
Abstract
Abstract
Luks, Andrew M., Erik R. Swenson. Clinician's corner: pulse oximetry at high altitude. High Alt. Med. Biol. 12:109–119, 2011.—Pulse oximetry is a valuable, noninvasive, diagnostic tool for the evaluation of ill individuals at high altitude and is also being increasingly used to monitor the well-being of individuals traveling on high altitude expeditions. Although the devices are simple to use, data output may be inaccurate or hard to interpret in certain situations, which could lead to inappropriate clinical decisions. The purpose of this review is to consider such issues in greater detail. After examining the operating principles of pulse oximetry, we describe the available devices and the potential uses of oximetry at high altitude. We then consider the pitfalls of pulse oximetry in this environment and provide recommendations about how to deal with these issues. Device users should recognize that oxygen saturation changes rapidly in response to small changes in oxygen tensions at high altitude and that device accuracy declines with arterial oxygen saturations of less than 80%. The normal oxygen saturation at a given elevation may not be known with certainty and should be viewed as a range of values, rather than a specific number. For these reasons, clinical decisions should not be based on small differences in saturation over time or among individuals. Effort should also be made to minimize factors that cause measurement errors, including cold extremities, excess ambient light, and ill-fitting oximeter probes. Attention to these and other issues will help the users of these devices to apply them in appropriate situations and to minimize erroneous clinical decisions.

Introduction
The purpose of this review is to consider the use of pulse oximetry at high altitude in greater detail. We describe the operating principles of pulse oximeters and then examine the types of devices that are available to travelers and medical providers and the potential uses of oximetry at high altitude. We then consider the potential pitfalls of pulse oximetry at high altitude to help all users to avoid erroneous data interpretation and application of the devices in inappropriate situations.
How Pulse Oximeters Work
Complete descriptions of the operating principles behind pulse oximetry are available elsewhere (Schnapp and Cohen 1990; Sinex 1999). Pulse oximeters provide an estimate of arterial hemoglobin oxygen saturation, that is, the percentage of hemoglobin binding sites that are occupied at any one time by oxygen. In general, the saturation is a function of the arterial partial pressure of oxygen (P

This hemoglobin–oxygen dissociation curve depicts how hemoglobin–oxygen saturation varies as a function of the partial pressure of oxygen (P
When considering the utility of pulse oximeters and data in the literature regarding how well they function, three important variables should be taken into consideration: accuracy, precision, and bias (Fig. 2). Accuracy refers to how close the measured value is to the true value. In pulse oximetry, this refers to how close the pulse oximeter value is to the saturation measured from arterial blood by co-oximetry. Precision refers to how close the measured values are to each other. That is, with repeated measurements, will you obtain similar or different values? Bias refers to the difference between the average of the measurements made by the device and its true value. For example, a pulse oximeter that consistently reads 2% below the Sa
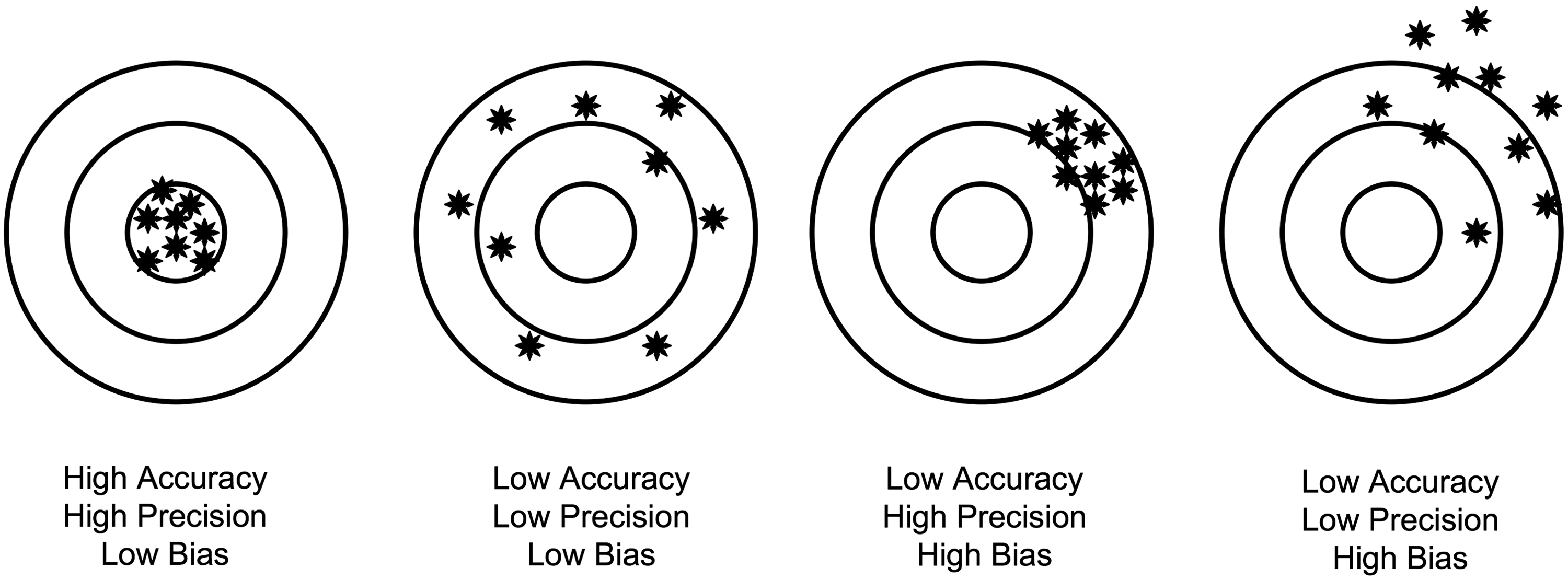
Visual description of the terms accuracy, precision, and bias that are used throughout the literature to evaluate pulse oximeters and other monitoring devices. Each diagram represents a bull's-eye target, and the location of the markers relative to the center of the target demonstrates the meaning of each term.
Types of Pulse Oximeters for Use at High Altitude
Several categories of pulse oximeters might be used in a variety of contexts at high altitude. Images of representative devices from each category are shown in Fig. 3.

Images of pulse oximeters from each of the three main categories of devices that may be used at high altitude: (
Pocket pulse oximeters
This category includes a series of battery-powered devices that are small and light enough to fit in pants or jacket pockets, such as the Nonin Onyx®9500 (Nonin Medical, Inc., Plymouth, MN, USA) or the SPO Medical PulseOx series devices (SPO Medical, Inc., Simi Valley, CA, USA). Given their size and relatively low cost (many of the devices other than the Nonin Onyx 9500 retail for less than $100), the pocket oximeters, a term originally coined elsewhere (Torre-Bouscoulet et al., 2006), are the devices most likely to be used by trekkers, climbers, or guides. While there is an exceptionally large array of U.S. Food and Drug Administration (USFDA)-approved pocket devices, what is lacking is adequate, readily accessible documentation about the accuracy, bias, and other operating characteristics. The Nonin Onyx 9500 is perhaps the only device for which one can easily find such information (Table 1). There is also a distinct lack of information in the medical literature about how well the various devices perform in comparison with co-oximetry, nonportable pulse oximeters, or other small, lightweight devices, both at sea level and, in particular, at high altitude. In one of the few studies of pocket oximeters at high altitude, Torre-Bouscoulet and colleagues (2006) measured pulse oximetry in 96 patients at 2240 m using the Nonin Onxy 9500 and found a mean Sp
Reported accuracy may vary based on motion, type of sensor, adequacy of perfusion, and type of patient (e.g., pediatric vs. adult).
Information obtained from device manufacturers' product brochures:
•Masimo oximeters: http://www.masimo.com/rad-57/
•Nellcor oximeters: http://www.nellcor.com/prod/product.aspx?id=295
•Nonin oximeters:http://www.nonin.com/PulseOximetry/Fingertip/Onyx9500
•Smiths medical oximeter: http://hwww.smiths-medical.com/upload/products/pdf/Mini-TorrPlus3.pdf
Hand-held portable pulse oximeters
The second category is the larger, battery-powered, portable devices, such as the Nonin PalmSat® 2500 (Nonin Medical, Inc.), Nellcor OxiMax™-N-65 (Covidien, Dublin, Ireland), or Masimo Rad-57 (Masimo Corp., Irvine, CA, USA), that can be carried in the palm of the hand, but are too big for easy storage in clothing. These devices are heavier and more expensive than the pocket devices and are probably better suited for use as part of a medical kit with larger groups, in a medical tent on a large expedition, or at a remote clinic. Accuracy data are not reported for Sa
Table-top pulse oximeters
A large number of pulse oximeters are better designed for use in a clinic setting or medical tent and are considered to be too big to carry in a pack or as part of a mobile medical kit. Among the many available devices, representative examples include the Masimo Radical-7 (Masimo Corp., Irvine, CA, USA), Nellcor OxiMax N-600x™ (Covidien), and the Nonin Avant® series (Nonin Medical, Inc.). Some devices, such as the Mini-Torr Plus (Smiths Medical, Kent, UK), function as combined blood pressure and pulse oximetry monitors. These are the most expensive of the oximeters discussed in this article, with costs ranging in the several thousands of US dollars, and are also the devices for which there are the most data in the literature that compare them to other pulse oximeters, as well as co-oximetry. Also, these devices have not been studied at terrestrial high altitude, although data do suggest that many of them overestimate Sa
Uses for Pulse Oximetry at High Altitude
In several situations, pulse oximetry has either a clear indication for use at high altitude or has been proposed as a way to monitor people traveling in this environment.
Evaluation of the ill patient
Clearly, the most important situation in which pulse oximetry should be used is in the evaluation of patients presenting with symptoms of altitude illness or other medical problems. A low Sp
Monitoring the patient with underlying cardiopulmonary disease
Patients with severe underlying cardiopulmonary diseases, such as chronic obstructive pulmonary disease, cardiomyopathy, or congenital heart disease, may be at risk for severe hypoxemia following ascent to high altitude (Luks and Swenson, 2007; Luks et al., 2010). Because high altitude simulation testing (Dine and Kreider, 2008) may not always be feasible prior to their planned sojourn and because travel with supplemental oxygen is logistically difficult, many of these patients may wish to monitor their oxygen saturation using a portable device or by periodic clinic visits upon arrival and use the measured values as a guide for further action (Luks, 2009). No data suggest this strategy improves outcomes at high altitude, but it is a prudent approach in light of the logistical issues previously noted and for the potential of detecting clinical deterioration in certain patients following arrival.
Assessing the likelihood of acute altitude illness following arrival at high altitude
Numerous studies have attempted to determine whether there is a link between oxygen saturation at high altitude and the likelihood of developing acute mountain sickness (AMS), with some studies reporting a link between hypoxemia and the development of AMS (Roeggla et al., 1996; Roach et al., 1998; Basnyat et al., 1999; Tannheimer et al., 2002; Burtscher et al., 2004; Karinen et al., 2010; Koehle et al., 2010) and others reporting no relationship (Roach et al., 1995; O'Connor et al., 2004). No studies have examined a link between hypoxemia upon arrival and subsequent development of high altitude pulmonary edema (HAPE), although Sonna and colleagues (2000) did report a case in which routine pulse oximetry identified a case of HAPE in a person who had yet to present to medical providers. In considering the AMS studies, it is important that only a few of the studies used a prospective approach and asked whether the presence of hypoxemia early in the trip predicts development of AMS at a later time (Karinen et al., 2010; Roach et al., 1998; Tannheimer et al., 2002); the remainder of the studies measured Sp
The question of a link between a low Sp
Predicting summit success
Related to the studies examining a link between Sp
Pitfalls of Pulse Oximetry at High Altitude
Many factors are known to affect the accuracy of pulse oximetry (Table 2) (Sinex, 1999; Jubran, 2004). Regardless of which type of oximeter is employed to measure Sp
Shape of the hemoglobin–oxygen dissociation curve
The hemoglobin–oxygen dissociation curve is sigmoidal in shape whereby oxygen saturation changes minimally in response to changes in arterial oxygen tension at high partial pressures of oxygen, but varies to almost a 10-fold greater extent in response to small changes in arterial oxygen tension at the lower end of the range (20 to 60 mmHg). (Fig. 1). This feature of hemoglobin–oxygen binding can have an important effect on pulse oximeter readings at high altitude. With travel to elevations ≥3000 m, average barometric pressure will fall to a point where the arterial P
Accuracy of pulse oximeter devices at high altitude
The high altitudes at which trekkers and climbers might be using these devices are significant for pulse oximeter function in another important respect. As noted earlier, pulse oximeters actually measure absorbency ratios, and these ratios are converted to an oxygen saturation value using calibration algorithms derived from experiments in healthy volunteers. In these experiments, the volunteers were exposed to hypoxic conditions, and oxygen saturation was then measured by pulse oximeter and in vitro laboratory co-oximetry. This approach was limited by the fact that the volunteers could only be exposed to modest degrees of hypoxia with nadir oxygen saturations of roughly 75% to 80%. At oxygen saturations below these levels, the data output from pulse oximeters is no longer based on actual comparisons between pulse oximetry and co-oximetry and, instead, is based on extrapolation from the data obtained at the higher saturation values. As a result, the accuracy, precision, and bias of these devices fall off at saturation values below 70% to 75% (Sinex, 1999) and may vary considerably between devices with these degrees of hypoxia (Severinghaus et al., 1989). In fact, as noted previously, many manufacturers do not report accuracy data for their devices at saturation values below 70%, since this is not required by the USFDA. (Locating any accuracy data for small pocket oximeters other than the Nonin Onyx 9500 is particularly difficult.) These accuracy problems may be exacerbated in dark-skinned individuals traveling at high altitude; it has been reported that several pulse oximeter models overestimate arterial oxygen saturation with exposure of such individuals to hypoxia (Bickler et al., 2005; Feiner et al. 2007). Given these issues, climbers and trekkers moving to very high altitudes (>4500 m), where baseline oxygen saturation in healthy individuals may fall below 75%, should avoid making clinical decisions based on small differences in oxygen saturation compared with other travelers in the group or with earlier values for a particular individual.
What is a normal saturation for a given altitude?
Clearly, oxygen saturation should decline with increasing altitude, but what constitutes a “normal” saturation for a given elevation is not entirely clear. We can get some sense of the expected values for particular elevations by reviewing oxygen saturation data from research studies conducted across different elevations (Table 3, Fig. 4). Although these values provide a reasonable estimate of the expected values, several important issues must be taken into consideration. First, although the saturation values across studies at a given elevation are often in agreement, other studies report discrepant values.

Graphical display of the average hemoglobin oxygen saturation measured by pulse oximetry in different research studies conducted at high altitude. Data are reported for only those studies that report mean values. Error bars have been omitted from the individual data points. In studies comparing outcomes between treatment and control groups, data are reported for the control group only. In studies comparing sick and healthy (AMS- or HAPE-free) individuals, data are reported for the healthy individuals only. The open circle represents the average oxygen saturation measured by co-oximetry on arterial blood samples taken from 4 climbers at 8400 m on Mt. Everest (Grocott et al., 2009).
Altitudes listed are those reported in the study.
Superscript P: reported values for subjects in the placebo group in a randomized study.
Superscript H: reported values for subjects who were AMS- or HAPE-free (i.e., healthy) during a study comparing AMS or HAPE patients with healthy patients.
IQR: Interquartile range.
Data are from the adult subjects in the study.
Data are from a cross-over design study. Each value given represents the saturation prior to each of the testing situations in the study independent of the order in which participants were tested.
Subjects in this study followed one of two different ascent profiles. Sp
Data from successful summiteers not taking acetazolamide during 5-day ascent to summit.
Second, in many studies, the standard deviations, 95% confidence intervals, or interquartile ranges are very large. Fagenholz and colleagues (2009), for example, reported a mean Sp
Third, it is important to consider the timing of the measurements relative to arrival at high altitude, because, given the effects of acclimatization and maturation of ventilatory responses, the expected value on day 1 at a given elevation will not necessarily be the same as that on day 3 or 4. This is demonstrated nicely in data from Bartsch and colleagues (1991), who measured oxygen saturation in climbers on arrival and over the course of 4 days at 4559 m and noted an increase in Sp
Given all these issues, it is clear that reliable normal values for a given elevation may not be available to people making these measurements. Lacking such data, guides and other travelers may need to rely on the predominant value in their group at a given altitude as the expected value, provided these measurements were taken in an appropriate manner. The problems defining the normal or expected saturation provide further evidence that clinical decisions based on oxygen saturation should not rely on subtle distinctions of only a few percentage points when compared with either other people in a group, earlier readings for a given individual, or known normal values. Instead, clinicians, guides, or other people taking measurements should be looking for large changes or deviations from expected values before implementing action plans.
Other environmental conditions at high altitude
Important environmental conditions at high altitude, including cold temperature and increased sunlight, may affect the accuracy of pulse oximeter readings. Pulse oximeters must distinguish signal from noise and will not generate accurate readings when the signal-to-noise ratio is low (Sinex, 1999). Although many potential sources of low signal-to-noise ratio, such as hypotension, use of vasoconstricting agents, and peripheral vascular disease, are more likely in a hospital setting than among travelers at high altitude, another factor, cold-induced peripheral vasoconstriction, may affect device accuracy. Intense vasoconstriction may limit blood flow to the extremities and, as a result, decrease the pulsatility of flow necessary to detect an accurate signal. Also, the reported temperature range for operation of many devices is above 0°C (Table 1). For these reasons, people traveling in cold environments should ensure that they are taking measurements within conditions appropriate for their oximeter and that the individuals have warm extremities prior to any measurements. Caution should also be used when interpreting values in travelers assessed during hypothermia.
Ambient light interference from a variety of sources has been shown to affect the accuracy of pulse oximeters by causing what is referred to as false signal (Sinex, 1999). Given that sun exposure is increased at high altitude, particularly when individuals are traveling on snow-covered terrain, it is reasonable to ask whether this could be a source of false signal at high altitude. Several reviews on pulse oximetry mention this possibility (Schnapp and Cohen, 1990; Sinex, 1999), but primary literature supporting this claim is difficult to find. When using a pulse oximeter in any light conditions, care should always be taken to ensure that the device fits well on the finger, and finger devices should not be applied to earlobes or toes, because the poor fit in these situations allows excessive ambient light into the device sensor. Given the possible interference from excessive sunlight, it is also worth considering doing measurements indoors, in a tent, or by covering the hand in a manner that blocks much of the ambient light.
Dyshemoglobinemias
Dyshemoglobinemias, such as methemoglobinemia or carboxyhemoglobinemia, can cause misleading pulse oximeter values that do not reflect the true level of oxyhemoglobin in the blood. Although the former would be extremely unlikely among high altitude travelers, unless they were using sulfonamide antibiotics or other medications known to cause this problem, the latter is potentially a concern in certain groups, particularly those cooking inside tents or other small, enclosed places. Thomassen and colleagues (2004), for example, have demonstrated that the mean carboxyhemoglobin level rose to 21.5% in seven health volunteers using a cooking stove in a small tent for 120 min, and Foutch and Henrichs (1988) have documented a case of fatal carbon monoxide poisoning in two climbers on Denali. Because the absorbance patterns of carboxyhemoglobin resemble those of oxyhemoglobin at one of the wavelengths used by pulse oximeters (660 nm), the pulse oximeter overestimates the true oxygen saturation in a person with significant carbon monoxide exposure. Although the diagnosis of carbon monoxide poisoning may be apparent in many cases when adequate history is available, in cases where the risk of carbon monoxide exposure is not readily appreciated, the falsely elevated pulse oximeter values can lead to inappropriate assessment of the patient who presents with dyspnea on exertion or symptoms resembling those of acute mountain sickness.
Summary
Pulse oximetry will continue to be widely used at high altitude. Clinics and other medical providers depend on it for the evaluation of people with respiratory and other complaints, and the increasing availability of low-cost pocket devices makes it highly likely that trekkers, climbers, and guides will also use them on a frequent basis. The ease of use makes these devices inherently appealing but, as discussed throughout this review, unrecognized potential pitfalls of the technique could lead to inaccurate measurements and inappropriate clinical decisions. These important considerations are summarized in Table 4. Users of these devices should familiarize themselves with these issues in order to minimize erroneous measurements, use in inappropriate situations, and misinterpretation of data that could lead to unnecessary disruption in high altitude travel plans.
Footnotes
Disclosures
The authors have no conflicts of interest or financial ties to disclose.