
Abstract
Abstract
Amon, Mojca, Michail E. Keramidas, Stylianos N. Kounalakis, Igor B. Mekjavic. The effect of a sleep high–train low regimen on the finger cold-induced vasodilation response. High Alt. Med. Biol. 13:32–39.—The present study evaluated the effect of a sleep high–train low regimen on the finger cold-induced vasodilation (CIVD) response. Seventeen healthy males were assigned to either a control (CON; n=9) or experimental (EXP; n=8) group. Each group participated in a 28-day aerobic training program of daily 1-h exercise (50% of peak power output). During the training period, the EXP group slept at a simulated altitude of 2800 meters (week 1) to 3400 m (week 4) above sea level. Normoxic (CIVDNOR; CON and EXP groups) and hypoxic (CIVDHYPO; FIO2=0.12; EXP group only) CIVD characteristics were assessed before and after the training period during a 30-min immersion of the hand in 8°C water. After the intervention, the EXP group had increased average finger skin temperature (CIVDNOR: +0.5°C; CIVDHYPO: +0.5°C), number of waves (CIVDNOR: +0.5; CIVDHYPO: +0.6), and CIVD amplitude (CIVDNOR: +1.5°C; CIVDHYPO: +3°C) in both CIVD tests (p<0.05). In contrast, the CON group had an increase in only the CIVD amplitude (+0.5°C; p<0.05). Thus, the enhancement of aerobic performance combined with altitude acclimatization achieved with the sleep high-train low regimen contributed to an improved finger CIVD response during cold-water hand immersion in both normoxic and hypoxic conditions.
Introduction
The level of physical fitness (Keramidas et al., 2010; Moriya and Nakagawa, 1990) and of altitude acclimatization (Daanen and van Ruiten, 2000; Felicijan et al., 2008) have been suggested as two nonthermal factors that could potentially affect the CIVD response. With regards to the former, Keramidas et al. (2010) observed a significant improvement in finger CIVD response as a consequence of a daily 1-hour aerobic exercise training in a 4-week period, which was more pronounced 10 days after the cessation of the training intervention. These responses were attributed to the training-induced central and/or peripheral cardiovascular adaptations such as increased cardiac output (Ekblom et al., 1968), diminished sympathetic activity (Grassi et al., 1994), and increased microcirculation (Maiorana et al., 2003).
The acute hypoxia-induced suppression of the CIVD response (Takeoka et al., 1993), appears to be partly reversed by prolonged exposure to a hypoxic environment (Daanen and van Ruiten, 2000; Mathew et al., 1977). In particular, Felicijan et al. (2008) observed an enhanced CIVD response in nine alpinists after a 3-week altitude expedition. The authors commented that during the expedition, other factors associated with the high altitude exposure might have also contributed to the observed increase in CIVD, specifically altitude acclimatization, cold acclimatization, and exercise. However, the manner in which these factors interact to influence the CIVD response remains unknown.
Thus, CIVD seems to benefit from aerobic training and altitude acclimatization. Possibly the combination of these two parameters may give the greatest improvement in CIVD. We therefore combined aerobic training with hypoxic exposure. The hypoxic exposure in our experiments was limited to the nights. According to this protocol, called “sleep high–train low” (SH-TL), subjects sleep in a hypoxic environment (SH, sleep high) and train near sea level (TL, train low). Of the hypoxic training protocols available, and used by athletes and climbers to enhance the O2 carrying capacity, and thus aerobic performance, SH-TL would appear to be most optimal (de Paula and Niebauer, 2010; Levine and Stray-Gundersen, 1997; Povea et al., 2005; Richalet and Gore, 2008;). Although the proposed mechanisms underlying such improvement in aerobic performance remain unresolved, most likely they include central (Levine and Stray-Gundersen, 2005) and peripheral (Gore and Hopkins, 2005) adaptations. Besides, it has been shown that altitude acclimatization can affect the expression of heat shock proteins (Magalhaes et al., 2005), which is considered a protective mechanism, specifically protecting proteins against cellular stress, such as the cold stress (cf. Sonna et al., 2002).
The purpose of the present study was to investigate the effect of SH-TL regimen on the finger CIVD response. We hypothesized that the known improvements in the CIVD response associated with sea level training (TL component) will be enhanced by including hypoxic acclimatization (SH component).
Materials and Methods
Subjects
Seventeen healthy male nonsmokers participated in the present study. All of them were near sea-level residents, and were not exposed to altitude >500 m during the month preceding the experiments. Moreover, they had no, or very limited previous experience with cold exposure experiments, and no history of circulatory disease or previous cold injuries. The subjects were informed in detail regarding the experimental procedures and gave their written consent. All were physically active on a recreational basis, and none were engaged in formal sport-training programs. They were instructed not to engage in any physical activity and to refrain from consuming alcohol or any caffeinated product 24 h prior to testing days. The tests were conducted at the same time of the day for each subject to ensure that the effect of diurnal variations was similar in all trials. The experimental protocol was approved by the National Committee for Medical Ethics at the Ministry of Health of the Republic of Slovenia and conformed to the Declaration of Helsinki guidelines.
Experimental protocol
On the first visit to the laboratory, subjects were thoroughly familiarized with all the testing and training procedures. The experimental protocol comprised three separate phases: (a) pre-training tests, (b) a 4-week training period, and (c) post-training tests. After completing all baseline tests, subjects were balanced according to age and aerobic capacity, and assigned to either the control (CON=9; age: 21.9±4.0 yrs; body mass: 72.0±6.0 kg; body fat: 9.2±2.9%; stature: 178.0±4.3 cm), or experimental (EXP=8; age: 23.9±3.0 yrs; body mass: 69.5±5.4 kg; body fat: 7.8±2.0%; stature: 178.6±5.2 cm) group (p>0.05). During both pre-training and post-training tests, all subjects performed an incremental exercise test to exhaustion. Two days later, they conducted a CIVD test, during which they immersed their right hand in cold water, while breathing room air (CIVDNOR). Apart from the CIVDNOR, the EXP group performed an additional CIVD test on a third test day, during which subjects breathed a hypoxic gas mixture (CIVDHYPO). The two CIVD tests were conducted in a counter-balanced order.
Testing sessions
Incremental exercise test to exhaustion
All subjects performed an incremental exercise test to exhaustion on an electrically braked cycle-ergometer (ERG 900S, Schiller, Baar, Switzerland) to determine their peak oxygen uptake (
Hand immersion
Each subject arrived at the laboratory at least 20 min before the test, to adapt to the controlled environment of the laboratory (temperature 22±1°C, relative humidity 35%–45%). During the hand immersion tests, subjects were lightly dressed in a T-shirt and short trousers, and remained resting on a semi-reclining chair for the entire experiment. The right hand was covered with a thin plastic bag (thickness of 0.025 mm) that was sealed with air permeable tape to the skin, approximately 10 cm above the wrist for the hand. Care was taken to remove all the air from the bag and to free the thermocouple sites from any plastic bag folds. Thereafter, subjects relaxed for 3 min with their hands at the level of the hips and resting values were recorded. After the 3-min resting period, the tested hand was immersed up to the ulnar and radial styloids in a tank filled with warm water (35°C) for 5 min. Afterward, subjects immersed the same hand in a different insulated tank with cold water (8°C) for 30 min. The temperature of the water was maintained with an active cooling system (Haake, Germany); and a propeller continuously stirred the water inside the tank. During the test, the immersed hand rested on an air-pillow that was positioned between the edge of the immersion bath and the forearm.
Throughout CIVDNOR, subjects breathed room air (FI
Finger pad skin temperature measurements were used to determine the vascular changes of the immersed fingers during the immersion tests. The finger pads are considered as a reliable temperature measuring site for evaluation of these changes (Daanen, 2003). Copper-constantan (T-type) thermocouple (each conductor was 0.2 mm in diameter) probes (Physitemp Instruments Inc., Clifton, NJ) were used in all experiments. The primary insulation material of the thermocouples was polytetrafluoroethylene (PTFE; insulation rating −75°C to +250°C). The uninsulated welded junctions of the thermocouples were attached to the skin. The probes were positioned in the middle of the palmar side of the distal phalanx of all five fingers of the right hand. The probes were attached directly to the skin by thin air-permeable tape (Tegaderm, 3M, Healthcare, St. Paul, MN).
Infrared tympanic temperature (Ttympanic), HR, and arterial pressure (AP) were recorded in pre-immersion and warm-water periods, and every 5 min during the cold-water immersion. In particular, Ttympanic was measured using a commercially available infrared thermometer (ThermoScan IRT 3020, Braun, Kronberg, Germany), HR was recorded using a heart rate monitor (Vantage NVTM, Polar Electro Oy, Kempele, Finland), and systolic (SAP) and diastolic (DAP) arterial pressure were measured with a noninvasive auscultatory method (300B, Speidel & Keller, Germany) on the nonimmersed arm. At the same time periods, subjects were requested to provide ratings of their temperature perception on a 10-point scale (TSS; from 0-unbearably cold to 9-very hot) and thermal comfort on a 5-point scale (TCS; from 1-comfortable to 5-extremely uncomfortable). In addition, during the immersion tests of the EXP group, capillary oxyhemoglobin saturation (SpO2) was recorded with a finger pulse oximeter (BCI 3110, Wisconsin).
Training protocols
Exercise training
Both groups trained 5 days per week for 4 weeks, and were supervised by the same investigators during the entire training period. All subjects exercised 1 hour on a cycle-ergometer at 50% of their pre-training PPO. The intensity of the exercise training was maintained so that the exercise HR corresponded to the HR measured at the 50% of PPO during the pre-training
Sleep high–train low (SH-TL)
During the 28-days study period, aside from the daily exercise training, the EXP group spent 9–12 hours per night exposed to a simulated hypoxic environment with an equivalent altitude ranging from 2800 to 3200 m above sea level (1st week: 2800 m; 2nd week: 3000 m; 3rd and 4th week: 3200 m). The FI
Statistical analysis
A computer program written in Matlab (MathWorks Inc, Natick, MA) was developed to determine the CIVD parameters from the raw data (Mekjavic et al., 2008). The results of the computer analysis were always checked manually to avoid any potential misinterpretation. The determined CIVD parameters during the hand immersion tests were the following:
1. Number of waves (N): the minimum temperature increase that was characterized as a CIVD response was set at 0.5°C. The minimum duration of such an increase in temperature was set at 3 min. 2. Average finger temperature (Tavg): the average temperature during the cold-water immersion period. 3. Temperature amplitude (ΔT): the difference between the lowest temperature recorded just before the CIVD and the highest temperature reached during the CIVD.
Statistical analyses were performed using Statistica 5.0 (StatSoft, Inc., Tulsa, OK). All the data are reported as mean±SD. Due to a technical problem with the temperature sensor positioned on the small digit (digit 5), only the data for the four digits will be reported. A three-way analysis of variance (ANOVA) for repeated measures was used to define the differences in CIVD parameters between the CON and EXP group during the CIVDNOR (group x testing phase x digits). Moreover, a three-way ANOVA for repeated measures was used to define the differences in CIVD parameters between the CIVDNOR and CIVDHYPO in EXP group (condition x testing phase x digits). Statistical significance of peak values during the incremental exercise tests (
Results
Training characteristics
There were no differences between the groups regarding the training HR (CON: 144±10 beats·min−1; EXP 148±6 beats·min−1; p>0.05) and L-RPE (CON: 10±2; EXP: 11±1; p>0.05). Moreover, the EXP group completed the 28-day training period without any symptoms of altitude sickness, as reflected by the scores of the Lake Louise Mountains Sickness questionnaires (mean Lake Louise score of 2.2±1.5; values 3 to 5 indicates mild mountain sickness).
Anthropometry
Body mass (CON: Pre=72.0±6.0, Post=72.5±5.6 kg; EXP: Pre=69.5±5.4, Post=70.1±5.2 kg; p>0.05) and body fat (CON: Pre=9.2±2.9, Post=9.2±3.8 %; EXP: Pre=7.8±2.0, Post=7.5±2.0 %; p>0.05) did not change in either of the groups over the course of the training period.
Aerobic capacity
Peak values during the maximal incremental exercise test are summarized in Table 1. Training significantly increased
Values are mean±SD. HRpeak: peak heart rate; L-RPEpeak: peak local sensation of effort; PPO: peak power output;
Statistically significant different from the pre-training period, (p≤0.05); #Statistically significant differences between the CON and EXP group (p≤0.05).
Hand immersion
CIVD characteristics
The EXP group had lower values of Tavg compared to the CON group during the pre-training CIVDNOR tests (p<0.001; Figs. 1A and 1B). However, only the EXP group increased the Tavg post-training compared to its pre-training values during both the CIVD tests (p<0.05).
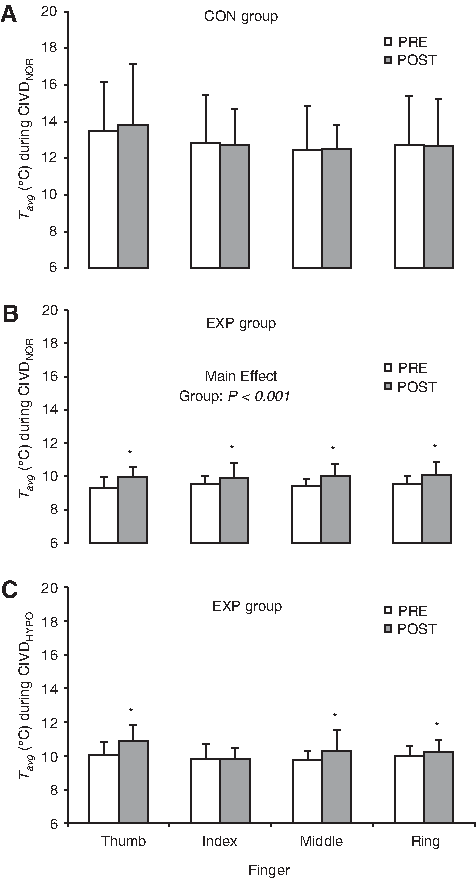
Average temperature (Tavg) in the four fingers of the right hand during
There were no differences in N between the groups during the pre-training and post-training periods (Table 2). However, the EXP group had higher values of N during the CIVDNOR after SH-TL compared to baseline values (p≤0.05; Table 2); these were more pronounced in the index and ring finger. Furthermore, the EXP group exhibited higher values of N during the post-training CIVDHYPO than in the pre-training tests (p≤0.05; Table 2).
Values are means±SD; *Statistically significant different from pre-training period, (p≤0.05).
There were no differences in ΔT between the groups during the pre-training and post-training periods (Fig. 2). There was a significant increase in ΔT during the post-training CIVDNOR in both groups (p<0.05; Figs. 2A and 2B). Likewise, there was a significant increase in the ΔT during the post-training CIVDHYPO (p<0.05; Fig. 2C).
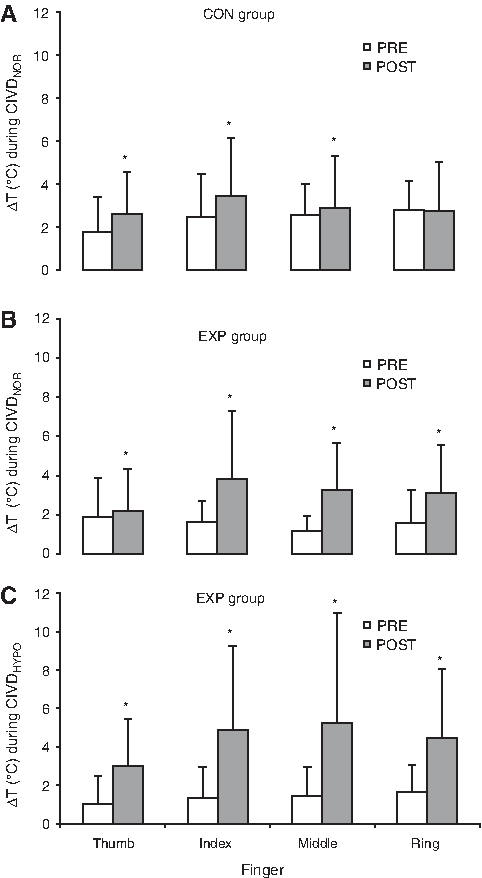
Temperature amplitude (ΔT) in the four fingers of the right hand during
HR and AP
The mean HR, SAP, and DAP obtained during the pre-immersion and cold-water immersion periods are summarized in Table 3. There were no differences in any of these cardiovascular variables between the groups during the pre-training and post-training tests. The EXP group had lower HR during the post-training CIVDHYPO compared to that observed in the pre-training tests.
Values are mean±SD; *Statistically significant different from the pre-training period, (p≤0.05).
Ttympanic, TSS and TCS
There were no significant differences in T tympanic , TSS and TCS in both groups during the pre-training and post-training tests (Table 3).
Spo 2
For the EXP group, the average Sp
Discussion
The principal finding of the present study is that hypoxic acclimatization enhances the training-induced augmentation of the CIVD response. The present results confirm our previous observation of an improvement in the CIVD response as a consequence of daily aerobic training (Keramidas et al., 2010), and demonstrate that the addition of hypoxic stimulus using the SH-TL regimen might potentiate these improvements. Specifically, the enhancement of aerobic performance combined with altitude acclimatization achieved with the SH-TL regimen contributed to increased average temperature, improved CIVD amplitude (particularly in hypoxia), and enhanced number of CIVD waves. Our findings are in agreement with previous studies exploring separately the contribution of fitness level (Keramidas et al., 2010; Masashi and Akihiro, 2004; Moriya and Nakagawa, 1990) and altitude exposure (Daanen and van Ruiten, 2000; Felicijan et al., 2008; Mathew et al., 1977) to the CIVD response.
CIVD at altitude (field studies)
Daanen and Van Ruiten (2000) studied the CIVD response of the cold-water immersed middle finger in 0°C at altitude in acclimatized (45 days at 5100–7000 m) and nonacclimatized (3 days at 5100 m) individuals. They observed that the initial suppression of the hunting reaction due to hypoxia was partly reversed in altitude-acclimatized subjects. Felicijan et al. (2008) observed improved CIVD characteristics (amplitude and average temperature) in members of a 3-week Himalyan expedition, although predominantly in the toes. Their results demonstrated a significant enhancement of the CIVD response as a consequence of high altitude acclimatization compared to a control group. However, in the aforementioned studies, the exact effect of hypoxia is not known, due to the coexisting stressors, such as cold and physical activity during an expedition.
Effect of SH-TL on CIVD
The observed enhanced performance after SH-TL is in agreement with previous studies (de Paula and Niebauer, 2010; Levine and Stray-Gundersen, 1997), which attributed the improvements to either central (oxygen transport enhancement) (Levine and Stray-Gundersen, 2005; Robach et al., 2006) and/or peripheral (muscle blood flow, buffering capacity) (Gore and Hopkins, 2005; Hahn et al., 2001) adaptations. Similarly, central (sympathetic vasoconstriction withdrawal (Flouris and Cheung, 2009) and/or peripheral (arteriovenous anastomoses, Daanen, 2003) factors have also been suggested to modify the CIVD response. Thus, the beneficial adaptations of both endurance training and acclimatization centrally and peripherally most likely contribute to the CIVD enhancement observed. Namely, the exacerbated CIVD response after SH-TL could be related to the improved blood supply in the fingers, given the fact that exercise training may enhance peripheral blood flow via microvascular angiogenesis in terminal arterioles and capillaries (Brown, 2003; Lenasi and Strucl, 2004). Furthermore, the enhancement of blood O2 carrying capacity for the CIVD improvement response is also likely (Rusko et al., 2004; Sawka et al., 2000). In addition, the enhancement of parasympathetic drive as a result of training (Grassi et al., 1994) and/or the reduced sympathetic response to hypoxia as a result of altitude acclimatization (Boushel et al., 2001; Povea et al., 2005) could also change the pattern of the cutaneous microcirculation in the extremities, resulting in a modification of the CIVD response. Moreover, an alternative mechanism might be the effect of altitude acclimatization on cellular homeostasis, such as the expression of heat shock proteins (Magalhaes et al., 2005), which in turn could attenuate the stress imposed by the cold stimulus during the immersion (cf. Sonna et al., 2002). However, the mechanisms underlying the enhanced CIVD response after the SH-TL regimen are still conjectural and need to be further investigated.
Methodological considerations
It has been previously shown that an individual's thermal status affects the CIVD response (Daanen and Ducharme, 1999; Dobnikar et al., 2009; Flouris et al., 2008). In the current study, the thermal status of the subjects was indicated by Ttympanic, which is a valid index of core temperature (Flouris and Cheung, 2010; Mekjavic et al., 1992), and the Tavg prior to the hand immersion in the warm water. Despite the fact that we did not detect any difference in Ttympanic, the Tavg prior to the immersion was different between the groups. The latter might be explained by seasonal variation. Namely, the experiments were performed at different times of the year (CON group: April to May, EXP group: September to October), and it has been reported that finger Tavg is higher during the spring than the autumn months (Tanaka, 1971; Tanaka et al., 1984). In order to minimize the variability in the starting skin temperature, both groups arrived at least 20 min before the commencement of the test to become acclimated to the controlled thermoneutral environmental conditions of the laboratory, and they immersed their hand in warm water of 35°C for 5 min to increase the local blood flow and to raise tissue temperature before the immersion in cold water. However, despite the similar values of Tavg at the beginning of the CIVD tests, the EXP group had unexpectedly lower values of Tavg during the pre-training CIVD tests. Irrespective of the cause of this discrepancy between the groups, both groups performed the Pre and Post tests under the same conditions. A further explanation for the observed discrepancy may be that during the 28-day SH-TL regimen, subjects in the EXP group were housed in the Olympic Sport Centre Planica (Slovenia) and were not exposed to any cold stress. Thus, the observed responses are a consequence of solely altitude acclimatization and training. During their sojourn in the Olympic Sports Centre, their nutrition, hydration, and physical activity was monitored. Prior to the CIVD test, they came to the laboratory from their respective rooms. In contrast, the CON group of subjects lived at home, and was not under constant supervision.
Moreover, it might be argued that any possible differences in the anthropometry of the subjects' hands could explain the different CIVD responses (Sienkiewicz et al., 1989). However, in a previous study conducted in our laboratory (Gorjanc, 2011), no correlation was observed between the hand volumes and the CIVD response, thereby indicating that hand anthropometry does not contribute significantly to the nature of the CIVD response. The homogenous group of subjects (age, sex, similar occupational characteristics and sports activities) and the repeated measures design used in the present study suggest that the characteristics of the hands did not vary between the groups and the testing periods.
Minimizing the risk of cold injury
The aim of achieving enhancement in the CIVD response is to induce a higher average skin temperature. In addition to the typical CIVD response, several atypical responses have been identified (Cheung and Mekjavic, 2007; Mekjavic et al., 2008; Reynolds et al., 2007). Common to all these responses is that greater and more frequent amplitudes of the CIVD response cause an increase in Tavg. Thus, although the CIVD response is characterized by many parameters, in terms of its cryoprotective mechanism it is the increased perfusion-induced elevation in Tavg during cold exposure that is ultimately the goal of any intervention attempting to minimize cold injury.
In conclusion, the present study shows that the SH-TL regimen improves the CIVD response during a cold-water hand immersion. Despite the fact that still remains obscure whether the SH-TL is more advantageous than a typical aerobic exercise training protocol, it is apparent that daily hypoxic stimuli inducing altitude acclimatization enhance CIVD response rather than suppress it. Moreover, the combination of aerobic training and altitude acclimatization appears to be a more efficient approach compared with repeated exposures to cold (Mekjavic et al., 2008) for the enhancement of the CIVD response. From a practical perspective, the present results suggest that after SH-TL the possible higher risk of cold injury due to prolonged high altitude exposure is not only prevented, but rather might be potentially reduced. However, the utility of SH-TL as a preventive method for cold injuries cannot be discerned from the present results. Indeed, despite claims that CIVD may have a cryoprotective function, there is as yet no evidence of a direct link between the quality of CIVD response and cold injury prevention. As others, we can only speculate that the observed enhancements could probably increase the prophylaxis against cold injuries during mountain expeditions.
Footnotes
Acknowledgments
The current study was funded, in part, by the Olympic Committee of Slovenia, and by a “Knowledge for Security and Peace” grant from the Ministry of Defense (Republic of Slovenia). We would like to thank all the subjects for their participation. We are also grateful to Bojan Musizza and Miro Vrhovec for their technical assistance.
Disclosure Statement
The authors state that there is no personal or financial conflict of interest in the present study.