
Abstract

Wednesday, Feb. 16, 2011
After brief introductions and announcements, the scientific symposium started Wednesday morning with a session on the role of hypoxia in cancer biology, chaired by Max Gassmann (Zurich). Joachin Fandrey (Essen, Germany) described the hypoxia inducible factor (HIF) complex, including the oxygen-regulated alpha protein along with the constitutive production of the beta subunit. In their laboratory, fluorescence resonance energy transfer (FRET) is used to calculate the distance between the alpha and beta subunits of the HIF complex bound to DNA. This FRET analysis provides new information about the compact three-dimensional structure of the HIF complex in living cells (Wotzlaw et al., 2007). Following this introduction, Amato Giaccia (Stanford, CA) described the implications of tumor hypoxia and novel cancer therapies. Several studies suggest that hypoxia increases metastases and/or the metastatic potential of a tumor (Le et al., 2004; Young et al., 1988). During the question and answer session, a discussion ensued about the role of hypoxia in stimulating cancer. Despite concerns that hypoxia increases tumor metastases, the suggestion was made that there is little evidence of increased cancer rates in populations living at high altitude except for skin cancer related to high UV exposure. This interesting suggestion was recently confirmed (Ezzati et al., 2011).
The next talk discussed the multiple complex pathways involved in cerebral blood flow regulation. Grant Gordon (Calgary, Alberta) discussed his recent work showing how astrocytes control cerebral blood flow (Gordon et al., 2007). Increased intracellular calcium in astrocytes can cause constriction as well as dilation of neighboring blood vessels through the production of arachidonic acid. Conversion of arachidonic acid to 20-hydroxyeicosatetraenoic acid causes vessel constriction, whereas conversion to prostaglandin E2 (PGE2) induces dilation. The metabolic state of the brain tissue and the level of nitric oxide dictate which pathway is utilized. When oxygen availability is low, vasodilation occurs; conversely when oxygen availability is high, vasoconstriction results (Gordon et al., 2008). Gordon's presentation was augmented by the use of real-time in vivo imaging techniques demonstrating uncaging of Ca2+ by UV stimulation causing vasoconstriction. Gordon's experiments demonstrated how hypoxia increases extracellular adenosine inhibiting Ca2+ release leading to vasodilation. These experiments also demonstrated how hypoxia increases lactate, inhibiting PGE2 transport, leading to increased extracellular PGE2 and vasodilation.
The first poster session was held Wednesday afternoon after the ski break. The following are a tiny sample of the many great posters. Suzy Stokes (Leicester, UK) conducted a study of the feasibility of establishing a diploma in mountain medicine in Nepal. Although significant financial barriers remain, responses from within Nepal and the wider mountain medicine community were uniformly positive. An initial course tailored to the needs of Nepalese physicians (but also open to international applicants) is planned in the Fall of 2011. To review the summary report and details of how to become involved, please visit www.medex.org.uk. Vincent Tedjasaputra (San Diego, CA) presented a poster on the effects of exercise on specific ventilation heterogeneity using oxygen-enhanced MRI techniques. Specific ventilation (SV) is the ratio of the volume of fresh air entering a lung region to that region's end-expiratory volume. Unlike perfusion heterogeneity which is known to increase (presumably because of interstitial edema), they found no significant increase in SV with exercise. These results suggest that increased VA/Q inequality during exercise is due to changes in distribution of perfusion that are not matched by ventilation.
David Dubowitz (San Diego) and colleagues presented data on cerebral diffusion, edema, and metabolism using brain MRI techniques in subjects with AMS. Symptoms of uncomplicated AMS overlap with those of cerebral edema, suggesting a common etiology. Whether hypoxia causes a vasogenic or a cytotoxic edema is unclear. Using subjects exposed to 3800 m at White Mountain, CA, no cytotoxic edema was found, but vasogenic edema of basal ganglia and splenium was seen. In a second poster from this same group, cerebral O2 metabolism assessed by MRI was increased after 2 days of sustained hypoxia (3800m) despite the reduced oxygen availability. This was true whether the subjects developed AMS.
The evening programs at Hypoxia are highlights of the meetings and this year was no exception. After dinner in the spectacular Victoria Dining room at the Chateau, Zoe Hart, an American climber, regaled us with stories and pictures of from her “Adventures and Miss-adventures in the life of an Alpine Princess”. Zoe is an American climber living in Chamonix and certified by the International Federation of Mountain Guides Association. Complete with her usual pink jacket, Zoe climbs all kinds of routes although alpine climbs are her real passion.
Thursday, Feb. 17, 2011
Thursday morning began with a series of talks on how the adrenergic nervous system adapts to hypoxia. This was followed by a session about the causes and consequences of sleep-induced periodic breathing. Jerry Dempsey (Madison, WI) spoke on the pathogenesis of periodic breathing (PB). PB commonly occurs in patients with chronic heart failure, with chronic opioid use, in some types of obstructive sleep apnea, and in hypoxic environments. The prevalence of sleep-disordered breathing varies but may occur in 2%–9% of middle-aged adults up to 10%–15% in older adults. Central and peripheral chemoreceptors, airway narrowing, and unstable sleep state (e.g., transient arousals) all contribute to ventilator instability, leading to sleep apnea. Nonrapid eye movement sleep (NREM) causes decreased motor output to the upper airway and to respiratory muscles, leading to hypoventilation and 2–8 mmHg increase in PaCO2 (Dempsey, 2005; Dempsey et al., 2004). With heart failure, multiple factors contribute to unstable breathing, including increased chemoreceptor activity, increased circulation time, and increased pulmonary vascular pressures. The engineering concept of “loop gain” was discussed in detail in its application to central respiratory regulation within narrow variations of PaCO2.
Dr. Dempsey's talk was followed with one by Shahrokh Javaheri (Cincinnati) on the consequences and treatment of periodic breathing in chronic heart failure. Central sleep apnea (CSA) in heart failure has a very regular breathing pattern, whereas CSA induced by opiates has a much less regular pattern. Oxygen administration, heart transplantation, acetazolamide, and theophylline all improve CSA in heart failure. In a recently published study, Dr. Javaheri found that only a small fraction of patients with newly diagnosed heart failure were suspected of having CSA. But those who were tested for sleep apnea and treated for it when present; survival was significantly improved (Javaheri et al., 2011).
On Thursday afternoon, Peter Bartsch and Annaluisa Cogo chaired the first Hot Topics session. Paul Robach, Christoph Siebenmann, and colleagues (Chamonix and Zurich) reported the effects of “Live High—Train Low” (LHTL) on V
Megan Wilson (Aurora, Colorado) presented data on gene expression signatures in AMS. Although AMS is the most common form of illness in those traveling to high altitude, the underlying mechanisms remain unclear. Megan Wilson and colleagues exposed 24 subjects to simulated altitude in a hypobaric chamber for 10 hours and analyzed gene expression in peripheral mononuclear blood cells before and after exposure. They evaluated massive datasets of transcripts for both altitude and AMS associations utilizing a variety of sophisticated mathematical filtering tools. In the end, six genes were isolated out of 47,000 transcripts that were predictive of AMS with 98% accuracy. These genes are found in the hypoxia sensing, angiogenic, and inflammatory pathways. We are eagerly awaiting prospective studies to validate these findings which hold promise in predicting individuals susceptible to AMS and providing additional insight into underlying mechanisms.
Tom Hornbein (Estes Park, Colorado) over the years has suggested the names of many of the evening speakers to Peter and Rob. Dawn Sumner (Davis, CA) continued this wonderful tradition speaking to us about the “Geologic History of Atmospheric Oxygen.” Dawn has spent several seasons studying cyanobacteria in ice-covered lakes in Antarctica. Complete with Antarctic pictures and fascinating preliminary data, she showed how atmospheric oxygen has changed over long periods of time.
Friday, Feb. 18, 2011
The morning sessions focused on epigenetics and cancer. Impaired apoptosis and excessive proliferation of pulmonary artery smooth muscle cells (PASMC) contributes to vascular obstruction in pulmonary arterial hypertension (PAH) patients. Stephen Archer (Chicago) described recent work in his laboratory on reduced mitochondrial superoxide dismutase-2 (SOD2). SOD2 is reduced in both patients with PAH and a Fawn-hooded rat (FHR) model of PAH impairing hydrogen peroxide signaling. Downregulation of SOD2 using siRNA produces a PAH phenotype in normal PASMCs. In the FHR model of PAH, portions of the SOD2 genetic loci demonstrated Hypermethylation, suggesting an epigenetic heritable abnormality. This methylation could be reversed with restoration of SOD2 expression and correction of the proliferation/apoptosis imbalance in PASMCs. Methylation-induced attenuation of SOD2 expression represents a novel epigenetic mechanism of PAH that may explain part of the cellular proliferation and decreased apoptosis seen in PAH. This could also lead to new therapeutic approaches to PAH (Archer et al., 2010).
After the mid-day ski break the second poster session of approximately 40 posters was held. Jim Milledge, Nick Talbot, Edith Kortekaas, and Dan Martin presented pilot data from the Margherita Hut evaluating the pulmonary vascular response to supplemental oxygen following ascent to altitude. Some time between 30 min and 8 h of hypoxia, supplemental oxygen does not restore pulmonary pressures to normal sea level values. These findings early in the course of hypoxia suggest that vascular remodeling alone cannot be the sole cause of the failure of supplemental oxygen to reverse hypoxic pulmonary vasoconstriction. Mary Slingo (Oxford, UK) evaluated performance of a visual analogue scale for assessment of AMS in adolescents during two expeditions to Ladakh. More than 75% of subjects aged ∼17.5 years preferred the VAS to the Lake Louise Score (LLS). The VAS was a reliable and user-friendly alternative to the LLS for use among adolescents.
Many, if not most, attendees at the Hypoxia Symposium are familiar with the history of climbing on Mt. Everest, yet it holds a fascination unlike most other adventure stories. Jake Norton participated in the 1999 expedition to the north side of Mt. Everest when the body of George Mallory was found. Jake recounted these events with slides and film in his talk “Lost on Everest: The Enduring mystery of Mallory and Irvine”. Once again we relived the compelling story from over three quarters of a century ago—mysteries that never grow old.
Saturday, Feb. 19, 2011:
One of the themes running throughout the Symposium was that of HIF-1α and its role in cancer. Jacques Pouysségur (Nice, France) is at the forefront of some of the work on the role of oxygen sensing in energy metabolism and vasculogenesis. Professor Pouysségur presented work from his laboratory showing how tumor hypoxia and metabolism can lead to novel approaches to cancer treatment (Brahimi-Horn et al., 2011; Pouyssegur et al., 2006). HIF controls a vast array of gene products controlling glycolysis, intracellular pH angiogenesis (e.g., VEGF-A and angiopoietin-2), and cell migration and invasion. This hypoxia-signaling pathway is a strong promoter of tumor growth and HIF expression and has been associated with poor patient prognosis in some cancers as shown in Figure 1 (Semenza, 2010; Trastour et al., 2007). The HIF-regulated carbonic anhydrase isoforms IX and XII are induced by hypoxia and promote tumor cell survival and growth by helping maintain normal intracellular pH. These membrane-bound carbonic anhydrase isoforms represent important new targets for cancer therapies (Chiche et al., 2009). An unexplained paradox is how HIF expression or activation in the setting of cancer leads to substantially worse clinical outcomes whereas HIF activation on ascent to altitude augments the acclimatization process without inducing tumors.
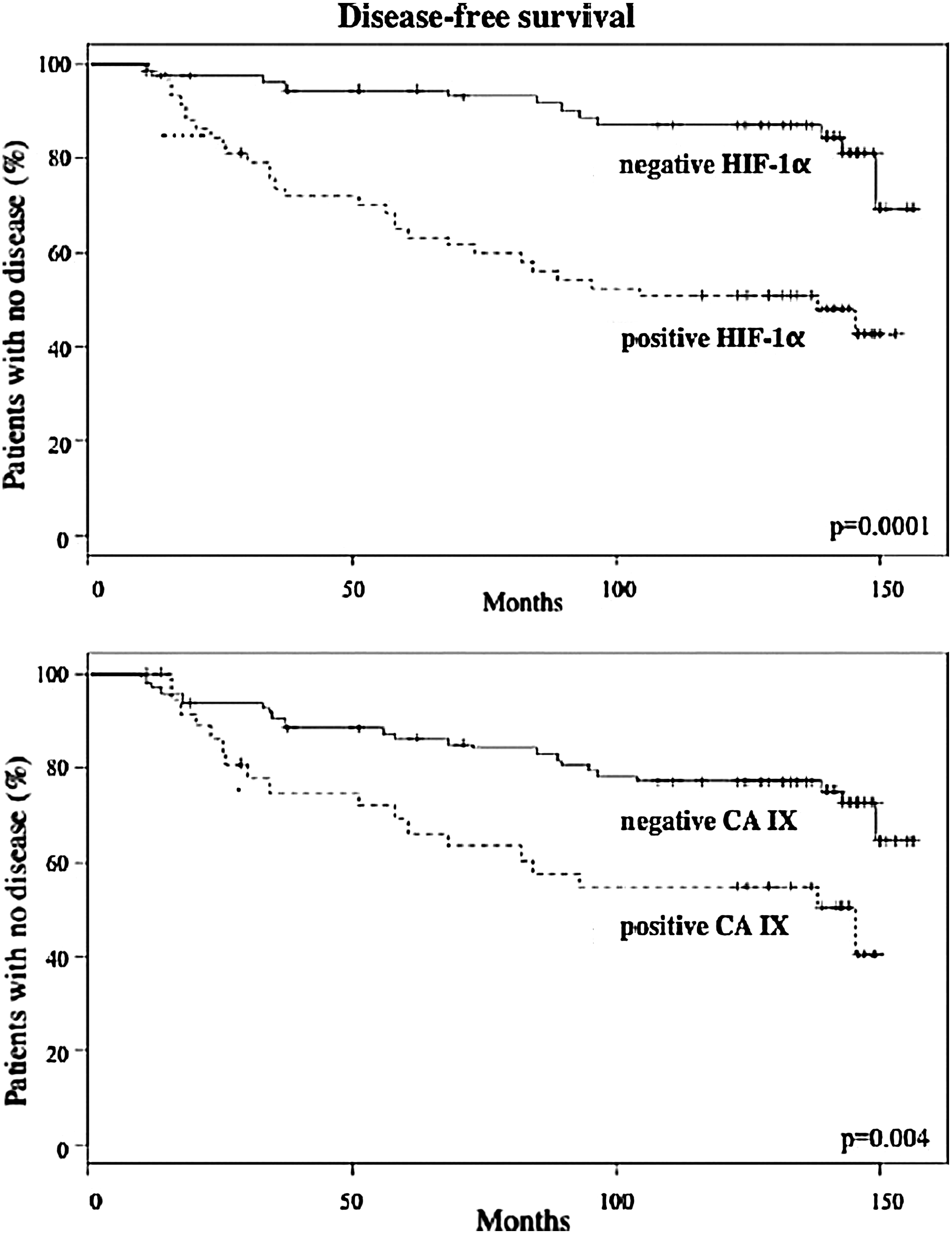
Kaplan-Meier survival curves of the disease-free survival in 132 breast cancer patients based on expression of HIF-1α in the tumors (top panel) or expression of carbonic anhydrase IX (CA IX), (bottom panel). © 2007 Wiley. Used with permission from Trastour C, et al., HIF-1alpha and CA IX staining in invasive breast carcinomas: prognosis and treatment outcome. Int J Cancer 120, 1451-8 (Trastour et al., 2007).
From cancer and hypoxia the session shifted to history. This year is the 100th anniversary of the Anglo-American Pikes Peak Expedition. John West (San Diego) traced the importance of this expedition and its influence on our understanding of how altitude affects human physiology. The principal figures in the expedition were J.S. Haldane, C.G. Douglas, Y. Henderson, and E.C. Schneider. They made extensive measurements of alveolar gas and blood partial pressures on the summit of Pikes Peak (4302 m) as well as collecting data on other aspects of cardiovascular physiology. The main physiological findings were published in a remarkable 134 page report of the expedition (Douglas et al., 1913). Mabel Fitzgerald, unable to join the men unchaperoned, participated in the expedition by collecting alveolar gas samples at various Colorado mining camps at altitudes ranging from about 1500 m to 4300 m (Fitzgerald, 1913). She collected over 500 alveolar gas samples on men and women aged 15–70 years, showing that alveolar PCO2 falls as altitude increased. Her data continues to be used and supports our current understanding of the hyperventilation following ascent to altitude.
After the morning refreshment break, Erik Swenson (Seattle, WA) gave an update on hypoxia and its acid-base consequences: from mountains to malignancy. Both alkalemia and acidemia affect responses to hypoxia. For example, the respiratory alkalosis associated with ascent to altitude decreases sympathetic nerve activity and cerebral blood flow. HIF is activated by hypoxia but may also be activated during normoxic acidosis by the pH-dependent nucleolar sequestration of the von Hippel-Lindau (VHL) factor, thus preventing the degradation of HIF (Mekhail et al., 2004). HIF activation also modulates the hypoxic pulmonary vasoconstrictor response (Wang et al., 2006). During normoxic exercise, lactate production does not equate with cellular hypoxia but is largely driven by catecholamines (Richardson et al., 1998). Finally, in sepsis or septic shock, lactate does not necessarily indicate tissue hypoxia. Rather, the lactate largely results from aerobic glycolysis through stimulation of cell membrane ion pumps such as Na+-K+-ATPase (Levy et al., 2005). We were left with three principles about acidosis in the ICU: 1) acidosis may help protect cells, 2) reduce the urge to play chemist by always normalizing the pH, and 3) treat the underlying disorder, not the pH.
Hot Topics in Mountain Medicine, Saturday afternoon
Kara Beasley (Eugene, Oregon) presented the results from her work in Andrew Lovering's laboratory at the University of Oregon on right-to-left shunting through hypoxia-induced intrapulmonary arteriovenous anastomoses. Study subjects breathed four different FIO2 concentrations (30 min each) and right-to-left shunt was semi-quantitatively categorized using an echocardiographic contrast (agitated saline bubbles) density and distribution score (0–5) within the left ventricle. Nearly all study subjects fell into one of two categories, desaturators and non-desaturators after breathing a hypoxic gas mixture with an FIO2 of 0.1. The desaturators had an O2 saturation of 63.0% whereas the non-desaturators had an O2 saturation of 76.2%. The desaturators had a bubble score of 2 with an O2 saturation of 93.8% and the non-desaturators only achieved the same bubble score at an O2 saturation of 85.3%. Kara suggested that bubble scores with mild hypoxia could identify individuals who would become desaturators with more severe hypoxic exposure and thereby more likely to suffer from high altitude related illness. Three variables are being considered: FIO2, O2 saturation (pulse oximetry), and right-to-left shunting (bubble score). The significance of these shunts is the subject of much debate. Some investigators contend that the degree of right-to-left shunting associated with progressive degrees of hypoxia is physiologically trivial. For an excellent overview of this debate, please see the “point:counterpoint” feature in J Appl Physiol 107:993–998, 2009.
Before presenting data from diving birds and mammals, Jessica Meir (Vancouver, BC, Canada) briefly told the audience about her current work with juvenile bar-headed geese. These geese migrate biannually over the Himalayan Mountains and have even been spotted over the summit of Mt. Everest (8850 m). Dr. Meir is training these birds to fly in a wind tunnel where they will obtain in-flight physiologic data under both normoxic and hypoxic conditions (see http://www.nsf.gov/discoveries/disc_summ.jsp?org=NSF&cntn_id=118659). Dr. Meir then shifted from hypoxia at high altitude to hypoxia in diving mammals and presented her data from emperor penguins and elephant seals (Meir et al., 2009; Meir and Ponganis, 2009). The mechanisms these birds and mammals use to achieve their impressive underwater foraging (to depths of 564 m and durations over 23 min in emperor penguins, and 1581 m and 119 min in northern elephant seals) are varied and incompletely understood (Meir and Ponganis, 2010; Ponganis et al., 2010). Recent work by Meir and colleagues suggest that depletion of oxygen stores in diving emperor penguins are primarily regulated by heart rate, with rates down to 3–6 beats per min (Meir et al., 2008; Ponganis et al., 2010). In northern elephant seals, other researchers have proposed that hypothermia might be a way to suppress metabolism, allowing for prolongation of dives. Direct blood temperature recordings, however, did not support this hypothesis (Meir and Ponganis, 2010). Instead, it is the recently documented extreme hypoxemic tolerance of the elephant seal that likely contributes to their remarkable diving capacity (Meir et al., 2009). Not surprisingly, this fascinating presentation received the first place award for the resident/fellow category.
The highlight of the final evening of the Symposium was the usual banquet dinner and dance along with presentation of awards. The Reeves Prize is awarded at the biennial International Hypoxia Symposium to the speaker judged to present the most outstanding scientific talk, with special emphasis on presentation skills focusing on clarity that were cherished, taught, and practiced by the late Professor John “Jack” T. Reeves (Moore and Grover, 2006). The evaluation criteria include whether the material is new, interesting, and important. This year's Reeves prize was split between Jacques Pouysségur and Grant Gordon. Space precludes inclusion of many other excellent presentations and posters. To paraphrase John Sutton's remarks at the conclusion of earlier Symposia, this was the best Hypoxia Symposium ever. We look forward to the 18th Symposium at Chateau Lake Louise during the full moon in early 2013.