
All steady-state data changed significantly from rest to exercise except for Sao2 at SL and diastolic BP in all conditions. Significant main effect of gender for Q at rest, SV and SBP at rest and during exercise, and RPE (p<0.05).
Time-Trial Performance at HA
Average power output during the 6-km time trial was significantly lower (25%) at HA than SL for men and women and resulted in performance times that were 11% slower (Table 5). The reduced exercise performance at HA was associated with significantly lower SaO2 values, but unaltered HR. Sildenafil did not improve exercise performance and had no effect on average power output, HR, or SaO2 during the 6-km time trial in men or women (Table 5). Two male subjects exhibited improvements in 6-km time-trial performance of 25 and 36 sec (3.6% and 4.7%) with sildenafil compared to placebo and only one (5% of male subjects, 2.8% of all subjects) met the criteria required for a meaningful improvement (>4.5%). No subjects met the criteria of a sildenafil responder set by Hsu et al. (Hsu et al., 2006) of greater than 1 min improvement in 6-km time-trial performance with sildenafil compared to placebo.
6-km Time-Trial Data at Sea Level and Simulated High Altitude
HA, simulated high altitude; HR, heart rate; Sao2, arterial oxygen saturation; SL, sea level.
Significantly different from SL (p<0.05).
Significantly different from corresponding value for women (p<0.05).
Average SV and Q values during the time trial are not reported due to technical difficulties in attaining reliable noninvasive impedance cardiography signals during the time trial. However, the limited reliable data available from 6 men and 6 women indicate that neither average Q (22.8±0.8 and 23.8±0.7 L•min−1, placebo and sildenafil for men; 17.5±0.8 and 18.3±0.9 L•min−1, placebo and sildenafil for women) nor average SV (143±6 and 146±6 ml•beat−1, placebo and sildenafil for men; 107±5 and 114±8 ml•beat−1, placebo and sildenafil for women) were influenced by sildenafil.
Discussion
The simulated altitude administered in this study (12.8% FIo2, ∼3900 m) had the expected effects on SaO2 at peak, HRpeak, SVpeak, Qpeak, and Wpeak (Table 2). The 23%–24% decline in SaO2 at peak and 9%–10% reduction in Qpeak likely resulted in significant declines in oxygen delivery and subsequently an 18%–23% reduction in Wpeak. Our co-author (Hsu et al., 2006) found similar reductions in SaO2 at peak (−26%), Qpeak (−15%), and Wpeak (−24%) with similarly trained male subjects at the same simulated altitude. Not surprisingly, the reductions in Wpeak of the current study are less than those noted at higher actual altitudes of 4350–5245 m (−33% to −39%) (Faoro et al., 2007; Ghofrani et al., 2004; Richalet et al., 2005) and simulated altitudes of ∼5800 m (10% FIo2, −34 to −50%) (Faoro et al., 2007; Ghofrani et al., 2004). The studies performed at 4350–5245 m resulted in similar reductions in SaO2 at peak (−23% to −26%) as the current study, while those performed at a simulated altitude of ∼5800 m resulted in much larger decreases in SaO2 at peak (−38%) (Faoro et al., 2007; Ghofrani et al., 2004) and Qpeak (−21%) (Ghofrani et al., 2004). Taken together, these studies support the contention that hypoxia-induced decrements in oxygen delivery are primarily the result of reductions in SaO2 and subsequently CaO2 and that at altitudes of approximately 4000 m and above reductions in Q play a contributory role to reduced oxygen delivery and maximal exercise capacity (Calbet et al., 2003).
Sildenafil significantly improved maximal exercise capacity compared to placebo at high actual and simulated altitudes (4350–5800 m) that resulted in significant 30%–82% increases in PAP compared to SL (Faoro et al., 2007; Ghofrani et al., 2004; Richalet et al., 2005). Under these conditions, sildenafil reduced PAP by 16%–29%, thereby reducing the detrimental effects of HPV on oxygen delivery and increasing SaO2, Q, and maximal exercise capacity (Faoro et al., 2007; Ghofrani et al., 2004; Richalet et al., 2005). Sildenafil did not significantly improve exercise performance in men or women at 3900 m in the current study and only led to a meaningful improvement in performance in one male subject. Similarly, sildenafil did not significantly improve maximal exercise capacity at simulated altitudes ranging from ∼3500 to 4130 m (13.5% to 12.5% FIo2) (Cisneros et al., 2009; Kjaergaard et al., 2007; Snyder et al., 2008) and did not significantly lower PAP during exercise at a simulated altitude of ∼4130 m (12.5% FIo2) (Kjaergaard et al., 2007; Snyder et al., 2008). Under these conditions, the reduction in oxygen delivery caused by low atmospheric Po2 and subsequent narrowing of the alveolar-capillary Po2 gradient may not have been greatly magnified by HPV-derived increases in PAP, leaving very little room for an ergogenic effect of sildenafil. Indeed while the variability in hypoxia-induced increases in PAP during exercise between subjects can be high, in most individuals PAP is known to begin to significantly exceed SL values at an altitude of ∼3000 m (Harris and Heath 1977).
Hsu et al. (Hsu et al., 2006) found that 4 of their 10 male subjects were responders, defined as those who derived greater than a 1 min improvement in exercise performance from sildenafil compared to placebo, and improved their 6-km time-trial performance by 4.2 min (range 1.2–6.3 min), or 39%. Despite identical experimental procedures (12.8% FIo2, 30 min at 55% altitude-specific Wpeak + 6-km time trial, 50 mg sildenafil in double-blind, randomized, counterbalanced fashion), the current study found no evidence of responders among 20 male and 15 female subjects. The men in the current study were similar to those of Hsu et al. in physical characteristics (Table 1) and closely resembled the nonresponders in terms of Vo2peak (56.5±1.2 vs. 58.1±2.3 ml•kg−1•min−1, Table 2), SV during submaximal exercise at SL (131±5 vs. 119.7±6.4 ml•beat−1, Table 4), and hypoxia-induced declines in SV during submaximal exercise (−7.6% vs. −2.3%). Additionally the men of the current study exhibited 6-km time-trial performance in the placebo and sildenafil conditions (11.3±0.2 vs. 11.3±0.2 min) that were identical to the nonresponders of Hsu et al.
It is reasonable to suggest that the prevalence of sildenafil responders at altitude should be similar to the prevalence of those that suffer from HAPE, as both may be integrally linked to exaggerated hypoxia-induced increases in PAP. With HAPE prevalence rates reported to be between ∼0.5%–15% in the general population at altitudes ranging from 4243 to 5000 m (Bartsch et al., 2002; Cremona et al., 2002; Hackett et al., 1976; Wu et al., 2007), it is perhaps not surprising that sildenafil responders were not identified in the current study. The results of the current study and those that have found no benefit of sildenafil on maximal exercise capacity at simulated altitudes ranging from ∼3500 to 4130 m (13.5%–12.5% FIo2) (Cisneros et al., 2009; Kjaergaard et al., 2007; Snyder et al., 2008) suggest that the subject population recruited by our co-author (Hsu et al., 2006) may have included a greater proportion of responders (40%) than exists in the general population. However, there remains the possibility that factors other than exaggerated hypoxia-induced increases in PAP explain why some individuals respond to sildenafil at less severe altitudes and others do not. A limitation of the current study is the lack of PAP measurements. Future studies in which HAPE susceptible and nonsusceptible subjects are studied in placebo-controlled sildenafil supplementation trials across a wide range of altitudes with the measurement of PAP will help to delineate the physiological characteristics that set sildenafil responders apart.
Sildenafil is typically administered in doses ranging from 25 to 100 mg and the 50 mg dose used in the current study is the recommended starting dose. While doses higher than 50 mg have been shown to result in significantly greater plasma concentrations of sildenafil (Nichols et al., 2002), they may not impart any additional benefits during exercise at high altitude. Hsu et al. (Hsu et al., 2006) clearly demonstrated no differences in cardiovascular hemodynamics or 6-km time trial performance between 50 and 100 mg of sildenafil with the same experimental conditions (30 min at 55% altitude-specific Wpeak + 6-km time trial, 3900 m simulated altitude). Additionally, doses higher than 100 mg are not typically recommended due to the increased risk of side effects. The effects of sildenafil may have been small enough that they could not be detected with the number of subjects used. However, the 35 subjects of the current study represent a larger sample size than in any previous study examining the effects of sildenafil at rest and during exercise at SL and HA (range=10–16) (Cisneros et al., 2009; Faoro et al., 2007; Ghofrani et al., 2004; Hsu et al., 2006; Kjaergaard et al., 2007; Ricart et al., 2005; Richalet et al., 2005; Snyder et al., 2008) and even if small effects were detected their physiological significance may be limited.
The decline in Wpeak from SL to HA was significantly greater for men than women (−23 vs. 18%, p<0.05; Table 2). The relatively few reports of direct gender comparisons at altitude indicate that men either exhibit greater (Paterson et al., 1987; Robergs et al., 1998) or similar (Elliott and Atterbom 1978) decrements in Vo2max compared to women at altitudes ranging from 2500 to 4450 m. Given that only SL Vo2peak and Wpeak were significantly correlated to the hypoxia-induced decline in Wpeak and together explained over 84% of the variance (Table 3), it appears likely that the greater decline in Wpeak for men compared to women was more a function of their higher Vo2peak at SL than an inherent ability of women to better preserve aerobic function at altitude. Men and women were similarly unaffected by sildenafil in terms of cardiovascular hemodynamics, BP, and RPE (Table 4) as well as time trial performance (Table 5). However, sildenafil did significantly increase SaO2 in women only during exercise at HA compared to placebo (Table 4). This is the first evidence that sildenafil may have differential gender effects during exercise at high altitude, and future work will need to focus on whether this effect is consistent or whether it is simply the product of the variable response to hypoxic exposure.
Phosphodiesterase-5 (PDE5) expression is not limited to the vascular smooth muscle of the corpus cavernosum and lungs, and future work should examine the effects of sildenafil at rest and during exercise on other tissues known to express PDE5, including the heart (Corbin et al., 2005). Finally, nitrate supplementation is thought to increase nitric oxide bioavailability and has been shown to reduce the oxygen cost and PCr degradation during both low- and high-intensity exercise (Bailey et al., 2010; Bailey et al., 2009; Larsen et al., 2007). Although 50–100 mg of sildenafil supplementation had no effect on steady state Vo2 during exercise at SL (Hsu et al., 2006), further investigation into the effects of sildenafil on metabolic efficiency appear warranted given its ability to inhibit cGMP degradation and prolong the effects of nitric oxide.
Conclusion
In our study, sildenafil had very little influence on cardiovascular hemodynamics, SaO2, and 6-km time-trial performance among most endurance-trained men and women at a simulated altitude of ∼3900 m. The efficacy of sildenafil during exercise at high altitude is integrally related to its ability to increase oxygen delivery and the magnitude of these effects is dictated by the severity of the hypoxia and likely by individual susceptibility to HPV. It appears that a very small percentage of endurance-trained men and women derive meaningful improvements in aerobic performance from sildenafil at a simulated altitude of ∼3900 m.
Footnotes
Disclosure Statement
The authors have no institutional or commercial affiliations that pose any conflict of interest regarding the publication of this manuscript.
Acknowledgments
The authors wish to thank the participants for their time and efforts, and Rich Viskochil, Steve Hwang, and Katie Chamberlain for their extensive and dedicated help in the laboratory. Additionally, we would like to thank Sonia Mora, RPh, for her assistance with the drug administration, and Jim Gunnerson for his assistance with the PhysioFlow device.
Funding
This study was supported by the World Anti-Doping Agency.
BoolellM, AllenMJ, BallardSA, Gepi-AtteeS, MuirheadGJ, NaylorAM, OsterlohIH, GingellC. 1996. Sildenafil: An orally active type 5 cyclic GMP-specific phosphodiesterase inhibitor for the treatment of penile erectile dysfunction. Int J Impot Res, 8:47–52.
5.
BoussugesA, MolenatF, BurnetH, CauchyE, GardetteB, SaintyJM, JammesY, RichaletJP. 2000. Operation Everest III (Comex '97): Modifications of cardiac function secondary to altitude-induced hypoxia. An echocardiographic and Doppler study. Am J Respir Crit Care Med, 161:264–270.
6.
CalbetJA, BoushelR, RadegranG, SondergaardH, WagnerPD, SaltinB. 2003. Determinants of maximal oxygen uptake in severe acute hypoxia. Am J Physiol Regul Integr Comp Physiol, 284:R291–303.
7.
CharlouxA, Lonsdorfer-WolfE, RichardR, LampertE, Oswald-MammosserM, MettauerB, GenyB, LonsdorferJ. 2000. A new impedance cardiograph device for the non-invasive evaluation of cardiac output at rest and during exercise: Comparison with the "direct" Fick method. Eur J Appl Physiol, 82:313–320.
8.
CisnerosIE, BettencourtJ, TurnerRJ, ZierkeJ, ParkerD, QuintanaR. 2009. Effects of sildenafil on VO2max in trained women with moderate normobaric hypoxia. Med Sci Sports Exerc, 41:S129.
9.
CorbinJD, BeasleyA, BlountMA, FrancisSH. 2005. High lung PDE5: A strong basis for treating pulmonary hypertension with PDE5 inhibitors. Biochem Biophys Res Commun, 334:930–938.
ElliottPR, AtterbomHA. 1978. Comparison of exercise responses of males and females during acute exposure to hypobaria. Aviat Space Environ Med, 49:415–418.
12.
FaoroV, LamotteM, DeboeckG, PavelescuA, HuezS, GuenardH, MartinotJ, NaeijeR. 2007. Effects of sildenafil on exercise capacity in hypoxic normal subjects. High Alt Med Biol, 8:155–163.
13.
GhofraniHA, OsterlohIH, GrimmingerF. 2006. Sildenafil: from angina to erectile dysfunction to pulmonary hypertension and beyond. Nat Rev Drug Discov, 5:689–702.
14.
GhofraniHA, ReichenbergerF, KohstallMG, MrosekEH, SeegerT, OlschewskiH, SeegerW, GrimmingerF. 2004. Sildenafil increased exercise capacity during hypoxia at low altitudes and at Mount Everest base camp: A randomized, double-blind, placebo-controlled crossover trial. Ann Intern Med, 141:169–177.
NicholsDJ, MuirheadGJ, HarnessJA. 2002. Pharmacokinetics of sildenafil after single oral doses in healthy male subjects: Absolute bioavailability, food effects and dose proportionality. Br J Clin Pharmacol, 53,Suppl 1:5S–12S.
25.
PatersonDJ, PinningtonH, PearceAR, MortonAR. 1987. Maximal exercise cardiorespiratory responses of men and women during acute exposure to hypoxia. Aviat Space Environ Med, 58:243–247.
26.
RicartA, MaristanyJ, FortN, LealC, PagesT, ViscorG. 2005. Effects of sildenafil on the human response to acute hypoxia and exercise. High Alt Med Biol, 6:43–49.
27.
RiceAJ, ThorntonAT, GoreCJ, ScroopGC, GrevilleHW, WagnerH, WagnerPD, HopkinsSR. 1999. Pulmonary gas exchange during exercise in highly trained cyclists with arterial hypoxemia. J Appl Physiol, 87:1802–1812.
28.
RichaletJP, GratadourP, RobachP, PhamI, DechauxM, Joncquiert-LatarjetA, MollardP, BrugniauxJ, CornoloJ. 2005. Sildenafil inhibits altitude-induced hypoxemia and pulmonary hypertension. Am J Respir Crit Care Med, 171:275–281.
29.
RichardR, Lonsdorfer-WolfE, CharlouxA, DoutreleauS, BuchheitM, Oswald-MammosserM, LampertE, MettauerB, GenyB, LonsdorferJ. 2001. Non-invasive cardiac output evaluation during a maximal progressive exercise test, using a new impedance cardiograph device. Eur J Appl Physiol, 85:202–207.
30.
RobergsRA, QuintanaR, ParkerDL, FrankelCC. 1998. Multiple variables explain the variability in the decrement in VO2max during acute hypobaric hypoxia. Med Sci Sports Exerc, 30:869–879.
31.
SnyderEM, OlsonTP, JohnsonBD, FrantzRP. 2008. Influence of sildenafil on lung diffusion during exposure to acute hypoxia at rest and during exercise in healthy humans. Eur J Appl Physiol, 103:421–430.
32.
WalkerDK, AcklandMJ, JamesGC, MuirheadGJ, RanceDJ, WastallP, WrightPA. 1999. Pharmacokinetics and metabolism of sildenafil in mouse, rat, rabbit, dog and man. Xenobiotica, 29:297–310.
33.
WuTY, DingSQ, LiuJL, YuMT, JiaJH, ChaiZC, DaiRC, ZhangSL, LiBY, PanLet al.2007. Who should not go high: Chronic disease and work at altitude during construction of the Qinghai-Tibet railroad. High Alt Med Biol, 8:88–107.