
Abstract
Abstract
Selig, Harald F., Michael Hüpfl, Helmut Trimmel, Wolfgang G. Voelckel, Peter Nagele. Pediatric trauma in the Austrian Alps: The epidemiology of sport-related injuries in helicopter emergency medical service. High Alt. Med. Biol. 13:112–117.—
Introduction
In a mountain environment, trauma related to sports/outdoor activities (predominately winter sports) is by far the most common cause for helicopter activation (Demartines et al., 1991; Kaufmann et al., 2006; Marsigny et al., 1999; Voelckel and Trimmel, 2008). On average, 4000 rescue missions for injuries caused by outdoor activities are flown in the Austrian Alps per year. An infrequent but substantial patient group involves the pediatric population (Selig et al., 2011).
The epidemiology of pediatric sports-related injuries is well described in the literature (Caine et al., 2008; Damore et al., 2003; Taylor and Attia 2000) and there is evidence that children are increasingly participating in mountain and wilderness recreation (Heggie, 2010). Particularly in winter sports, they are more likely to sustain sports-related trauma and suffer from more severe injuries than adults (Corra et al., 2004; Skokan et al., 2003). So far, we are not aware of any study focusing on pediatric sports-related trauma served by HEMS in an alpine environment. Thus, based on a nationwide sample of HEMS rescue missions, we aimed to investigate the main characteristics and injury patterns of pediatric sports-related trauma to evaluate the focal points HEMS crews face at a specific environmental area of operation.
Materials and Methods
Setting
Our study analyzed all children under 15 years of age injured during sports/outdoor activities in the Austrian Alps and attended by HEMS from January 1, 2006 to June 30, 2007. The Alps cover 65% of Austria's national territory with an area of 54.620 km2 and almost 40% (3.2 Mio) of Austria's population. Because the Alps serve as the ideal region for sports/outdoor activities, tourism in Austria is characterized by its specific geographical situation, especially during the winter season. During this period of time, approximately 350,000 tourists stay in Austria per day in addition to its residents (Statistics Austria, 2009); around 40% (140,000) of that number accounts for tourists in Tyrol, a mountainous federal state in Western Austria with a high density of skiing resorts. In Austria, approximately 200,000 sports-related injuries requiring hospitalization are registered every year; one out of five affects children younger than 15 years. In the alpine environment, around 10,000 pediatric sports-related injuries occur every year as indicated in Figure 1 (Injury Database Austria 2003-2009).
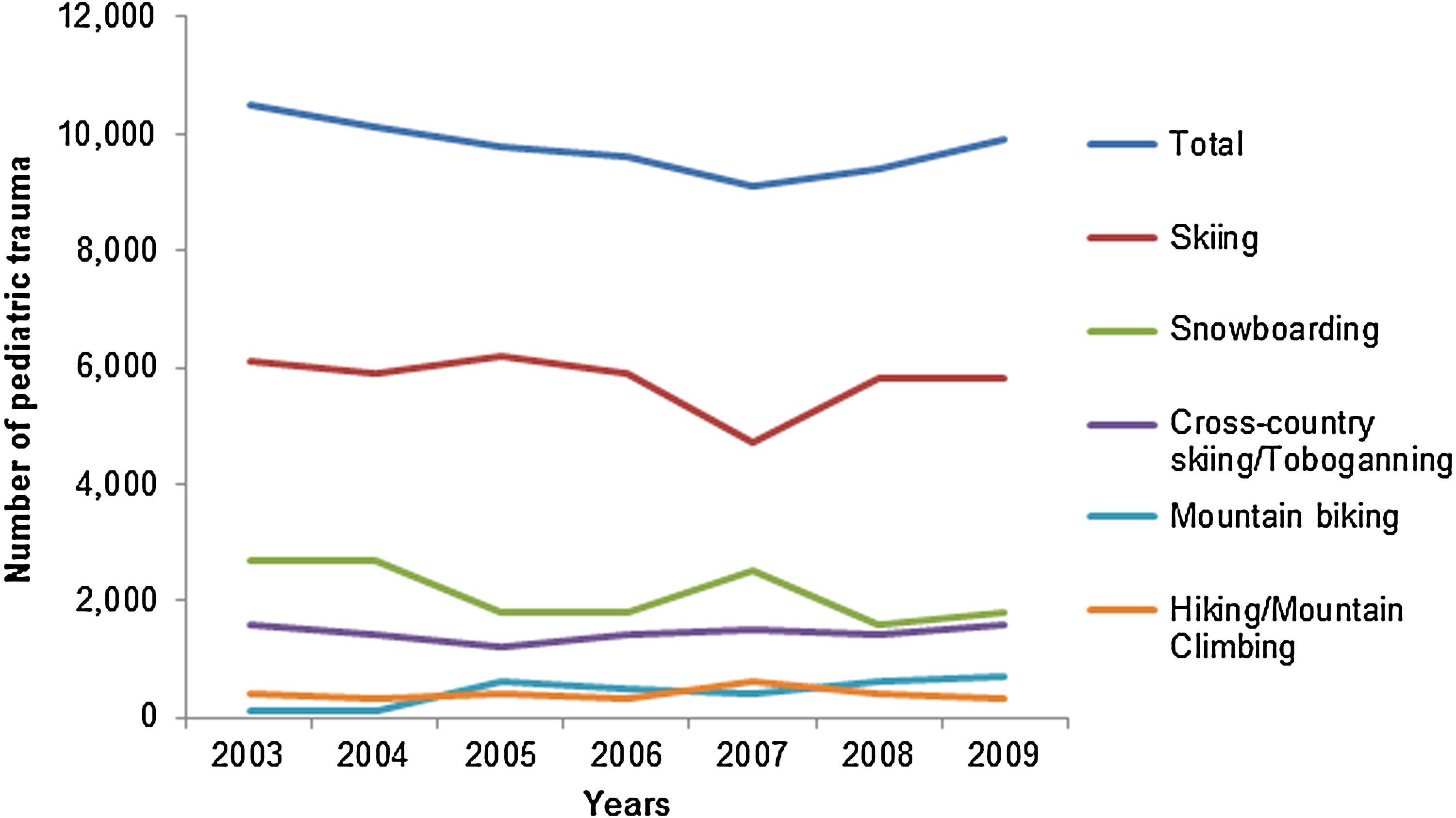
Pediatric sports-related trauma patients (<15 years of age) in alpine environment requiring hospitalization in Austria between 2003 and 2009 (Source: Injury Database Austria). The total number of hospitalized pediatric trauma patients injured during sports/outdoor activities in alpine environment approximates 10,000 injuries per year, without any substantial differences since 2003. Significant differences of injuries stratified by outdoor activity have not been reported since 2003. The predominant cause of injury has been skiing, followed by snowboarding and cross-country skiing/tobogganing.
Helicopter Emergency Medical Service
In Austria, a nationwide air-rescue service is run by the automobile-motorcycle-touring club (OEAMTC) as “Christophorus air-rescue service”. The OEAMTC is a private organization that provides nationwide air-rescue service in Austria in cooperation with the Austrian Federal Ministry of Internal Affairs. The OEMTC HEMS organization operates 16 helicopter bases, of which 12 guarantee HEMS supply in an alpine environment. In addition, 6 alpine helicopter bases are run in cooperation with the private air rescue service Heli Ambulance Team (HAT) only in winter. Other private air rescue services (up to 17 private helicopters) supplement the increased need in Austria's alpine regions during skiing season. The federal state of Tyrol alone comprises 11 HEMS helicopter bases in winter, which signify a unique HEMS density. In general, rescue helicopter operations during winter are conducted from dawn to dusk, which translates into less than 10 hours/day.
Air-rescue helicopters are staffed by an emergency physician, an emergency medical technician, and the pilot. Because of the unique operational conditions in mountain environment, HEMS crews have to be specially trained. In addition to profound experience in ground-based EMS and special knowledge of intensive and emergency care, emergency physicians have to attend special seasonal courses in mountain medicine.
Data collection and analysis
This study analyzed all HEMS flights for pediatric trauma caused by sports/outdoor activities in alpine environment. Alpine emergency scenes were defined by the abstractor as areas located more than 800 meters above sea level. OEAMTC has been using a proprietary computer-based documentation system (Leonardo, currently Version 2.2.2) since 2006 that includes all data from the HEMS flight report. The following variables that are obligatory to report were collected: age, sex, primary diagnosis, etiology of injury, prehospital therapy, prehospital monitoring, Glasgow Coma Scale (GCS) score, and National Advisory Committee for Aeronautics (NACA) score. The injury severity score (ISS), revised trauma score (RTS), abbreviated injury score (AIS), and trauma injury severity score (TRISS) were unavailable. The prehospital diagnoses were determined by abstracted data, not by ICD-codes.
Age groups were classified as toddlers (3–5 years of age), children in early school age (6–9 years), and in late school age (10–14 years of age). The abstractor stratified all cases by the etiology of injury: skiing, snowboarding, other activities. Based on the physician's suspected prehospital diagnoses, each case was stratified into “fracture”, “contusion”, “traumatic brain injury (TBI)”, and miscellaneous (including blunt abdominal trauma, major trauma, traumatic dislocation, snow burial, multiple trauma), and the main pattern of injury was allocated for each pediatric emergency.
Descriptive statistics were used for data analysis. Numbers are given as fractions for nominal and ordinal data. Data collection was based on Excel™ (Microsoft, Seattle, WA) and data analysis was performed by using SPSS™ 17.0.2 (SPSS Inc., Chicago, IL).
Results
During the 18-month study period, 912 HEMS rescue missions were flown for pediatric sports-related trauma in alpine environment; that number is equivalent to a prevalence of 3.4% out of a total of 26,850 helicopter rescue missions. No HEMS transport was carried out in 1.4% (n=13). One-hundred-forty-six children (16.0%) were severely injured (according to NACA IV-VI), whereas 89.1% (n=812) equaled NACA III or higher. No deaths on the scene (equivalent to NACA VII) were recorded.
Table 1 summarizes the characteristics of the study population differentiated by type of sports/outdoor activity. The majority of rescue missions were related to skiing (82.1%; n=749). Other causes of injuries were related to snowboarding (n=117), hiking (n=6), tobogganing (n=6), biking (n=5), horse-back riding (n=3), and miscellaneous activities (n=26). In total, 73 (8.0%) sports-related injuries were caused by collision with another skier or snowboarder. The prevalence of serious trauma and predominance of boys and children in late school age were similar in each sports/outdoor activity group. In regard to the male–female ratio, girls showed a higher prevalence of serious snowboard-related trauma than boys (21.4 and 12.0%, respectively).
NACA=National Advisory Committee for Aeronautics.
The most common diagnoses were fracture, contusion, and traumatic brain injury (see Table 1). The majority of fractures were related to the lower extremities (62.7%, 269/429), predominately caused by skiing (94.4%, 254/269), of which 224 (83.3%) were of minor injury severity. Thirty-one percent (48/155) of children suffering from TBI were in a serious condition (according to NACA > 3), whereas 3.4% (6/155) children exhibited a GCS lower than 9.
Overall, the main injury patterns in skiing were related to the lower extremity (40.5%), whereas injuries caused by snowboarding were mainly related to the upper extremity (29.1%). Head/facial trauma was equally distributed between skiers and snowboarders (21.2% and 22.2%, respectively). One-hundred thirty-four (14.7%) children suffered from spinal injury; of whom 82.8% (111/134) were between 10–14 years of age, and 10.4% (14/134) were rated to be severely injured.
The most common patterns of injury in each age group are summarized in Figure 2. Injuries related to the lower extremities and head decreased by age-group. The percentage of spinal and multiple trauma was higher in early and late school age compared to toddlers.
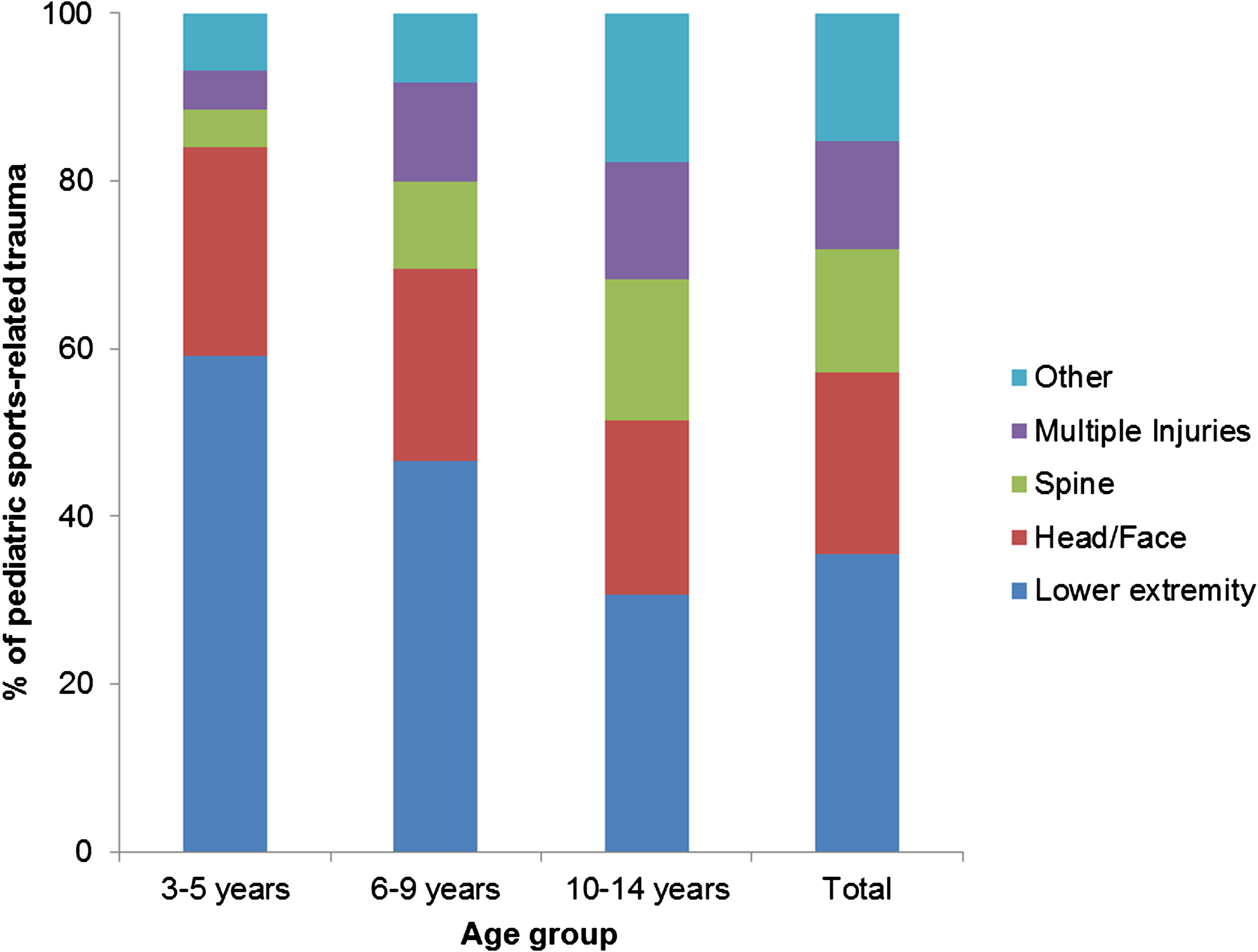
Injury patterns of pediatric sports-related trauma stratified by age group. The most frequent patterns of injury were related to the lower extremities, head/face and spine in each pediatric age group. A decline of trauma related to the lower extremity and the head/face by age group was identified, whereas spinal and multiple trauma increased with age.
Discussion
This retrospective study was conducted in order to evaluate epidemiological characteristics of pediatric trauma related to sports/outdoor activities in alpine environment. Prior research gave evidence that such knowledge incorporated into appropriate skills training translate into a better transport care with fewer avoidable adverse events in critically injured children (Macnab 1991; Sharples et al., 1990)
Overall, skiing was by far the most common reason for HEMS activation. Fortunately, only a minority of pediatric trauma patients were in a critical or life-threatening condition. The leading primary diagnosis was fracture, predominately of minor severity and related to the lower extremity. Head and spinal trauma were also of substantial occurrence.
Our analyzed data is based on an almost nationwide sample of HEMS rescue missions for children injured in the Austrian Alps. Therefore, this study can be assumed to be representative for air-rescue services operating in other Alpine countries. To the best of our knowledge, epidemiological data analyzing pediatric sports-related trauma served by HEMS in alpine environment have not yet been published.
Although previous reports could show that pediatric snowboard-related injuries have risen (Hayes and Groner, 2008; Sacco et al., 1998), skiing is still counted among one of the leading causes of sports-related injuries in children (Hagel, 2005). Our findings signify the predominant role of skiing injuries within a HEMS rescue system operating in an alpine environment, which is in accordance with previous reports (Kaufmann et al., 2006; Marsigny et al., 1999). Despite the fact that a considerable number of pediatric injuries related to mountain biking, hiking, or tobogganing require hospitalization in Austria (Fig. 1), these types of injury were rare in HEMS. In these cases, HEMS activation may not have been necessary because of the availability of ground-based EMS.
Our results support the finding of previous sports injury studies that males are more commonly injured and account for more serious injuries than females (Damore et al., 2003; Hackam et al., 1999; Skokan et al., 2003; Taylor and Attia, 2000). While a higher rate of serious skiing injuries occurred among boys, we found a nearly two-fold higher percentage of serious snowboard-related injuries in girls. The latter result underlines the inconsistent findings in literature reported by Hagel who questioned the influence of gender on the injury risk in pediatric skiers and snowboarders (Hagel, 2005). The same author has indicated that pediatric snowboarders are at higher risk for severe injuries compared to young skiers that is explained by “more common aerial maneuvers in snowboarders” (Hagel, 2005). This statement may be doubted today. New styles of downhill skiing, to be covered by the term “freestyle skiing”, have seen a huge growth in popularity in recent years, particularly in the younger population of skiers. Apart from that, it has recently been reported that a potential injury problem may arise due to activities performed in terrain parks (Brooks et al., 2010). It remains to be determined in which way these new trends influence the characteristics of pediatric winter-sports-related injuries.
Our findings confirm previous observations that different patterns of injury exist in pediatric skiers and snowboarders with noticeable variation in different age groups (Hagel, 2005). Similar to other reports (Hackam et al., 1999; Skokan et al., 2003), we found that serious injuries were predominately related to the head. Current strategies to prevent pediatric head injuries have focused on the beneficial effects of helmet use in skiers and snowboarders (Macnab et al., 2002). A recent meta-analysis by Russel et al. (2010) strengthens the evidence of the original research that helmet use significantly reduces the risk of head injuries in skiers and snowboarders without any additional increase of neck injuries. The high risk of head injuries in children has already influenced legislation in some European alpine countries, including some federal states in Austria, to make the use of helmets mandatory in pediatric skiers and snowboarders below 15 years of age.
Children suffering from spinal injury that is associated with the potential risk of serious long-term sequelae represented another important subgroup of pediatric trauma patients. A review of articles associated with the worldwide epidemiology of spinal cord and traumatic brain injury between 1990 and 2004 by Ackery (2007) found an increased incidence of spinal trauma, together with head trauma, in alpine skiing and snowboarding, and explained these developments by an increased risk-taking behavior, especially in young males.
In mountain rescue, the International Commission for Mountain Emergency Medicine (ICAR-MEDCOM) has established criteria for helicopter activation that comprises the patient's condition as well as circumstances at the site of accident (Tomazin et al., 2003). In our population, the majority (89.1%) of all HEMS flights for children showed a NACA injury severity score ≥III, an indication that is consistent with the guidelines suggested by ICAR-MEDCOM. Considering the substantial rate of injuries rated as NACA III, this result may be of limited informative value because the cost absorption by public health insurance is only guaranteed if rescue missions equal NACA III or higher. Despite experience showing that HEMS-physician diagnoses are quite accurate, HEMS physicians may be prone to overestimate the patient's actual injury severity.
In western Austria, an alpine area with significant winter tourism, an excessive number of private HEMS operate, because helicopter rescue from skiing areas is very profitable and thus substantial competition between public and private HEMS systems exist.
The usage of HEMS for pediatric trauma that only partially meet triage criteria may be a common occurrence. Therefore, certain triage criteria are proposed to identify trauma patients who might benefit from helicopter transport. In mountain as well as urban environment, the GCS is suggested to be a sensitive and specific indicator (McCowan et al., 2006; Moront et al., 1996).
Limitations
This study is a retrospective review based on abstracted data. The physicians collected and documented prehospital data themselves, which may be subject of relevant reporting bias without the proof of definite diagnosis. Moreover, our sample was restricted to HEMS rescue missions conducted by the OEAMTC air-rescue service and, therefore, lacking with information on helicopter flights by privately run air-rescue services in alpine environment. Because of our limited available study period, we were not able to identify any epidemiological trends for pediatric sports-related trauma in alpine environment.
Conclusions
The knowledge about epidemiological characteristics of HEMS use for injured children may be essential for training and operational requirements of HEMS crews and providers. Prior research indicates that these factors can translate into better triage, transport care and reduced morbidity.
The incidence of head and spinal injuries indicates the need for support of initiatives to promote helmet- and spine protection wear, as well as appropriate risk behavior amongst skiers and snowboarders.
Footnotes
Acknowledgment
We are grateful for the support of OEAMTC Christophorus Air Rescue Service for providing HEMS data.
We also want to thank Christoph Eckert for his contribution during final revision.
Author Disclosure Statement
The authors have no financial relationships relevant to this article to disclose.