
Abstract
Abstract
Degache, Francis, Gabriele Larghi, Raphael Faiss, Olivier Deriaz, Gregoire P. Millet. Hypobaric versus normobaric hypoxia: same effects on postural stability? High Alt. Med. Biol. 13:40–45.—
Introduction
Combinations of barometric pressure (PB) and inspired fraction of oxygen (FIO2) that result in any inspired pressure of oxygen (PIO2) less than a normoxic value of 150 mmHg is by definition hypoxic (Conkin and Wessel, 2008). The fact that the physiological responses might be slightly different between hypobaric hypoxia (HH; FIO2=20.9%; PB<760 mmHg) and normobaric hypoxia (NH; FIO2<20%; PB∼760 mmHg) has been reported but remains debated (Loeppky et al., 1997; Savourey et al., 2003). For example, the ventilatory responses at rest were shown to be slightly different (breathing frequency, FETO2 and FETCO2 were higher but minute ventilation was lower) in HH than NH (Savourey et al., 2003). With the recent development of hypoxic training methods combining “real” (HH) and “simulated” (NH) altitude (Millet et al., 2010), it is important to further investigate whether HH and NH induce noticeable different physiological responses. Regarding postural stability, it is well known that the vestibular system is altered by hypobaric hypoxia through multiple mechanisms (Nordahl et al., 1998; Singh et al., 1976). A deficient vestibular system often results in an altered postural stability. However, in HH, vision is the first of the special sense to be altered in hypoxia (DeHart, 1996).
Several studies using static platform posturography have shown decrements in postural stability in HH (Baumgartner and Bartsch, 2002; Baumgartner et al., 2002; Cymerman et al., 2001; Nordahl et al., 1998); for example, sway is increased in HH compared to baseline value, more in the antero-posterior than lateral direction (Fraser et al., 1987; Holness et al., 1982; Nordahl et al., 1998) for healthy subjects as well as in subjects prone to acute mountain sickness (Baumgartner et al., 2002; Cymerman et al., 2001). The results of these studies suggest that PB has a significant effect on postural stability. In NH at 4300 m, a lower stability was observed after 3 h of exposure (Cymerman et al., 2001). However, to our knowledge, comparison of the effects of HH and NH on the postural stability has not been reported. The aim of this study was therefore to compare the changes in postural stability parameters during acute HH and NH exposures in healthy subjects.
Materials and Methods
Subjects
Twelve healthy males (age: 24.7±6.4 years, height: 178±4 cm, weight: 76.0±9.7 kg) participated in this study. No participant had any history of neural disorder. All volunteers were low altitude residents (380–500 m) and they had no significant altitude exposure at least one month prior the experiment. The study was approved by the local Medical Ethics Committee (CCVEM007/10, Sion, Switzerland) and written informed consent was obtained from each participant after explaining the experimental procedures and possible risks.
Experimental design
The experiments were conducted in two separate trials for two groups of six subjects (Group A and Group B). The experimental design and values of PB, FIO2, and PIO2 for each trial are shown in Figure 1. Normoxic normobaric (NN) measurements were performed in a well-ventilated laboratory outside the hypoxic chamber at an altitude of 480 m. (NN, PB 720±2 mmHg, FIO2 20.9±0.1 %, 24±1°C; Sion, Switzerland). The HH experiments were conducted at 1700 and at 3000 m (HH1700 and HH3000; Fig. 1). The NH sessions were realized in a hypoxic chamber (SL–400, ATS, Sydney, Australia), which is a well-ventilated 30-m3 room (2.4 m x 5.0 m x 2.5 m) with transparent glass panels. The hypoxic system allows sufficient hypoxic air input flow (up to 1000 l/min) in order to obtain a continuously stable FIO2. Measurements at altitude were made at 1700 and 3000 m (NH1700 and NH3000; Fig. 1). PB was measured at these altitudes using a validated hand-held digital barometer (GPB 2300, Greisinger Electronic, Regenstauf, Germany). This barometer had a precision of±2.0 mbar (temperature: 0°–50°C).
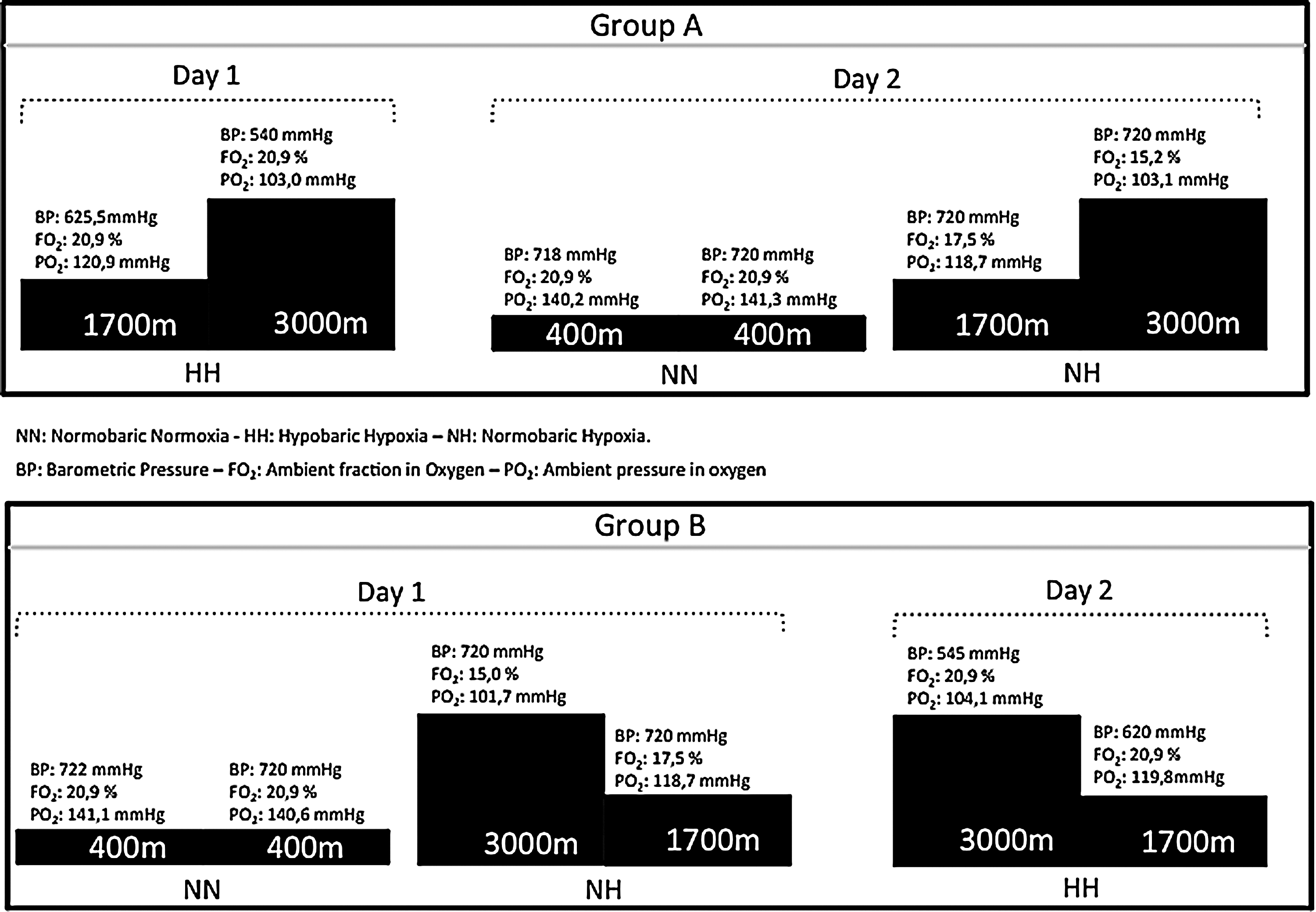
Study design. NN, normobaric normoxia; HH, hypobaric hypoxia; NH, normobaric hypoxia; BP, barometric pressure; FO2, ambient fraction in oxygen; PO2, ambient pressure in oxygen.
FIO2 was measured using an oximeter (GOX 100T, Greisinger Electronic) with an external sensor (GCO/GOO 370, Greisinger Electronic). The precision of this oximeter was±0.1% O2±1 Digit (temperature for sensor ranged 0°–45°C and for oximeter−20°–50°C). PB and FIO2 were measured and recorded every 4 hours.
We took into account travel time to go to each place of experimentation. To reach the base to 1700 m, travel time was 20 min by car. And to reach base at 3000 m, the travel time was 25 min by lift. Each experimental period at each altitude and each travel time was carefully timed to match and reproduce these times in the hypoxic chamber for each subject.
Testing protocols
For all NN, HH, and NH conditions, a force plate (Win-Posturo®, Medicapteurs SA, Toulouse, France; Dekra certification) was used to calculate the CoP for lower limbs. Data were recorded by a PC computer with the Medicapteurs Winposture2000® software. The force plate measured 530 mm×460 mm×35 mm and was equipped with three pressure gauges (hysteresis<0.2%). Signal processing was accomplished with a 16-bit A/D converter at 40 Hz. Duration of each test was 25.6 seconds, allowing for 1024-point time series to be obtained.
The subjects were placed according to precise markers. Their legs were extended and their feet formed a 30° angle relative to each other (intermalleolar distance of 5 cm). The subjects were first requested to maintain balance with the eyes opened (EO) and then with the eyes closed (EC) and finally with a verbal Dual Task (DT). In the EO and DT conditions, the subjects looked at a fixed level target at a distance of 90 cm. They were instructed to stand with their arms at the sides and look straight ahead. The height of the visual target was adjusted for each subject. They were instructed to stand on the platform while trying to maintain postural stability during the trials in both NH and HH sessions. In the EC condition, they were asked to keep their gaze straight ahead and maintain postural stability. During the DT conditions, subjects were asked to count 3 of 3 starting from 100 to 0 and maintain postural stability. The final score and number of errors were retained for each subject.
A test-retest was performed in NN for assessing the reliability of the postural measures.
Data analysis
The CoP displacement was measured in medio-lateral plane (X-axis) and in antero-posterior plane (Y-axis). The total length of the CoP displacement (CoPxy), the variation of displacement in Y (CoPy), and in X (CoPx) were used in our analysis. The CoP surface area (CoPsurf) (90% confidence ellipse) evaluated the subject's postural performance: the smaller the area, the better the performance (Caron et al., 2000). Mean CoP speed (CoPs), which corresponds to the cumulative distance over the sampling period, was used to evaluate the ability of participants to control their balance. CoPs constitutes a good index of the activity required to maintain stability and has been considered as a sensitive and discriminant variable of postural stability (Baratto et al., 2002; Geurts et al., 1993; Maki et al., 1994; Raymakers et al. 2005). The variance of speed of CoP (CoPvs) that reflects the net neuromuscular activity required to maintain balance and characterizes the postural control of the subjects as well as the Romberg Index (RI) that is the ratio between measured parameters with EC and EO were calculated (Caron et al., 2000). Usually, body sway increases in EC, causing a detectable deterioration of performance. Accordingly, RI is expressed with a numeric value>1. Finally, for the DT condition, the final score reached during the counting and the number of errors were retained and averaged.
Statistical analysis
Mean (±SD) values were calculated for all variables of interest. After testing the assumption of normality of distribution (Kolmogorov–Smirnov test), the mean changes in postural parameters from NN to HH and from NN to NH were tested using the Wilcoxon test. A large number of comparisons led to an inflated Type I error. Therefore, Bonferroni adjustment is appropriate and was applied. Briefly, it is a procedure that consists of an adjustment in the alpha level based on the number of comparisons and the desired experiment-wise error rate.
An Intraclass Coefficient Correlation (ICC) in all parameters measured during the two consecutive trials in NN condition was calculated. Statistical analysis was computed using commercially available software (Sigmaplot version 9.0; Systat Software, CA). Statistical significance was accepted at p<0.05.
Results
The values of the postural control parameters in NN, HH and NH are presented in Fig. 1. The ICC (0.88–0.98) in NN condition showed a good reliability of the measurements. Ambient pressure in O2 was matched between HH and NH at 1700 and 3000 m, respectively (Table 1).
p<0.05 for differences with NN.
p<0.05 for differences with NH at same altitude.
p<0.05 for differences with Eyes Open.
p<0.05 for differences with Eyes Closed.
Δ NN-1700 P-value for the differences between change from NN to NH1700 and change from NN to HH1700.
Δ NN-3000 P-value for the differences between change from NN to NH3000 and change from NN to HH3000.
In the DT condition, the average score achieved was 29±17 in NN, 25±19, and 30±18 in HH1700 and HH3000 and 21±17 and 20±19 in NH1700 and NH3000 respectively. The average number of errors was 0.4±0.6 in NN, 0.3±0.5 and 0.4±0.7 in HH1700 and HH3000, and 0.3±0.4 and 0.2±0.2 in NH1700 and NH3000, respectively. No significant differences were found between the conditions.
Discussion
The main finding of this study was that the postural instability increased in hypobaric hypoxia (HH) but not in normobaric hypoxia (NH), when compared to normobaric normoxia (NN).
In the present study, after a short exposure either in NH or HH conditions, static posturographic assessment was realized in three conditions (EO, EC, and DT). We recorded the variations of CoP motion in medio-lateral (CoPx) and antero-posterior (CoPy) plane. To our knowledge, this is the first study comparing postural instability in HH and in NH at the same altitudes. In the present study, the measurements were performed after a short 30-min exposure. This might seem too short for inducing any different postural adaptations or physiological responses between HH and NH. However, the postural stability was reported to be disturbed almost immediately during exposure to HH (4300 m) and for at least 24h (Cymerman et al., 2001). However, although the acute adaptations observed in the present study were significant, we cannot speculate if a longer exposure would induce greater differences in postural control between HH and NH.
It is known that postural stability was significantly deteriorated at high altitude in healthy subjects (Baumgartner et al., 2002). However in NH condition, there are only few studies suggesting a deterioration on postural stability: recently, short-term exposure to NH was shown to induce postural instability specifically in antero-posterior plan (CoPy) only from 2538 m (FIO2: 15.7%) (Wagner et al., 2011). Previously CoPy was significantly increased when SpO2 decreased to 70% within 10 min by breathing hypoxic gas (FIO2: 6%–10%) (Holness et al., 1982) or body sway was increased after 4-min exposure to simulated altitudes of 5500, 4300, and 2440 m (Nordahl et al., 1998). Our results were not in agreement with these latest NH studies because we did not found any significant change about CoPy at 1700 m and 3000 m compared to NN values.
Contradictory to previous studies reporting significant lower stability control in NH than in NN (Cymerman et al., 2001; Hoshikawa et al., 2010; Nordahl et al., 1998; Wagner et al., 2011), we did not note any difference in CoPsurf, CoPxy, CoPx, CoPz, CoPs, and CoPvs between these two conditions. These later results suggest that a decrease in FIO2 would not affect the postural control to a small extent.
Comparison between HH and NH
CoPsurf was higher at HH3000 than in NH for the EO task. Moreover, the change from NN to HH3000 was higher than the change from NN to NH3000 for both EO and DT.
Potential mechanisms to explain the effects of HH on CoPsurf.
These results of CoPsurf higher in the HH conditions showed that neuromuscular control is altered by the hypobaric condition inducing significant oscillation of whole human body. These alterations of postural stability appeared to be correlated with acute mountain sickness (Baumgartner et al., 2002; Cymerman et al., 2001).
In general, dual-task interference produced increased excursion of the CoPsurf, and this effect became more pronounced with increase in task complexity. Even if we did not find any difference of change of CoPsurf between HH3000 and HH1700, this result could still explain that hypobaric task induced a decrease of cognitive performance like the findings of Tsarouchas et al. (2008) and contradictory to NH condition (Linde et al. 1997).
Vision seems to influence postural stability by reacting to motion as a relative image shift on the retina (Brandt et al., 1986) and it also triggers the muscle activation required for postural corrections. The efficiency of vision in postural control depends on visual acuity (Paulus et al., 1984) and visual contrast (Leibowitz et al., 1979). Since it was reported that HH influenced the visual system by inducing a significant decrease in visual contrast sensitivity (Benedek et al., 2002), we expected that RI would be more affected by HH than NH. Previous results were inconsistent. Cymerman et al. did not found any change of RI in NH condition as Baumgartner et al in HH whereas Nordahl et al. reported a decrease of RI with altitude for CoPs and CoPy (Baumgartner et al., 2002; Cymerman et al., 2001; Nordahl et al., 1998). In the present study, RI was neither modified by HH nor by NH because the ratio EC/OE evolved in the same proportions in NN, NH, and HH.
Potential mechanisms to explain the effects of HH on CoPy
In the present study, and in line with the results of Nordhal et al., (1998), postural instability was significantly higher in the antero-posterior plane (CoPy) but not in the medio-lateral plane (CoPx) at HH1700 compared to NH1700. This might be explained by the anatomical fact that hip and ankle joints are freer for movements in the antero-posterior than in the lateral plane and that the visual corrective input is greater in the lateral plane. It is known that α-motoneuron activity contributes to the ankle joint stabilization (Lephart et al., 1998). Moreover, reticulospinal pathways exist at all brain stem levels, and the outflow from this system was shown to influence spinal α-motoneuron excitability (Niemer and Magoun, 1947; Shapovalov, 1972). The HH condition could alter the activity of the reticular system. It was reported that low arterial oxygen pressure elicited cortical activation via afferent chemoreceptor activation of the ascending reticular activating system (Hugelin et al., 1959).
Postural instability could be evaluated by the variance of speed of CoP (CoPvs). This parameter corresponds to the acceleration of CoP and is correlated to postural muscles activity (Caron et al., 2000).
Potential mechanisms to explain the effects of HH on CoPvs
In our study, the CoPvs was lower in HH1700 than in NH1700. HH leads to a decrease in reflex activity of postural muscles and therefore a decrease in postural control. Although the vestibular-cerebellar system is part of the balance system and plays a central role in the maintenance of postural control, it may be speculated that this system could not be the only site disturbed. It is known that hypoxia affects not only somatosensory information but also its integration and hypoxia inhibits the tonic vibration reflex in humans (Delliaux and Jammes, 2006). Moreover, activation of muscular mechanoreceptors (group I afferents) by tendon vibration is largely attenuated in acute and chronic hypoxemia in different animal species (Dousset et al., 2001; Lagier-Tessonnier et al., 1993).
Although a systematic review on the test–retest reliability of center of pressure measures in bipedal static task conditions recommends data collection for at least 90 sec (Ruhe et al., 2010), we chose 25.6 sec as the duration of measurement in each condition and for each task for the following reasons:
• Previous studies about the effect of hypoxia on postural control used either 25.6 sec (Baumgartner et al., 2002; Cymerman et al., 2001; Hoshikawa et al., 2010; Wagner et al., 2011) or 51.2 sec (Nordahl et al., 1998). With this posturographic platform and an acquisition frequency of 40 Hz, 25.6 sec was long enough for our purpose.
• A previous study (Pinsault and Vuillerme, 2009) reported a good reliability (ICC>0.75) for this duration of 25.6 sec in young healthy adults. Moreover, our data presented a good reliability (ICC between 0.88 and 0.98).
Finally, we cannot neglect that the fatigue (for a measurement duration superior of 30 sec) would be greater in HH and that this would affect the postural stability. Since the aim of the present study was to compare the acute responses, we chose the shortest relevant duration in accordance with the literature.
However, some limitations are presents and further investigations are required to confirm the present results over a longer hypoxic exposure and for describing the time course of the postural adaptations. It would be interesting to explore the dose-effect response with a larger range of altitude levels as 3571 m (Jungfraujoch, Switzerland) and 4559 m (Capanna Regina Margherita, Italy) and with a larger sample size. In addition, it could be interesting to record EMG activity of the main postural muscles for better analyzing the impact of HH and NH on neuromuscular activity and CoPvs. Since differences in respiratory pattern have been reported between HH and NH (Loeppky et al., 1997; Savourey et al., 2003), recording the ventilatory pattern would be also of interest. The respiratory frequency has been associated with micro-movements of CoP (Sakellari and Bronstein, 1997) but the influence of the hypoxic ventilatory responses on postural control is unknown. Finally, to differentiate better the hypobaric effect, a fourth condition—normoxic hypobaria—is relevant. Studies of normoxic hypobaria are rare and are required as a control condition to determine whether the two independent variables (reduced PB and reduced PIO2) work in opposite directions to cause the observed responses.
Conclusions
Short exposure to hypobaric hypoxia at 1700 and 3000 m deteriorated the postural control whereas normobaric hypoxia did not. The relative increase in sway movements was higher in the antero-posterior plane than in the lateral plane. CoPvs was lower in HH than in NH. Overall, these results suggest that postural instability is more influenced by change in barometric pressure than by change in fraction of oxygen per se. Training in “real” or “simulated” altitude seems to induce different postural adaptation. These observations have practical implications in all sports where postural control is important.
Footnotes
Acknowledgments
The authors acknowledge Manu Praz for his technical assistance.
Author Disclosure Statement
No competing financial interests exist.