
Abstract

At sea level, improving oxygen delivery to working muscles results in a higher VO2max (Audran et al, 1999; Birkeland et al, 2000; Ekblom and Berglund 1991; Robach et al, 2008; Russell et al, 2002). At altitude, the factors limiting exercise performance appear to be different from those at lower elevations, leading several authors to suggest that reducing hypoxic pulmonary vasoconstriction (HPV) improves exercise performance (Faoro et al, 2009; Ghofrani et al, 2004; Naeije et al, 2010). The argument follows the intuitive premise that lowering pulmonary artery pressure (PAP) by decreasing pulmonary vascular resistance (PVR) will reduce RV afterload, allowing higher maximal cardiac output. Since output from the left and right ventricles is coupled, it is postulated that elevated RV afterload will significantly limit left ventricular cardiac output.
The focus of this debate is two-fold: 1) do changes in right ventricular (RV) afterload have a significant influence on maximal cardiac output? and 2) are the observed improvements in exercise performance at altitude after pulmonary vasodilators due to an increased cardiac output? For the current debate, we will limit our discussion to normal, healthy individuals either acutely or chronically hypoxic. These subjects would have a normal HPV response to altitude. Subjects with exaggerated HPV, as seen in individuals susceptible to high altitude pulmonary edema (HAPE), will only be briefly mentioned.
We propose that reduction of PAP in healthy subjects at high altitude (above ∼4000 m) does not impact exercise performance or improve VO2max. Four lines of evidence for this argument are evaluated, namely: 1) altitude modeling studies indicate that substantial changes in cardiac output produce minimal effects on VO2max, 2) breathing supplemental oxygen at altitude restores working capacity to normal sea level values without normalizing PVR, 3) individuals with elevated PAP at altitude have similar VO2max values as compared to those with lower PVR, and 4) improved oxygen saturation and other mechanisms, not lower PAP, are primarily responsible for improved exercise performance following pulmonary vasodilator treatments. Each line of evidence is expanded upon below.
Models of Exercise Performance at Altitude
Over the last 30 years, investigators have modeled the oxygen transport system at elevations up to the summit of Mount Everest (8850 m) (Piiper and Scheid 1981; Wagner 1996; 2000a; 2010). These models largely arrive at similar conclusions, that at altitude: 1) no single factor limits VO2max, and 2) above ∼4500 m, increasing cardiac output provides little increase in VO2max (Fig. 1).
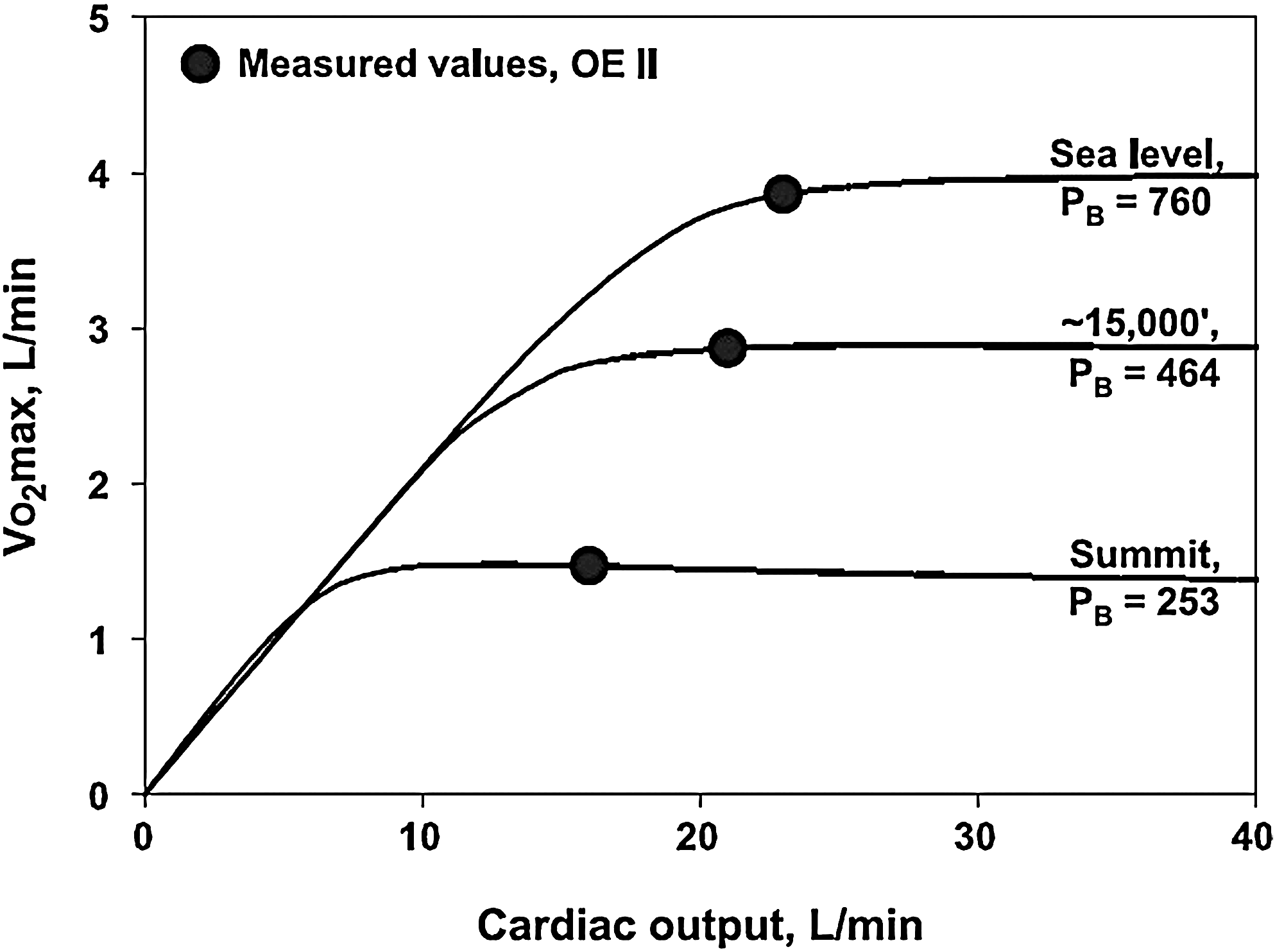
Predicted VO2max as a function of cardiac output at sea level, 15,000 ft (4572 m), and 8850 m. The model is based on that of Wagner (1996) using data from Operation Everest II (Sutton et al., 1988; Wagner et al., 1987). The filled circles represent actual data from OEII and the lines show how VO2max would change with changes in cardiac output (assuming no change in other parameters). Note that maximal cardiac output with exercise at each altitude above sea level is within the horizontal portion of each curve, demonstrating that changes in cardiac output have little effect on VO2max. Reprinted from Wagner (2010).
Although these models provide theoretical evidence, experimental human studies provide more substantial proof that oxygen delivery, regardless of mechanism, does not affect exercise performance at extreme altitudes. Altitude studies with β-adrenergic blockade (Bogaard et al, 2002; Moore et al, 1986) and vagal blockade (Boushel et al, 2001) demonstrate significant alterations in maximal heart rate without affecting VO2max or maximal cardiac output. In another study, Lundby et al. infused ATP into the femoral artery of subjects at 4559 m to cause peripheral microvascular vasodilation. The intervention lowered mean arterial pressure but failed to alter cardiac output or femoral artery oxygen consumption, leading to the conclusion that changes in mean systemic pressure did not limit cardiac output (Lundby et al, 2008).
Another experimental approach to enhance oxygen delivery to the tissues is through changing hemoglobin concentration while maintaining constant total blood volume. Robach et al. found that in acutely hypoxic exercise recombinant human erythropoietin increased VO2max up to an altitude of 3500 m, but the effect disappeared at 4500 m (Robach et al, 2008). Young et al. infused erythrocytes to increase hemoglobin but found no improvement in VO2max at 4300 m (Young et al, 1996). While keeping blood volume constant, Calbet et al. acutely reduced hemoglobin from 18.5 g/dl to 14.2 g/dl, and found no change in VO2max or maximal cardiac output at 5260 m (Calbet et al, 2002). These findings, along with those of earlier studies (Sarnquist et al, 1986; Schaffartzik et al, 1993; Tufts et al, 1985; Winslow et al, 1985), suggest that above about 4000–4500 m alterations in O2 delivery, even without changing cardiac output, produce little or no change in VO2max.
Effects of Supplemental Oxygen
Operation Everest II (OEII) provided a unique opportunity to measure PAP directly in a simulated environment equivalent to the summit of Mount Everest. These data provide a clear picture of preserved cardiac function under conditions of severe hypoxia, and demonstrate that PVR is unchanged by the acute administration of 100% oxygen (Groves et al, 1987; Reeves et al, 1987; Reeves et al, 1990). The mechanisms leading to unresponsiveness of PVR are likely related to vascular remodeling. The time frame for these changes is unknown, but certainly occurred within the 40 days exposure in OEII.
Although 100% O2 did not reduce PVR, it can return VO2max and cardiac output to sea level values. Pugh found that exercise capacity and cardiac output were restored close to sea level values with supplemental oxygen (Pugh 1964; Pugh et al, 1964). After 9 weeks acclimatization at 5260 m, breathing an FIO2 of 0.55 returned maximal cardiac output and power output to sea level control values (Boushel et al, 2001; Calbet et al, 2002). Lundby et al. demonstrated a return to sea level VO2max values after several days at 4559 m by “mild hyperoxia” (Lundby et al, 2008). Withdrawal of sympathetic tone, as suggested for dexamethasone, along with the increased PIO2 may contribute to these findings (Fischler et al, 2009; Siebenmann et al, 2011). These observations are not universal. Other researchers, using different experimental conditions, found less than complete return of VO2max or cardiac output to sea level values with supplemental oxygen (Lundby et al, 2004; Saltin et al, 1968; Wagner et al, 2002). Possible explanations of these disparate results include detraining of the subjects during the time at altitude and changes in systemic blood flow distribution (Lundby et al, 2004). Since cardiac output in healthy acclimatized subjects at altitude breathing supplemental oxygen can reach sea level maximal values despite unchanged (and elevated) PVR, it is clear that cardiac output is not determined by RV afterload under these conditions.
Pulmonary Hypertension Does Not Universally Decrease Exercise Capacity
Patients with chronic mountain sickness (CMS) provide a natural experiment since these individuals have increased hemoglobin concentrations and increased pulmonary pressures. Several studies report that healthy Andean highlanders have aerobic capacities comparable to acclimatized lowlanders (Kollias et al, 1968; Lundby et al, 2004; Penaloza and Arias-Stella 2007) but few maximal exercise data in CMS patients without overt heart failure exist (Leon-Velarde et al, 2010; Maignan et al, 2009; Penaloza and Arias-Stella 2007; Reeves and Leon-Velarde 2004; Stuber et al, 2010). A recent abstract from Naeije's group reports similar VO2max values in 10 CMS patients compared with 15 age and body mass index-matched healthy highlanders (Groepenhoff et al, 2011).
VO2max in HAPE-susceptible (HAPE-s) subjects is equivalent to that of control subjects during normoxic exercise and, more importantly, the decline in VO2max is similar in these groups despite the differences in their pulmonary vasculature responses to hypoxia (Eldridge et al, 1996; Steinacker et al, 1998). Two additional studies evaluated the effects of drug administration on exercise capacity in HAPE-s subjects. Fischler et al. studied 23 HAPE-s subjects randomly assigned to placebo, dexamethasone, or tadalafil in a double-blind trial at the Capanna Regina Margherita (4559 m) (Fischler et al, 2009). Exercise testing was conducted shortly after arrival to the Margherita hut with echocardiography performed the next day. The groups all had comparable responses at low altitude; however, the dexamethasone group, but not the tadalafil group, had significantly less reduction in VO2max at 4559 m compared with VO2max at low altitude. Their data do not exclude the possibility that impaired RV function contributed to these findings, but this was felt unlikely since reduced RV stroke volume would result in an increased heart rate and thus a reduced heart rate reserve. Their data showed equivalent heart rate reserves in all groups.
In a follow-up study, Siebenmann evaluated upright cycle ergometer exercise in 24 HAPE-s subjects (including 16 subjects from Fischler's study) (Siebenmann et al, 2011). Exercise testing was conducted after the first night at the Margherita hut. Exercise performance, VO2max, and O2-pulse (a noninvasive estimate of stroke volume) were higher in the dexamethasone group. O2 saturation during maximal exercise was similar in both the dexamethasone and control groups. However, the dexamethasone groups maintained this saturation at a significantly higher workload. The authors suggest that a combination of a higher maximal cardiac output (inferred but not directly measured) and improved oxygen diffusion in the lungs (that allowed a similar O2 saturation despite shorter pulmonary transit time) explain their findings (Siebenmann et al, 2011).
Pulmonary Vasodilator Studies
Numerous attempts have been made, with varying success, to improve VO2max and/or exercise performance at altitude using pulmonary vasodilators. Given the variety of experimental designs, the widely differing results are not surprising.
Ghofrani et al. (2004) conducted one of the earliest trials of sildenafil, studying subjects both in a low-altitude laboratory and in the field at Everest base camp (5245 m). They interpreted the observed improved exercise capacity as most likely due to reduced RV afterload, although the accompanying editorial by Rubin and Naeije pointed out that improved arterial O2 saturation may have contributed to the results (Rubin and Naeije, 2004). In a study conducted at the Observatoire Vallot (4350 m), Richalet et al. (2005) observed improved VO2max with the use of sildenafil and attributed this to both a decreased RV afterload and to improved oxygenation. With acute normobaric hypoxia, FIO2 of 0.1, Faoro et al. (2007) observed improvement in VO2max from ∼27 to ∼32 ml/kg/min along with increased O2 saturation from 62% to 68% when subjects took 50 mg sildenafil. At a simulated altitude of 3874 m, Hsu et al. demonstrated improved 5-km time trial performance and increased arterial oxygenation after subjects took sildenafil (Hsu et al, 2006). Importantly these improvements were all attributable to a subset of their subjects who were “responders” to sildenafil while the other subjects showed no response (Hsu et al, 2006). Vasodilator medications may play an important role at the level of heart or skeletal muscle through their effects on the nitric oxide (NO) pathway. NO operates as a signaling molecule that regulates mitochondrial respiration and may contribute at the cellular level to improved exercise capacity at altitude (Lansley et al, 2011; Shiva et al, 2007; Taylor and Moncada 2010).
Not all trials of phosphodiesterase-5 inhibitors have found improvements in VO2max or exercise performance at altitude. In a hypobaric chamber at a simulated altitude of 5000 m, Ricart et al. studied 14 healthy males. Although maximal exercise was not performed, submaximal arterial O2 saturation was not altered by 100 mg sildenafil, despite a significant blunting of systolic PAP response to hypoxia (Ricart et al, 2005). In another study, after 2-weeks acclimatization on Mount Chimborazo (5000 m), subjects did not increase VO2max or arterial O2 saturation while taking sildenafil (Faoro et al, 2007). At the Margherita hut (4559 m), tadalafil failed to improve exercise performance in contrast to the subjects who took dexamethasone (Fischler et al, 2009). Finally, in a recently published, randomized, placebo-controlled crossover trial, sildenafil did not improve 15-km time-trial performance at either 2100 m or at 3900 m (Kressler et al, 2011).
Two studies using endothelin-receptor antagonists (bosentan and sitaxentan) reported increased exercise capacity at high altitude, while a third study did not show any benefit from bosentan. Faoro et al. (2009) studied 11 volunteers in a double-blind cross-over study with subjects breathing either room air (FIO2 0.21) or FIO2 of 0.12 for ∼90 minutes while undergoing echocardiography and exercise testing. Subjects took either bosentan or placebo for 3 days prior to testing. With hypoxia, bosentan decreased systolic PAP, shifted the mean PAP–cardiac output relationship to lower pressures and VO2max from 35 to 39 ml/kg/min without any change in exercise arterial saturation. The changes in systolic PAP were loosely correlated with the change in VO2max (r2=0.53). These findings contrast with those of Seheult et al. who tested eight subjects in a double-blind cross-over study at the Barcroft Laboratory, White Mountain Research Station at 3800 m altitude (Seheult et al, 2009). The subjects took bosentan for 5 days before going to altitude and were studied 36 hours after ascent to altitude while still taking bosentan. Systolic PAP was unaffected by bosentan as was time-trial performance, possibly due to the dosing regimen used and the fluid retention properties of bosentan acting on kidney endothelin receptors (Ge et al, 2006).
A trial of the endothelin-receptor antagonist, sitaxentan, was conducted by Naeije et al. (2010) using a cross-over design breathing gas mixtures with either an FIO2 of 0.21 or 0.12. This was combined with a chronic hypoxic exposure to 5050 m altitude in subjects assigned either to a placebo arm or to sitaxentan. In the cross-over portion of the study, sitaxentan significantly decreased systolic PAP and increased hypoxic VO2max from 32 to 35 ml/km/min, while at 5050 m sitaxentan limited the hypoxia-induced decrease in VO2max by 10% compared with placebo. The correlation between the change in systolic PAP and change in VO2max was weak (r2=0.33) (Naeije et al, 2010).
Noninvasive pulse oximetry data, particularly during exercise, is notoriously inaccurate. In a study of acute hypoxia (FIO2 of 0.11 for ∼180 minutes), Olfert et al (2011) studied sildenafil in one group and bosentan in another group of subjects. They sampled blood from an indwelling radial artery catheter during exercise up to about 90% of VO2max. Both drugs significantly increased arterial oxygenation at rest and during exercise. While pulmonary artery pressures were not measured, their findings provide strong support for alternative mechanisms beyond the reduction of RV afterload for the beneficial effects of these medications.
Conclusions
Although the argument that RV afterload constrains cardiac output appears intuitive, theoretical and experimental data clearly demonstrate the shortcomings of this premise. Elegant modeling studies based on OE II data establish the theoretical basis that is further validated by numerous human trials demonstrating that increased cardiac output is not responsible for improved exercise capacity at high altitude. Pulmonary vasodilators have several effects beyond simply reducing RV afterload that may explain the positive studies. The poor correlation between the changes in systolic PAP and VO2max in the endothelin–receptor antagonist studies and the highly variable responses in the phosphodiesterase inhibitor trials argues against RV afterload having a significant effect. Since acute normalization of PIO2 can return VO2max and cardiac output to maximal sea level values despite unchanged PVR, the concept of constrained maximal cardiac output by RV afterload during maximal exercise in healthy individuals at altitude remains speculative and unproven.
Footnotes
Author Disclosure Statement
Drs. Anholm and Foster have no conflicts of interest or financial ties to disclose.