
Abstract
Abstract
Brugger, Herman, Peter Paal, and Jeff Boyd. Prehospital resuscitation of the buried avalanche victim. High Alt. Med. Biol. 12:199–205.—In North America and Europe, approximately 150 people die of avalanches per year, and fatalities are presumed to be many times higher in developing countries. Four factors are decisive for survival: grade of burial, duration of burial, presence of an air pocket and a free airway, and severity of trauma. According to Swiss data, the overall mortality rate with avalanche burial is 23%, but it largely depends on the grade of burial. While the mortality rate is 52.4% in completely buried (head below the snow) victims in the Swiss population, it is only 4.2% in partially buried (head free) victims. Additionally, survival in completely buried victims drops to 30% within the first 35 min, initially due to death from lethal trauma, followed by asphyxia in 20–35 min. Thereafter, survival decreases more gradually and victims who are not fatally injured and are able to breath under the snow slowly succumb to hypoxia, hypercapnia, and hypothermia. In the absence of fatal injuries, rescue strategies depend on the duration of burial and the victim's core temperature. With a burial time <35 min, survival depends on preventing asphyxia by rapid extrication, adequate airway management, and cardiopulmonary resuscitation. With a burial time >35 min, tackling hypothermia is of utmost importance. Therefore, gentle extrication and continuous core temperature and electrocardiogram monitoring are recommended. Pulseless victims with a patent airway and a core temperature <32°C should receive uninterrupted cardiopulmonary resuscitation and be transported to a hospital with extracorporeal rewarming facilities.
Introduction
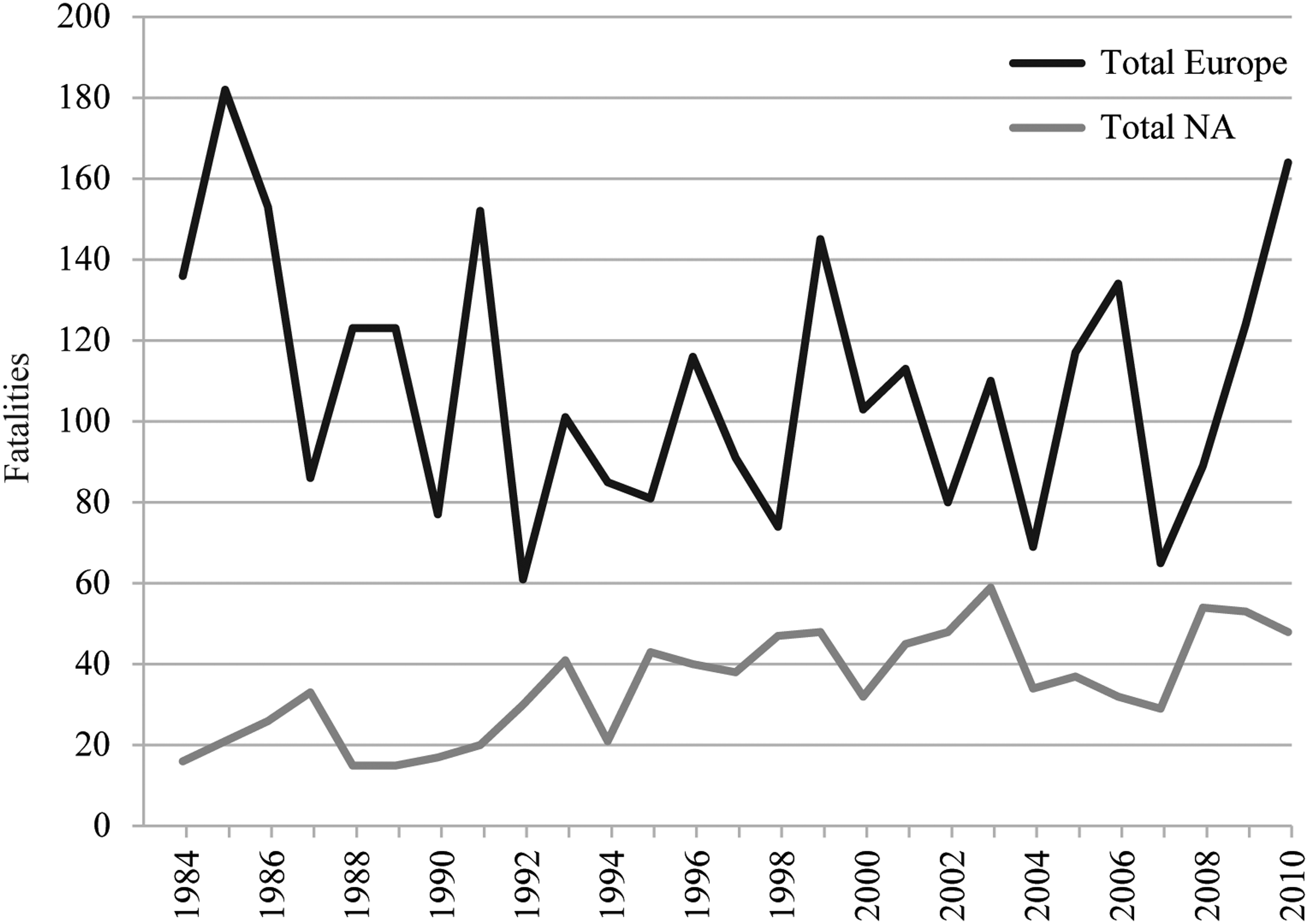
Yearly avalanche mortality in the European Alps and in North America (Etter, 2009).
Underlying Pathophysiology
The overall mortality rate of an avalanche accident is 23% (Brugger et al., 2001). Survival depends primarily on four factors: grade of burial, duration of burial, presence of an air pocket and a free airway, and severity of trauma.
Grade of burial
A Swiss analysis of avalanche accidents showed that the avalanche mortality rate was 52.4% for completely buried victims (i.e., head buried under snow), and only 4.2% for victims who were not buried or only partially buried (i.e., head free); the mean depth of complete burial was 1 meter (Brugger et al., 2001).
Duration of burial
For completely buried victims, survival is inversely related to the duration of burial whereby different phases can be identified (Falk et al., 1994; Brugger et al., 2001; Haegeli et al., 2011). In a recent study (Fig. 2) (Haegeli et al., 2011), survival probability in Switzerland remains higher than 80% up to 20 min postburial and drops to 30% at 35 min. The authors concluded that initially deaths are attributable to trauma, whereas the steep decline between 20 and 35 min is mainly due to asphyxia, which is the predominant cause of death from avalanches. After 35 min, survival decreases more gradually and victims who are not fatally injured and are able to breath under the snow slowly succumb to hypoxia, hypercapnia, and hypothermia. In contrast to Switzerland, survival in Canada declines significantly earlier and more steeply, but this is different across climate zones and suggests that the rate of asphyxia depends primarily on snow density, as suspected previously (Brugger et al., 2003).

Comparison of survival curves in Canada (black; n=301) and Switzerland (gray; n=946) from 1980 to 2005. Extracted from Haegeli P., et al. (2011).
Air pocket and hypothermia
In the last 50 years, Swiss and Austrian avalanche records have contained cases of survival after complete avalanche burial without sequelae in victims who presented a clearly visible air space in front of the mouth and nose upon extrication. From retrospective survival analyses, it was concluded that a patent airway is essential for survival longer than 35 min (Boyd et al., 2010; Soar et al., 2010; Vanden Hoek et al., 2010) and the presence of an air pocket distinguishes that the victim was able to breathe during burial and that prognosis is not unfavorable. In 2001, a human experiment demonstrated that during breathing into artificial air pockets in snow, hypoxia and hypercapnia occur with a concomitant respiratory and metabolic acidosis within a few minutes, and the degree of hypoxia depends on the volume of the air pocket, snow density, and unidentified individual characteristics (Brugger et al., 2003). The combination of hypoxia, hypercapnia (Grissom et al., 2000, 2004, 2008), and hypothermia was termed “triple H syndrome” (Brugger et al., 2003). The cooling rate during snow burial is still debated. Locher and Walpoth (1996) calculated a mean core cooling rate of 3.0°C/h for the overall time between avalanche burial and hospital admission, and estimated a maximum cooling rate of 8.0°C/h during the actual period of snow burial. In contrast, in an experimental study, Grissom et al. (2004) found a cooling rate as low as 0.7°C/h under normocapnic, and 1.2°C/h under hypercapnic conditions. Several studies found that increasing CO2 levels hasten cooling (Wagner et al., 1983; Johnston et al., 1996a,b) probably by suppressing shivering and by inducing vasodilation and increasing respiratory heat loss due to evaporation from hypercapnia-induced hyperventilation. Furthermore, hypoxia increases the core temperature cooling rate (Johnston et al., 1996b). Recently, cooling rates of 6°C/h (Putzer et al., 2010) and 9°C/h (Oberhammer et al., 2008) have been reported, which is comparable to a recent experimental study in pigs (Brugger et al., 2010a; Paal et al., 2010). Thus, the cooling rate of avalanche victims varies widely, and rapid cooling of up to 9°C/h may occur. This implies that hypothermia with a core temperature <35°C becomes important soon after snow burial in some victims.
Trauma
The percentage of avalanche victims who die from fatal trauma is variable. Hohlrieder et al. (2007) retrospectively reviewed clinical and radiological findings between 1996 and 2005 in Austria. Of the 105 avalanche victims, 78 (74.3%) had minor injuries (Injury Severity Score, ISS <8), 18 (17.1%) moderate (ISS 8-13), 2 (1.9%) severe (ISS 14-20), and 7 (6.7%) critical (ISS >20), primarily on extremities, chest, and spine. Two of 36 (5.6%) fatalities were attributable solely to trauma, both with dislocated cervical spine fractures. In contrast, Boyd et al. (2009) reviewed 204 coroner's reports of avalanche fatalities in western Canada between 1984 and 2005 and found trauma as the single immediate cause of death in 48 (24%) cases, with a median ISS of 30 in trauma deaths and an ISS exceeding 15 in 13% of asphyxia deaths. Both severity of injuries and trauma mortality, which varies between 5% and 24%, are highly dependent on the topography of the terrain (e.g., rocky, forested) and snow composition (e.g. heavy, wet) (Haegeli et al., 2011).
Causes of death
Table 1 shows the cause of death in 296 avalanche fatalities, diagnosed postmortem with autopsy or full external examination in Canada, USA, and Austria (Hohlrieder et al., 2007; McIntosh et al., 2007; Boyd et al., 2009). Asphyxia remains the most important cause of death, but trauma mortality is increasingly important. Based on autopsy reports, hypothermia seems to play a negligible role as the sole cause of death in avalanche victims. However, hypothermia alone or in combination with asphyxia is difficult to identify solely by external examination or autopsy (Brugger et al., 2009a) and may be underestimated. In most cases, hypothermia is associated with asphyxia and trauma and thus prognosis is much poorer when compared to hypothermia from environmental exposure.
Treatment Recommendations
Aid by first responders
Avalanche survival is strongly time dependent. Depending on the characteristics of snow climate, the onset of asphyxia is between 10 and 20 min after burial (Fig. 2). Search and excavation should be initiated as promptly as possible after avalanche release as every minute is crucial for survival in this early stage. As soon as the head of a victim is free, airway management and conventional CPR, including rescue breaths, should be started if the victim is not breathing. Although the 2010 Adult Basic Life Support guidelines encourage hands-only (chest compression only) CPR for the untrained lay-rescuer, they also recognize that combined CPR is an important component for successful resuscitation from asphyxial cardiac arrests in adults (Berg et al., 2010; Nolan et al., 2010). After excavation, the victim's body should be insulated from the cold. A victim should be wrapped in available materials, such as aluminum blankets, jacket, raincoat, bivouac bag, hat, and gloves.
Organized rescue
An avalanche accident is a medical emergency that should prompt, if available, a helicopter rescue operation; however, the risk incurred by the rescue team should be weighed against the expected benefit to the victim. Since the probability of survival decreases over time, it may be justifiable to take greater risk soon after the accident, but less risk after longer burials. The staff should be dressed warmly with complete winter equipment, including avalanche safety devices, with a transceiver and ideally an airbag. Airbags offer protection on approach as well as on scene. All medical equipment should be protected from the cold, and electronic instruments prepared with full batteries. Rescue bags should include blankets or similar insulation, aluminized wraps, chemical heat packs, thermometers suitable for core temperature reading, and cardiac monitoring devices. Standard guidelines have been introduced for the field management of avalanche victims by the International Commission for Mountain Emergency Medicine ICAR MEDCOM (Brugger and Durrer, 2002) and the International Liaison Committee for Resuscitation ILCOR (Soar et al., 2010; Vanden Hoek et al., 2010).
CPB, cardiopulmonary bypass; CT, core temperature.
Use core temperature if duration of burial is unknown.
Basic Life Support, Advanced Life Support according to international guidelines.
Cardiopulmonary Bypass or Extracorporeal Membrane Oxygenation.
Transport to the nearest hospital for serum potassium measurement if hospitalization in a specialist unit with extracorporeal rewarming facilities is not logistically possible. If K+ exceeds 12 mmol/L, resuscitation should be terminated (unless depolarizing neuromuscular blocking agents were used); if K+ is ≤12 mmol/L, continue CPR and transport the patient to a specialist hospital for extracorporeal re-warming. PEA, pulseless electrical activity; PVT, pulseless ventricular tachycardia; VF ventricular fibrillation.
If burial duration exceeds 35 min, a patent airway is essential for survival and combating hypothermia assumes paramount importance. The Swiss staging system of hypothermia (Durrer et al., 2001) is based on clinical signs—clear consciousness and shivering (stage I), impaired consciousness without shivering (stage II), unconsciousness (stage III), and not breathing (stage IV)—and can be used by nonmedical members of the rescue team at the scene.
Monitoring
A core temperature of 32°C is proposed as the limit between the ‘safe’ and ‘danger’ zones for the risk of cardiac arrhythmias (Matz, 1986). Early measurement of the core temperature is therefore indispensable since the level of consciousness varies widely among patients at a given core temperature due to concomitant asphyxia. The gold standard for core temperature reading is the measurement in the lower third of the esophagus. In the prehospital setting, this is the most reliable location for core temperature monitoring, but it is attainable only in intubated patients (Brugger et al., 2009b). If the patient is responsive, epitympanic measurement is an alternative (Walpoth et al., 1994). Only thermistor-based, not infrared-based, ear thermometer readings correlate well with the core temperature in a cold environment (Locher et al., 1997). However, the epitympanic temperature may still be erroneously lower than the esophageal temperature in the case of a cold environment, poor placement (and therefore insulation) of the probe, blockage of the external auditory canal, or circulatory arrest and reduced carotid artery flow.
Cardiac monitoring should be initiated prior to transport to detect arrhythmias provoked by movement of the patient. As standard electrodes may not work on cold skin, needle electrodes may be useful, which can be improvised by puncturing standard electrodes and the skin with a thin injection needle (Weinberg, 1993). Pulse oximetry may be unreliable in hypothermic patients due to peripheral vasoconstriction, but still indicates the correct saturation as long as the peripheral pulse rate corresponds to the heart rate on the ECG monitor (Striebel et al., 1988).
Stage I: Patient alert and shivering
If the patient is responsive, wet clothing is removed and replaced with dry insulating material and the patient is permitted to walk. Exercise rewarms a person more rapidly than shivering, but may increase afterdrop (Giesbrecht and Bristow, 1997; Grissom et al., 2008). Warm, sugar-containing, nonalcoholic drinks may be given providing swallowing is possible. The alert patient without an arrhythmia and with normal blood pressure may be transported to the nearest hospital for observation.
Stages II–III: Patient somnolent or comatose but breathing
The three guiding principles for prehospital management of a somnolent or comatose hypothermic patient should be followed: (1) adequate oxygenation, (2) careful handling, and (3) full body insulation. Unconscious victims have a low threshold for developing ventricular fibrillation (VF) (Danzl, 1994) and require careful handling during rescue and transport. Gentle handling is a priority over speed during extrication, and patients should be kept horizontal to avoid afterdrop and postrescue collapse due to arrhythmias. Although it is not always possible to avoid rough movements, movements of the limbs and trunk should be carried out slowly and with great care (Kornberger and Mair, 1996). Full body insulation and application of hot packs are part of the standard prehospital treatment for hypothermia to prevent further heat loss in the prehospital setting. The application of external heat to the trunk is particularly helpful when shivering ceases. Insulation should be applied and the patient placed in the recovery position if unconscious and if the airway is not secured. Cardiac and core temperature monitoring should be established as soon as possible. Adequate oxygenation is essential to stabilize the myocardium in the hypothermic patient (Danzl, 1994). Thus, nonintubated patients should receive supplemental oxygen with a facemask or nasal cannula. If the patient is not responsive, the airway should be protected by endotracheal intubation or a supraglottic airway (Deakin et al., 2010a; Morrison et al., 2010). With low core temperature drug metabolism is decreased and anesthesia and neuromuscular blockade are prolonged (Caldwell et al., 2000; Heier and Caldwell, 2006; Leslie et al., 1995). Depolarizing neuromuscular blocking agents (e.g., succinylcholine) should be avoided as they can affect triage decisions by increasing the serum potassium level (see below). Prolonged diagnostic and treatment procedures should be avoided to prevent further heat loss. Victims with severe hypothermia should be transported to a hospital with an intensive care unit experienced in hypothermia care. In the field, aggressive volume replacement is contraindicated as cardiac output is reduced and the circulating volume contracts due to peripheral vasoconstriction (Lloyd, 1992). In a cold environment, infused fluids should be warm (∼42°C), although this may be difficult. In patients with a core temperature <30°C, the administration of advanced life support drugs is controversial and may be withheld (Soar et al., 2010; Vanden Hoek et al., 2010). Notably, epinephrine may worsen peripheral circulation and exacerbate frostbite.
Stage IV: Patient not breathing
Avalanche victims in cardiorespiratory arrest with a patent airway and core temperature <32°C are best managed optimistically by rewarming in a hospital with extracorporeal rewarming capability, where available. Detecting signs of life may be difficult in severely hypothermic patients as respirations and pulses may be very slow, irregular, and small-volume. Vital signs in hypothermic victims should therefore be checked for up to 1 min rather than the 10 sec recommended for normothermic victims. Any avalanche victim with a patent airway who presents with hypoventilation or apnea, arrhythmia, systolic blood pressure <80 mmHg, pulseless electrical activity (PEA), VF, or asystole should ideally be transported directly to a center offering extracorporeal rewarming (Farstad et al., 2001; Ruttmann et al., 2007; Vretenar et al., 1994; Walpoth et al., 1997). It is advisable to contact the destination hospital in advance to ensure the availability of an extracorporeal rewarming unit. Early CPR improves the survival of an arrested hypothermic patient, even when continued for a prolonged period (Larach, 1995). A case of full recovery in a severely hypothermic patient after six and a half hours of CPR has been reported (Lexow, 1991). The rate of chest compressions and ventilation should be the same as standard basic life support (BLS) with minimal interruptions. Performing continuous manual chest compressions with minimal hands-off time during ground transport is not possible and may be difficult even during helicopter transport. Mechanical chest compression devices should be considered for long and difficult transports, where rescuer fatigue may impair the effectiveness of manual chest compressions, to guarantee optimal CPR (Deakin et al., 2010b). With a core temperature <30°C, VF may or may not respond to defibrillation. Despite this, it may be reasonable to repeat defibrillations (Vanden Hoek et al., 2010), but these might be limited compared to normothermic victims and a delay in transport should be avoided. It should be emphasized that if defibrillation attempts are not successful, CPR must be continued until extracorporeal rewarming has raised the core temperature to >30°C (Soar et al., 2010; Vanden Hoek et al., 2010). With avalanche victims, hyperkalemia is an important outcome marker (Boyd et al., 2010; Locher et al., 1991; Mair et al., 1994; Schaller et al., 1990). Hyperkalemia indicates that cardiorespiratory arrest from acute asphyxia occurred before cooling. There is evidence that in avalanche burial with hypothermia, serum potassium >12 mmol/L is sufficient to justify cessation of CPR. A serum potassium <8 mmol/L is a positive prognostic marker for return of spontaneous circulation (ROSC) (Mair et al., 1994). The highest admission serum potassium in an avalanche victim in cardiac arrest who survived to hospital discharge was 6.4 mmol/L (Locher and Walpoth, 1996). However, a nonavalanche-associated case of survival has been reported in a hypothermic child with an initial potassium of 11.8 mmol/L (Dobson and Burgess, 1996). The international CPR guidelines 2010 proposed two thresholds for serum potassium—8 mmol/L in adults (Morrison et al., 2010) and 12 mmol/L in all avalanche victims regardless of age (Soar et al., 2010). If transport to a unit with extracorporeal rewarming facilities is not readily available, the serum potassium at the nearest hospital may be used as an additional prognostic marker.
Prognosis
The lowest recorded core temperature from which a person with accidental hypothermia has been successfully resuscitated is 13.7°C (Gilbert et al., 2000). In avalanche victims, the nadir is 19°C (Althaus et al., 1982). The numerous case reports of long-term survivors with full neurologic recovery after severe hypothermia give every reason to treat hypothermic patients optimistically (Walpoth et al., 1997). Attempts at resuscitation are not indicated if the cause of cardiac arrest is clearly attributable to a lethal injury or asphyxia, if the chest and abdomen are incompressible, or if transport with continuous CPR would endanger the rescuers. In all other cases the guiding principle for avalanche victims should be “no hypothermic avalanche victim with a patent airway is dead until warm and dead.”
Footnotes
Acknowledgments
We thank Emily Procter for the help in editing the manuscript and figure drawing.
Author Disclosure Statement
HB has published studies on avalanche resuscitation; no financial conflict of interest. PP and JB have no financial or other conflict of interest.