
Abstract
Abstract
Drew, Christian M., Shane Colleran, Maarten Zijp, Lama Phuri Lama, Nuru J. Sherpa, Julia L. Kelly, Nina Sulzbach, Denise Prior, Sally A. Currin, Simon Currin, Annabel H. Nickol, and Mary J. Morrell. Preparation and medical outcomes of Nepalese staff and porters compared with foreign nationals on the Annapurna trekking circuit. High Alt. Med. Biol. 12:349–356.—This cross-sectional study investigates preparedness and medical problems in Nepalese staff and porters compared with foreign nationals trekking at altitude in the Nepal Himalaya. 331 Nepalese and 338 foreign nationals in 61 trekking groups were surveyed over 4 weeks on the Annapurna trekking circuit. Foreign nationals reported that 92% of trekking groups received altitude illness information and carried a medical kit. However, fewer than 30% knew the evacuation insurance status of the Nepalese staff and porters on their trek, 39% would not pay for an ill Nepalese national's helicopter evacuation, and 41% reported insufficient resources to carry an individual. Medical problems occurred in 44% of groups. A significantly higher proportion of Nepalese staff and porters were evacuated compared with foreign nationals. No significant differences in Nepalese and foreign national preparation were found between groups with and without medical problems. Medical problems were commonly encountered, yet many groups lacked resources to evacuate someone dangerously ill. Foreign and Nepalese nationals have a duty of care towards each other; recognizing that preparedness relies not only on a first aid kit, but also on knowledge of acclimatization and individuals' insurance is an important part of health and safety for individuals trekking at altitude.
Introduction
Trekking in Nepal is increasing in popularity. From 1991 to 2009, the number of visitors trekking and mountaineering in Nepal increased from 42 to 133 thousand (Khatri, 2010). Many foreign nationals who participate in trekking employ the services of Nepalese nationals, such as porters (load carrying personnel) and staff (who may include trekking guides and cooking staff). Compared with Nepalese staff, porters are often from lower socioeconomic backgrounds, reside at lower altitudes outside of the trekking season, and are paid less for their trekking services. These factors may make them vulnerable to medical problems at high altitude, particularly in remote regions and if insufficiently prepared. Furthermore, cultural differences in symptom and illness reporting may mean that foreign nationals are less able to care for their staff because they are not aware of the medical problems. To our knowledge, there are no data addressing this issue. Therefore, the aim of this project was to conduct an observational cross-sectional study to investigate the preparedness of trekking groups, and the nature of medical problems that occur in Nepalese staff, porters, and foreign nationals trekking in the Nepal Himalaya.
Methods
An observational cross-sectional study was conducted over a 4-week period during the spring 2010 trekking season (March to April 2010). Participants were recruited and questioned in the village of Muktinath on the Annapurna trekking circuit in the Nepal Himalaya. The Annapurna trekking circuit is a 200 km counter-clockwise loop around the Annapurna mountain range. The circuit passes through many villages where accommodation, food, and trekking supplies can be found. Trekkers undertaking this circuit must cross the Throng La pass—at an altitude of 5416 m this is purportedly the highest pass in the world. No climbing is required during the trek, making it accessible to those with less experience. Muktinath is situated on the descending slope of the Throng La pass, at approximately 3700 m.
Participants
Tourists engaged in trekking activities are referred to in this study as foreign nationals, avoiding the term ‘western trekker’, which excludes numerous nationalities. Where jointly discussed, Nepalese staff and porters are referred to as Nepalese nationals. Data collection was undertaken by volunteer researchers from Europe (UK, Ireland, the Netherlands, and Germany) and Nepal. Nepalese researchers were experienced in expedition and trek logistics, and were fluent in English and the local languages.
Groups of trekkers were approached in the afternoon or evening after their arrival in Muktinath from the Throng La pass. Only trekking groups who were accompanied by Nepalese nationals were surveyed. Questionnaires were conducted separately for foreign and Nepalese nationals. The foreign nationals were interviewed by the European researchers. The trekking staff and porters were interviewed in Nepali by the Nepalese researchers. Groups were selected at random from the tea houses in Muktinath, and we varied the order in which the tea houses were visited. We aimed to interview as many groups as possible each day before meal or rest time, ensuring our data were representative of groups in the region, and capturing any medical events that may have occurred.
Interviews were conducted in the presence of all members of the trekking group; where the group consisted of more than two people, a spokesperson was nominated to answer on behalf of the group. The study was approved by the Oxford Tropical Research Ethics Committee (OXTREC ref: 56–09) and the Nepal Health Research Committee (NHRC ref: 518). All participants gave written informed consent.
Survey
Data were collected using a three-part questionnaire. The first part recorded basic trek information: numbers of participants, nationalities, highest altitude, and average duration of expedition. The second part examined the preparedness of the trek with questions focused on first aid equipment and experience, insurance, and prior knowledge of altitude-related illness. Particular focus was placed on the preparedness of the foreign nationals to assist in the event of an illness among Nepalese nationals within the trekking expedition, for example, the ability of trekking groups to carry a dangerously ill Nepalese national to safety, or the willingness of foreign nationals to pay for helicopter evacuation of a Nepalese staff member or porter. The third part of the questionnaire was completed if any member of the trekking group reported experiencing a medical problem. Medical problems were defined as a debilitating event, illness, or injury that was sufficiently severe to affect an individual's ability to comfortably continue with the trek, and which may have resulted in that individual being evacuated (sent down by any means—on foot, horseback, or evacuated via helicopter).
Travel along the Annapurna circuit requires foreign nationals to register at various police checkpoints along the route. The number of foreign nationals arriving and registering in Muktinath was obtained each day during the survey period.
Data analysis
A chi-squared test was applied to compare the preparedness, medical problems, and evacuation outcome of the trekking groups. A two-sample, two-tailed Student's t-test was performed to compare the composition of the trekking groups (number of foreign nationals, Nepalese nationals, staff, and porters), total duration of trek, and day questioned. A preliminary F-test was performed to assess the equality of variance. Significance was considered as p<0.05.
Results
A total of 73 trekking groups were approached during the study period; 68 of these agreed to participate (93%). Of the 68 trekking groups surveyed, there were three groups where only Nepalese nationals were questioned, and four groups where only foreign nationals were questioned; these groups were excluded from further analysis. Therefore, results are reported for 61 groups where both foreign nationals and Nepalese nationals were questioned, comprising 669 individuals; 331 Nepalese nationals, and 338 foreign nationals (Fig. 1).
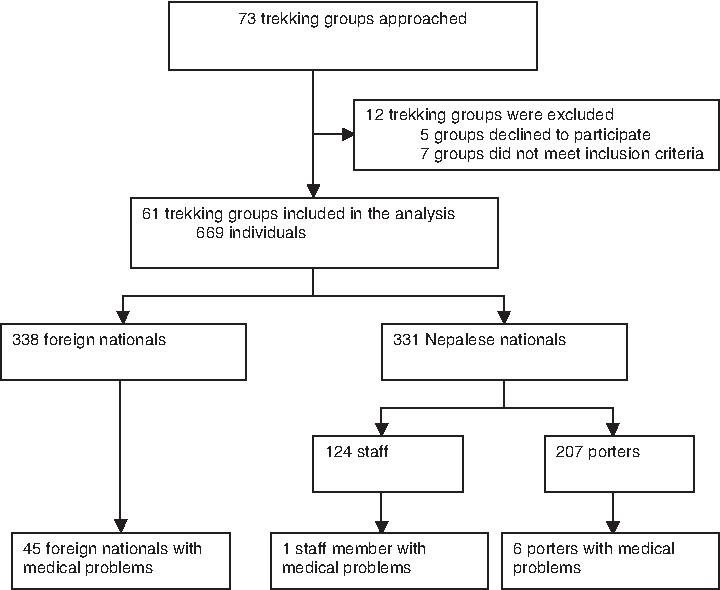
A consort diagram of the number of people approached and included or excluded in the study during survey period, and the number of people who reported medical problems.
During the 4-week study, 1114 foreign nationals registered with the police checkpoint in Muktinath after their descent from the Throng La pass. Three hundred and thirty eight of these individuals were surveyed, representing 30% of the foreign nationals who registered in Muktinath. The median duration of the treks was 17 days (range 7–29), the median day on which trekking groups were questioned was day 10 (range 6–14).
Nepalese and foreign nationals
Fifty-four of the 61 trekking groups employed Nepalese staff and porters, two groups employed only staff, and five groups employed only porters. The number of Nepalese and foreign nationals in each trekking group was similar (median [range]: Nepalese nationals 4 [1–23], foreign nationals 4 [1–19] per group), making the ratio of Nepalese nationals to foreign nationals 1:1. The ratio of Nepalese staff to porters was 1.0:1.7. Foreign nationals from 18 different nationalities participated in the study. The distribution of the foreign nationals' country of origin is presented in Figure 2, with the commonest being France (n=106, 31%), the UK (n=94, 28%), and Germany (n=45, 13%).
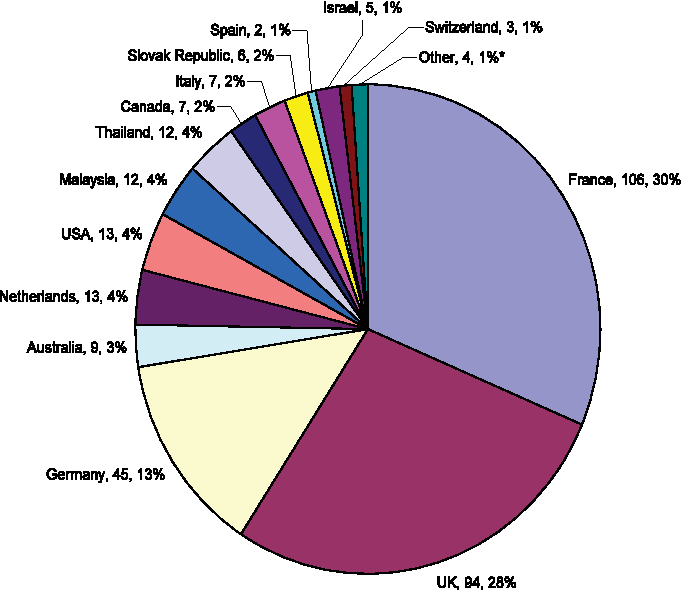
Distribution of foreign nationalities surveyed, by country of origin.
Preparation of the trekking groups
The preparedness of the trekking groups is shown in Table 1. A high proportion of foreign nationals (92%) had received information regarding high altitude illness and acclimatization. The main sources of this information were reported as the Internet, trekking guidebooks, personal physicians, and a short talk on AMS given by the Himalayan Rescue Association at their aid post on the Annapurna circuit at Manang. A high proportion of the Nepalese nationals (83%) knew that the foreign nationals had received this information. Significantly fewer Nepalese nationals, compared with foreign nationals, stated that the trekking group had a comprehensive first aid kit (χ2=10.5, p<0.01).
a=missing data; *p<0.05 compared with Nepalese nationals.
Nepalese nationals were more likely to know if they were insured for search and evacuation, compared with the foreign nationals' reciprocal knowledge of the insurance for the Nepalese nationals on their trek (χ2=23.9, p<0.001; χ2=21.6, p<0.001; staff and porter evacuation, respectively). Likewise, the foreign nationals were more likely to know if they were insured for helicopter evacuation compared with the Nepalese nationals' reciprocal knowledge of this insurance (χ2=13.2, p<0.001). A significantly lower proportion of Nepalese nationals, compared with foreign nationals, reported that foreign nationals would pay for the helicopter evacuation of a seriously ill staff member or porter (χ2=40.0, p<0.001). There was no significant difference when comparing the proportion of Nepalese nationals and foreign nationals who believed they had sufficient resources to carry a dangerously ill Nepalese national from 5000 m to 4000 m (χ2=1.8, p>0.05).
Medical problems
Twenty-seven of the 61 trekking groups (44%) surveyed included one or more member who was affected by a medical problem. Six of the 61 trekking groups (10%) included only Nepalese nationals affected by a medical problem, 22 (36%) included only foreign nationals affected, and one group (2%) included Nepalese and foreign nationals affected by a medical problem. There were no significant differences between the groups with and without medical problems when considering total trek duration (median 16 and 17 days, respectively), day questioned (median 10 and 11, respectively), and group size (median number of Nepalese and foreign nationals (both 6 and 4, respectively), and the number of staff (2 and 1, respectively) and porters (3 and 2, respectively); p>0.05; t-test).
The symptoms of individuals affected by medical problems are presented in Table 2. Nepalese nationals reported significantly fewer medical problems than foreign nationals (χ2=29.3, p<0.0001). The most common medical symptoms were those consistent with the diagnosis of AMS. Three of the 7 Nepalese nationals who reported medical problems had AMS symptoms; all 3 were porters, representing 1% of the 237 porters surveyed. Fifteen of the 45 (33%) foreign nationals who reported medical problems had symptoms of AMS. Although a greater absolute number of foreign nationals, compared with Nepalese nationals, experienced AMS, there was no significant difference in the incidence of AMS experienced by Nepalese and foreign nationals experiencing medical problems (χ2=0.24, p>0.05).
Medical problems were defined as a debilitating event, illness or injury that was sufficiently severe to affect an individual's ability to comfortably continue with the trek. The discrepancy between the number of symptoms presented and the number of individuals experiencing medical problems is due to some individuals experiencing multiple symptoms. *p<0.05 compared with Nepalese nationals.
Evacuation outcome
The outcomes of the 52 individuals who reported experiencing medical problems are presented in Table 3. Of the 7 Nepalese nationals and 45 foreign nationals who reported experiencing medical problems, a total of 20 (38%) were evacuated. A significantly higher proportion of Nepalese nationals were evacuated (5 of the 7; 71%) compared with foreign nationals (15 of the 45; 33%) (χ2=5.5, p=0.02). All 5 of the Nepalese nationals who were evacuated were porters. Fifteen of the 20 individuals evacuated were carried (by their trekking group or horse). Of these, 5 foreign nationals were carried over the Throng La pass (5416 m) by horse. That is, they were carried along part of the trekking circuit, ascending up to 5416 m before their descent to the village of Muktinath (3700 m).
Preparation of groups with and without medical problems
The preparedness of the trekking groups with and without medical problems is shown in Table 4. No significant differences were found between the answers given by Nepalese nationals with and without medical problems (p>0.05 for all comparisons; χ2 test). Similarly, no significant differences were found between answers from foreign nationals with and without medical problems (p>0.05 for all comparisons; χ2 test).
a=missing data; *p<0.05 compared with Nepalese nationals in groups with medical problems; †p<0.05 compared with Nepalese nationals in groups without medical problems.
For groups without medical problems, a significantly lower proportion of Nepalese nationals (76%), compared with foreign nationals (94%), reported that the foreign nationals had read or received information on altitude illness and acclimatization (χ2=4.4, p<0.05). There was no significant difference for groups with medical problems, when considering the same question.
Similarly, for groups without medical problems, a significantly lower proportion of Nepalese nationals (65%), compared with foreign nationals (94%), stated that the group had a comprehensive first aid kit (χ2=6.9, p<0.05). Again, for groups with medical problems, there was no significant difference between Nepalese and foreign nationals' responses to this question. For all other comparisons, where significant differences occurred between Nepalese and foreign nationals' responses, these were present in both groups with and without medical problems.
Discussion
Our study revealed that medical problems were encountered by one or more individuals in almost half of the trekking groups surveyed (44%). Of the people who reported medical problems, a significantly higher proportion of porters was evacuated from high altitude, compared with foreign nationals. No significant differences in preparation were found between Nepalese nationals with and without medical problems, nor between foreign nationals with and without medical problems. This study represents the first investigation of the preparation and medical problems experienced by both Nepalese staff and porters, as well as by foreign nationals along the Annapurna trekking circuit in Nepal.
Preparation of the trekking groups
This study revealed that a large proportion of the trekking groups reported receiving information on altitude illness and acclimatization, and a high number of trekking groups had a comprehensive first aid kit and appropriate evacuation insurance coverage. However, differences existed between foreign nationals' and Nepalese nationals' knowledge of trekking group preparedness. Overall, foreign nationals in fewer than 30% of the trekking groups were aware that their staff and porters were insured for search and evacuation.
Adequate medical and evacuation insurance is essential for emergency planning. During medical emergencies, trekking group participants may be called upon to know the limitations of both their own and other trek and staff members' insurance. These issues highlight the need for good communication between foreign and Nepalese nationals on all aspects of trekking group preparedness. This is particularly important when considering that, according to foreign nationals, approximately 40% of all trekking groups would not pay for helicopter evacuation of a Nepalese national, and approximately 40% of the trekking groups reported insufficient resources to be able to carry a dangerously ill Nepalese member of staff or porter down from an altitude of 5000 m to 4000 m.
Medical problems
Nepalese nationals experienced fewer medical problems than foreign nationals; this difference may reflect a variation in the susceptibility to medical problems (e.g., AMS and diarrhea) between the two groups. Nepalese nationals have a greater familiarity with the environment, and may be pre-acclimatized or more able to acclimatize to high altitude.
However, the difference may also reflect reporting differences; Nepalese nationals may be more reluctant to disclose medical problems in order to maintain employment and professional reputation. Foreign nationals may over-report medical problems because of unfamiliarity or discomfort with the trekking environment. The fact that a greater number of porters than staff experienced medical problems in our study, may potentially be a reflection of an increased susceptibility to medical problems because of poor health prior to the trek, and the lower quality of their equipment and clothing. A previous study examining the incidence of medical problems at high altitude in the Nepal Himalaya revealed 43% of Nepalese nationals and 55% of foreign nationals experienced medical problems (Basnyat and Litch, 1997). This previous study examined the problems encountered during a 22-day trek in a more remote region of Nepal with less infrastructure and support, requiring a higher ratio of porters and staff to foreign nationals; approximately 6 times that seen within our study. The overall incidence of AMS in Nepalese and foreign nationals in this previous study was 7% and 14%, respectively. Our study revealed AMS incidences of 1% and 4% for Nepalese and foreign nationals, respectively. Compared with these previous data, the lower overall incidences of medical problems and AMS reported in our study may be a result of the improved infrastructure, support services, and accommodation on a more popular trekking circuit; therefore our findings may not be translatable to more remote regions. Moreover, the low ratio of porters to foreign nationals on the Annapurna circuit may have contributed to a lower absolute number of medical problems, since Nepalese staff (such as trekking guides) are likely to be better paid, and have improved health compared with porters.
The overall incidence of foreign nationals reporting symptoms consistent with the diagnosis of AMS was found to be 4%. The incidence of AMS has previously been shown to be 34% in trekkers in Nepal at altitudes above 5000 m (Vardy et al., 2006). Direct comparisons between trekking routes are problematic because of differing ascent profiles, which have been shown to be a major determinant for the prevalence of AMS (Schneider et al., 2002). A previous study, conducted in 1998, which examined AMS on the Annapurna trekking circuit showed the incidence to be 29% in foreign nationals crossing the Throng La pass (Gaillard et al., 2004). The difference in the incidences between this previous study and our data may be explained by the method of data collection. In contrast with the previous study, which examined the incidence of AMS symptoms in all individuals, we only assessed AMS symptoms in individuals who reported that they had experienced a medical problem; some individuals experiencing AMS symptoms (e.g., headache) may not have considered these to be a medical problem. In addition, an increase in use of the Internet as a source of information for illnesses and treatments may have also contributed to the decreased incidences seen within our study.
Evacuation outcome
A significantly higher proportion of porters with medical problems was evacuated, compared with foreign nationals. These findings are consistent with previous data, which also showed a greater number of porter evacuations compared with staff and foreign nationals (Basnyat and Litch, 1997). Taken together, these data suggest that when porters report medical problems, they are more severe than those experienced by foreign nationals.
Our study also revealed that 5 of the 15 foreign nationals (33%) who were evacuated were carried along part of the trekking circuit, up to 5416 m, before their descent to the village of Muktinath (3700 m). This method of evacuation may have been used because individuals and trekking groups are often under pressure to complete trekking activities within a certain time period while on vacation. Individuals who ascend in altitude while experiencing medical problems may worsen AMS and place themselves at an increased risk of developing serious medical problems related to hypobaric hypoxia such as HAPE or HACE.
Preparation of groups with and without medical problems
When considering preparedness, measured with our questionnaire, no differences were found between Nepalese nationals with and without medical problems, nor between foreign nationals with and without medical problems, although for groups without medical problems, more of the foreign nationals, compared with Nepalese nationals, reported that they had a comprehensive first aid kit and received information regarding acclimatization. This may be because Nepalese nationals who are exposed to others with medical problems could become more aware of the trekking groups' preparedness. Preparedness plays a key role in reducing certain risks when trekking at high altitude. A previous study has shown that foreign national trekkers in the Nepal Himalaya who were better prepared, in terms of their understanding of AMS, were more likely to adhere to recommended ascent guidelines and experience fewer altitude-related illnesses (Vardy et al., 2005). However, within our study (which did not assess participants' understanding of AMS), approximately 90% of trekking groups included foreign nationals who had received or read information on altitude illness and acclimatization. Many medical problems are encountered spontaneously while trekking at high altitude. Some aspects of preparedness (such as knowledge of acclimatization and ascent guidelines) may help to reduce the risk of medical problems, and others, such as the presence of a comprehensive first aid kit or appropriate insurance, reduce their impact.
Conclusion
This study contributes to the limited literature on the preparedness and subsequent medical problems encountered by both Nepalese and foreign nationals at high altitude in the Nepal Himalaya. Foreign nationals should recognize that, as a consequence of socioeconomic differences, Nepalese staff and porters are often reliant on the preparedness and resources of the trekking group to reduce the risk of medical problems. Porters may be particularly vulnerable, even on a popular trekking circuit where medical facilities are available, since their lack of resources may mean the medical supplies carried by the group are their only access to health care. Furthermore, for an uninsured individual, the ability of a trekking group to pay for a helicopter or carry an individual to safety could be their only means of evacuation. Foreign nationals and Nepalese nationals in trekking groups have a duty of care towards each other; recognizing that trekking group preparedness relies not only on a comprehensive first aid kit, but also on knowledge of acclimatization and individuals' insurance that may contribute towards improving the health, safety, and welfare of individuals taking part in trekking activities in the Nepal Himalaya.
Author Disclosure Statement
The study was funded by an unrestricted educational grant from Medical Expeditions (registered charity number SC020922; www.medex.org.uk) and Porters Progress UK (registered charity no: 1112943; www.portersprogress.org).
Footnotes
Acknowledgments
The authors wish to thank Dr. Buddha Basnyat, Dr. Ghan Bahadur Thapa, and Dr. Matiram Pun, Institute of Medicine, Tribhuvan University, Kathmandu, for their support in setting up the study. We would also like to thank Sherpa Brothers (Sherpa Brothers Treks & Expeditions (P) Ltd, GPO, Box. No. 12731 Sundhara Kathmandu, Nepal; ![]() ) for their assistance in the field, and the Entwistle family, The Royal Society of Medicine, and Mr. Tony Drew for their funding contributions.
) for their assistance in the field, and the Entwistle family, The Royal Society of Medicine, and Mr. Tony Drew for their funding contributions.