
Abstract
Abstract
Acute mountain sickness (AMS) is a common and disabling condition that occurs in healthy individuals ascending to high altitude. Based on the ability of iron to influence cellular oxygen sensing pathways, we hypothesized that iron supplementation would protect against AMS. To examine this hypothesis, 24 healthy sea-level residents were randomized to receive either intravenous iron(III)-hydroxide sucrose (200 mg) or saline placebo, before ascending rapidly to Cerro de Pasco, Peru (4340 m). The Lake Louise scoring system was used to assess incidence and severity of AMS at sea level and on the first full day at altitude. No significant difference in absolute AMS score was detected between the two groups either at baseline or at high altitude. However, the mean increase in AMS score was 65% smaller in the iron group than in the saline group (p<0.05), and the change in AMS score correlated negatively with the change in ferritin (R=−0.43; p<0.05). Hematocrit and arterial oxygen saturation were unaffected by iron. In conclusion, this preliminary randomized, double-blinded, placebo-controlled trial suggests that intravenous iron supplementation may protect against the symptoms of AMS in healthy volunteers.
Introduction
Few medications offer protection from AMS, and those that are effective are associated with side effects (Basnyat and Murdoch, 2003; Dumont et al., 2000; Hackett and Roach, 2001). Increased understanding of the pathophysiology of AMS could lead to development of more effective prophylaxis. Cerebral vasodilatation, increased blood brain barrier permeability, and impaired cerebral autoregulation are all believed to contribute to AMS susceptibility by increasing the risk of vasogenic edema and brain swelling (Bailey et al., 2009a; Hackett et al., 1998; Hackett and Roach, 2001; Wilson et al., 2009). At a cellular level, these cerebrovascular changes may result from enhanced free radical production and/or expression of hypoxia-regulated genes such as vascular endothelial growth factor (VEGF) or nitric oxide synthase (Tissot van Patot et al., 2005; Wang et al., 2009; Wilson et al., 2009).
Recently, iron availability has been shown to influence physiological responses to hypoxia. In iron-replete individuals, iron supplementation reverses hypoxia-induced pulmonary hypertension at high altitude, while iron depletion increases pulmonary artery pressure in this setting (Smith et al., 2008a; Smith et al., 2009). In isolated cells, excess iron availability reduces the stability of the hypoxia-inducible factor (HIF) transcription factors, while iron depletion increases HIF stability and mimics the cellular effects of hypoxia (Epstein et al., 2001; Knowles et al., 2003). Based on these observations, we hypothesized that iron supplementation would protect against AMS. We tested this hypothesis by performing a randomized, double-blinded, placebo-controlled trial in 24 volunteers ascending rapidly from sea level to an altitude of 4340 m.
Methods
Participants
Twenty-four healthy male volunteers (mean age [± SD] 32±10 years) participated in the study. All volunteers were residents of Lima, Peru, were of lowland ancestry, and had not been at high altitude within the preceding 12 months. The study was approved by the Oxford Tropical Research Ethics Committee (Oxford, UK) and the Universidad Peruana Cayetano Heredia Research Ethics Committee (Lima, Peru). All volunteers gave written, informed consent, and all completed the study.
Protocol
Baseline measurements of AMS score, hematocrit, arterial oxygen saturation, and iron status were measured at sea level (Day 0). On the morning of Day 1, volunteers were block-randomized to receive an intravenous infusion of either iron(III)-hydroxide sucrose (200 mg in 100 mL over 30 min; Vifor Inc, St Gallen, Switzerland) or saline placebo (100 mL over 30 min). Within 2 h of the infusion, volunteers began the ascent by road to Cerro de Pasco (4340 m), which took approximately 8 h. The following day (Day 2, the first full day at altitude), measurements of hematocrit, arterial oxygen saturation, iron status and Lake Louise AMS score were repeated.
Assessment of AMS
The incidence and severity of AMS was assessed using the standard Lake Louise consensus symptom questionnaire (Roach et al., 1993), which includes assessment of the presence and severity of headache, gastrointestinal symptoms, fatigue, dizziness or lightheadedness, and difficulty sleeping, to produce a score between 0 and 15. Following a rise in altitude, AMS is defined as the presence of a headache with an overall symptom score of 3 or more.
Other measurements
Arterial oxygen saturation was measured by pulse oximetry (Pulsox-2, Minolta, Japan). Hematocrit was measured by microcentrifugation of whole venous blood. Iron status was assessed by measurement of serum ferritin and transferrin saturation (Medlab, Lima, Peru).
Data analysis
AMS was assessed in the morning and evening at altitude, and the mean score calculated. Unpaired Student's t-tests were used to compare changes in AMS score, arterial oxygen saturation, hematocrit, and iron status in the iron and saline groups after ascent to altitude, and to compare absolute AMS score at altitude. AMS incidence in the two groups was compared using chi-squared (χ2) tests. Pearson correlation was performed to assess the relationship between changes in iron status and AMS score across all 24 volunteers. Comparisons were considered statistically significant when p<0.05.
Results
Iron status
Iron status at baseline was normal in all individual volunteers, and mean ferritin and transferrin saturation were similar for the two groups (Table 1). Iron infusion produced a substantial rise in ferritin and transferrin saturation, compared with saline (p < 0.001).
Values are mean±SD. Saturation, iron status and hematocrit were measured on the morning of Day 2 at altitude. Lake Louise scores were obtained on the morning and evening of Day 2 at altitude, and the average score is given. *denotes a significantly smaller rise in the iron group than the saline group after ascent to 4340 m (p<0.05). **denotes a significantly larger rise in the iron group than the saline group after ascent to 4340 m (p<0.001).
AMS score
There was no significant difference between absolute Lake Louise AMS scores in the two groups at sea level (p>0.05). AMS scores were increased in both groups at altitude, compared with sea level (Fig. 1). There was no significant difference in absolute AMS score at altitude (p>0.1), but the rise in AMS score was significantly greater in the saline group than the iron group (3.4±0.8 vs. 1.2±0.6 points, mean±SEM; p<0.05). Pearson correlation revealed a significant relationship between the changes in serum ferritin and the changes in AMS score (R=−0.43, p<0.05).
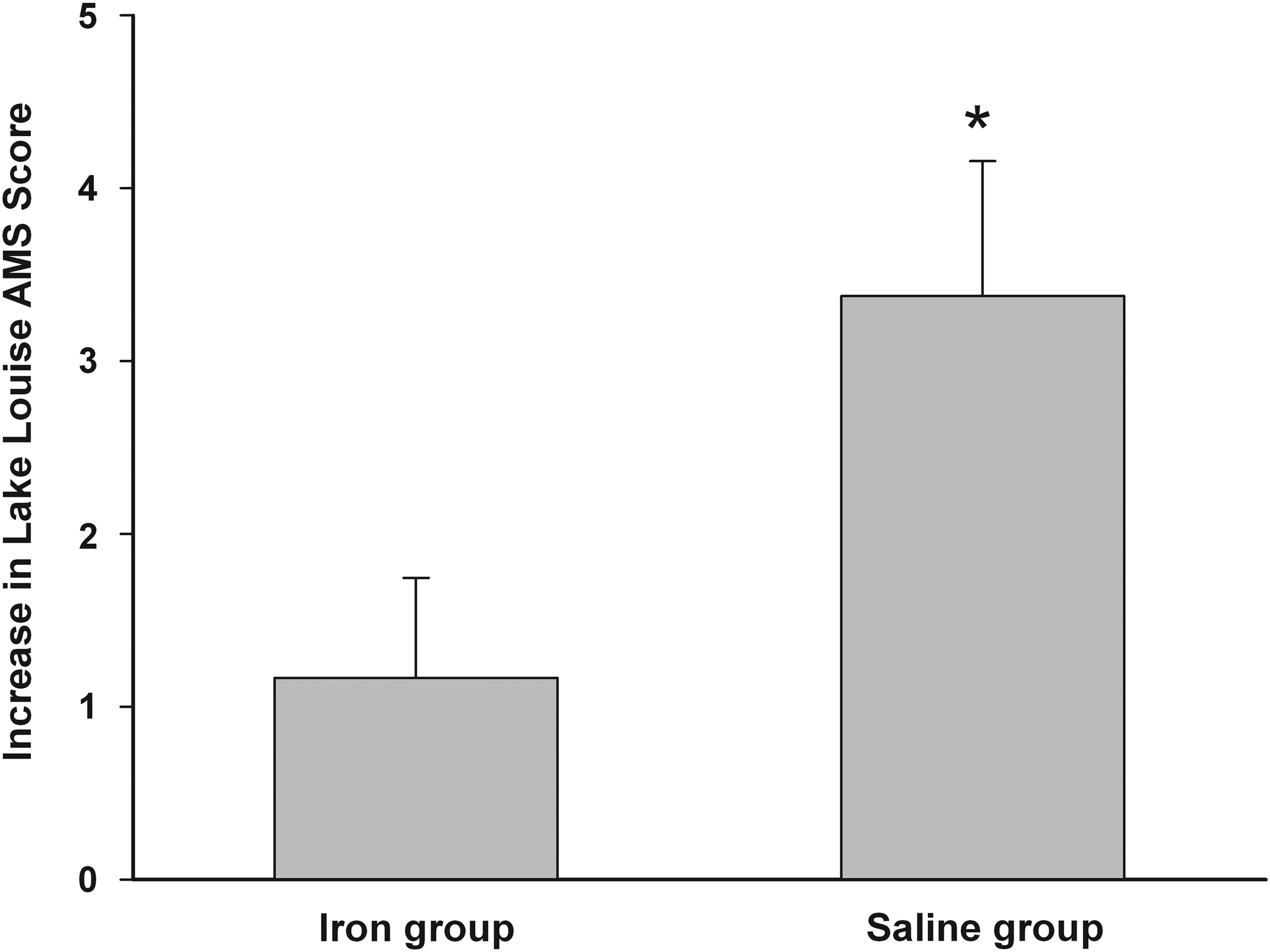
Increase in Lake Louise AMS score after rapid ascent to high altitude. Prior to ascent, volunteers received an intravenous infusion of either iron(III)-hydroxide sucrose (200 mg in 100 mL; n=12) or saline placebo (100 mL over 30 min; n=12). Within 2 h of the infusion, volunteers began the ascent by road to Cerro de Pasco (4340 m), which took approximately 8 h. Values represent the difference between AMS scores at sea level and on the first full day at altitude (mean±SEM). *indicates significant difference between groups (p<0.05).
The incidence of AMS (as defined by headache and total Lake Louise score ≥3) was 67% in the saline group and 42% in the iron group (p>0.4). The incidence of severe AMS (as defined by headache and total Lake Louise score ≥6) was 17% in the saline group and 0% in the iron group (p>0.4).
Other parameters
There was no difference between the changes in hematocrit or arterial oxygen saturation in the iron and saline groups (p>0.4, Table 1). No withdrawals, adverse events, or drug reactions occurred in either group.
Discussion
The principal finding of this study is that prophylactic iron loading reduced the magnitude of the rise in AMS score in healthy volunteers ascending rapidly to high altitude. A secondary finding is that changes in ferritin, a serum marker of cellular iron stores, correlated negatively with changes in AMS score at high altitude. Both findings lend support to recent suggestions of a link between iron availability and physiological responses to hypoxia, and raise the possibility that cellular iron status may influence susceptibility to AMS.
Possible mechanism of action of iron
Iron is a substrate for hemoglobin production and erythropoiesis at high altitude. However, in common with previous reports over longer periods at high altitude (Hornbein, 1962), we found no evidence that iron loading influences the rise in hematocrit during the first 24 h at high altitude. This suggests that any effects of iron loading in our volunteers were independent of hemoglobin concentration. Other authors have reported cardiovascular benefits of iron therapy in patients with iron deficiency and tissue hypoxia, which were not related to hemoglobin concentration (Anker et al., 2009; Tay et al., 2011).
The cellular mechanisms underlying our observations remain unknown, but iron may have direct effects on cellular oxygen sensing. The hypoxia-inducible factor (HIF) family of transcription factors coordinates the cellular response to hypoxia (reviewed in Kaelin and Ratcliffe, 2008). In the presence of oxygen, the alpha-subunit of HIF is continuously expressed but rapidly degraded. The rate limiting step in the degradation pathway is catalyzed by specific oxygen-dependent hydroxylase enzymes (Bruick and McKnight, 2001; Epstein et al., 2001). During hypoxia, the activity of these enzymes is reduced, leading to accumulation of HIF and transcription of target genes. Importantly, these hydroxylase enzymes also depend upon other rate-limiting cofactors, including iron (Fe2+) and ascorbate, and supplementation of either factor decreases HIF levels in cell culture (Knowles et al., 2003).
The HIF pathway is known to play a role in systemic cardiorespiratory physiology (Formenti et al., 2010; Semenza, 2004; Smith et al., 2006; Smith et al., 2008b). It is of interest that the HIF-regulated gene products VEGF and nitric oxide synthase have both been implicated in AMS (Tissot van Patot et al., 2005; Wang et al., 2009; Wilson et al., 2009), and that ascorbate has been suggested by some authors to reduce AMS scores at altitude (Bailey and Davies, 2001). To our knowledge, no previous study has examined the effect of iron on AMS. However, iron loading has recently been shown to reverse hypoxia-induced pulmonary hypertension in healthy volunteers at altitude (Smith et al., 2009). Pulmonary hypertension is a major risk factor for high altitude pulmonary edema (HAPE; Grünig et al., 2000; Hackett and Roach, 2001), suggesting that iron may have multiple benefits at altitude.
An important alternative explanation for our findings relates to the anticipated increase in cellular free radical formation after iron infusion (Kakhlon and Cabantchik, 2002). Given that increased free radical formation and cerebral oxidative stress was recently identified as a risk factor for AMS (Bailey et al., 2009a; Bailey et al., 2009b), further free radical production due to iron seems an unlikely explanation for the apparent benefit seen in the current study. However, future studies could examine this possibility directly, for example by measuring free radical-mediated lipid peroxidation or other blood-derived markers of oxidative stress (Bailey et al., 2009a).
Clinical implications
A limited number of medications have been shown to be effective at reducing the incidence or severity of AMS (Basnyat and Murdoch, 2003; Dumont et al., 2000; Hackett and Roach, 2001). The carbonic anhydrase inhibitor acetazolamide is the most commonly used, and probably relies (at least in part) upon ventilatory stimulation and improved oxygenation for both its beneficial effects and some of its common side effects. Iron had no effect on arterial oxygen saturation in the current study, and is therefore unlikely to have increased ventilation in our volunteers.
An important clinical question raised by our findings is whether iron deficiency might enhance individual susceptibility to AMS or other high-altitude illnesses. This possibility has not been addressed by this study, as all volunteers were healthy and iron-replete at baseline, but could have important implications for many patients traveling to altitude. This is of particular importance when one considers that ascent to altitude itself can induce relative iron deficiency, due to mobilization of iron stores for erythropoiesis (Richalet et al., 1994).
Limitations
The major methodological limitation of our study is the modest sample size. However, it is reassuring that the incidence of AMS in the control group of the current study was in keeping with previous reports after rapid ascent (Dumont et al., 2000; Hackett et al., 1976). The study size may explain why iron supplementation reduced the increment in AMS score with altitude, but produced no significant difference in absolute AMS score, compared with saline. The symptoms of AMS (e.g., headache, fatigue, gastrointestinal upset) are relatively common in a healthy population, and some individuals may be constitutionally more prone to these symptoms than others, whether at high altitude or at sea level. We therefore selected the change in AMS score with altitude to be the primary outcome measure for this study. However, an important role for iron loading would be supported by an additional effect on absolute AMS score in future studies.
Conclusions
In summary, this preliminary trial suggests that iron loading prior to ascent to high altitude may protect healthy individuals from AMS. If confirmed in larger studies, this would have implications not only for AMS prophylaxis in iron-replete individuals, but also for the management of iron-deficient patients wishing to travel to high altitude.
Author Disclosure Statement
The authors have no conflicts of interest or financial ties to disclose.
Footnotes
Acknowledgment
We are grateful to the participants in the study.