
Abstract
Abstract
Kayser, Bengt, Lionel Dumont, Christopher Lysakowski, Christophe Combescure, Guy Haller, Martin R. Tramèr. Reappraisal of acetazolamide for the prevention of acute mountain sickness: A systematic review and meta-analysis. High Alt. Med. Biol. 13:82–92.—Acetazolamide is used to prevent acute mountain sickness (AMS). We assessed efficacy and harm of acetazolamide for the prevention of AMS, and tested for dose-responsiveness. We systematically searched electronic databases (until April 2011) for randomized trials comparing acetazolamide with placebo for the prevention of AMS. For each dose, risk ratios were aggregated using a Mantel-Haenszel fixed effect model. Numbers needed to treat (NNT) to benefit one subject with each dose were calculated for different baseline risks. Modes of ascent were taken as proxies of baseline risks. Twenty-four trials were included; 1011 subjects received acetazolamide 250, 500, or 750 mg day−1; 854 received placebo. When climbing, median speed of ascent was 14 m/h, average AMS rate in controls was 34%, and NNT to prevent AMS with acetazolamide 250, 500, and 750 mg/day compared with placebo was 6.5, 5.9, and 5.3. When ascending by transport and subsequent climbing (speed of ascent 133 m/h) or by transport alone (491 m/h), average AMS rate in controls was 60%, and NNT with acetazolamide 250, 500, and 750 mg/day was 3.7, 3.3, and 3.0. In hypobaric chambers, median speed of ascent was 4438 m/h, average AMS rate in controls was 86%, and NNT with acetazolamide 250, 500, and 750 mg/day was 2.6, 2.3, and 2.1. The risk of paresthesia was increased with all doses. The risk of polyuria and taste disturbance was increased with 500 and 750 mg/day. The degree of efficacy of acetazolamide for the prevention of AMS is limited when the baseline risk is low, and there is some evidence of dose-responsiveness.
Introduction
Generally AMS is self-limiting, passing with time spent at altitude. However, the intensity of symptoms may become severe and it is thought that AMS may develop towards potentially lethal high altitude cerebral edema (Hackett and Roach, 2004). More and more subjects going to high altitude are using acetazolamide, a sulfonamide and carbonic anhydrase inhibitor, for the prevention of AMS. Self-medication with acetazolamide in trekkers in the Himalaya increased from 1% in 1986 to 12% in 1998 (Gaillard et al., 2004), and further to 25% in 2010 (Kilner and Mukerji, 2010). However, the optimal regimen of acetazolamide remains unknown. Also, fear of specific adverse drug reactions (e.g., paresthesia or polyuria) may prevent users from taking an adequate dose.
Ten years ago, systematic review of randomized trials suggested that only 750 mg/day was efficacious for the prevention of AMS and that for lower doses, there was a lack of evidence of efficacy (Dumont et al., 2000). At the time, that conclusion was contentious; lower doses were widely believed to be as efficacious as higher doses, with a lower risk of adverse effects (Bartsch and Schneider, 2001; Basnyat and Gertsch, 2003; Dumont et al., 2005; Hackett and Roach 2001). A review of studies published between 2000 and 2011 concluded that evidence was still insufficient to recommend acetazolamide 250 mg daily as superior to higher doses in the prevention of acute mountain sickness or resulting in fewer adverse events (Seupaul 2011).
The aim of this study was to update the previously published systematic review (Dumont et al., 2000) and to test for dose-responsiveness of acetazolamide for the prevention of AMS. We stratified analyses according to daily doses of acetazolamide and baseline risks.
Methods
Search strategy
Two reviewers (LD and CL) carried out a comprehensive literature search (last update, April 2011) in
Selection of studies
One of us (LD) reviewed the abstracts of all retrieved titles and decided whether the paper contained potentially relevant information; this was verified by a second author (CL). If the paper was deemed eligible, the full report was obtained for detailed analysis.
We included studies published in any language that were performed in subjects who were ascending to high altitude by climbing or transport. We also included studies where high altitude conditions were simulated in hypobaric chambers.
Data abstraction and assessment of methodological quality
The primary end point of interest was prevention of AMS according to the original authors' definition. We only extracted data when they were available in dichotomous form. When AMS was reported at different time points, we extracted the highest cumulative incidence, with acetazolamide and placebo. Data on adverse drug reactions were extracted when they were reported in dichotomous form.
Potentially relevant reports were read by all authors independently and assessed for quality of data reporting using a validated three item, five point scale that considers quality of randomization, degree of blinding, and reporting of withdrawals (Jadad et al., 1996). Agreement was reached through consensus. To be included, studies had at least a randomized design (i.e., score ≥1).
Statistical analysis
We analyzed dichotomous data by calculating risk ratios with 95% confidence intervals. We used a Mantel-Haenszel fixed effect model to aggregate data. Heterogeneity between studies was tested using the Cochrane and I2 statistics. We assessed publication bias using funnel plots and the Egger's test for asymmetry.
To test for dose-responsiveness, we compared aggregated risk ratios of the three tested acetazolamide regimens (250, 500, 750 mg/day). There was a pre-hoc agreement that consistently decreasing point estimates of the risk ratios with increasing doses, in combination with significant heterogeneity (p≤0.1), would be regarded as evidence of statistically significant dose-responsiveness.
To test for the relationship between baseline risk of AMS and the efficacy of prophylaxis, we grouped trials according to different modes of ascent (climbing, transport, hypobaric chamber), as there was evidence that the baseline risk was closely related to mode of ascent (Dumont et al., 2000). We computed an average control event rate (incidence of AMS in control subjects) for each stratum; the control event rate was regarded as a surrogate of the true underlying risk. Within each stratum, we then calculated for each dose of acetazolamide a number-needed-to-treat to prevent AMS compared with placebo, using the average, mode of ascent-specific, control event rate, and the aggregated risk ratio that was previously calculated for that dose.
For the analysis of adverse drug reactions, we stratified data according to daily regimens (250, 500, 750 mg/day) and compared subgroups using the Cochrane test for heterogeneity.
Data were processed and analyzed using Excel 2007 (Microsoft, Redmond, WA), Revman 5.0.24 (The Nordic Cochrane Centre, Copenhagen, Denmark), Comprehensive Meta-analysis, version 2 (Biostat, Englewood, NJ), and PSAW 18.0 (SPSS Inc, Chicago, IL).
Results
We retrieved 122 articles of which 24 randomized trials were eventually included in our analyses (Fig. 1) (Basnyat et al., 2003; Basnyat et al., 2006; Basnyat et al., 2008; Basnyat et al., 2011; Bradwell et al., 1981; Burki et al., 1992; Carlsten et al., 2004; Chow et al., 2005; Ellsworth et al., 1987; Ellsworth et al., 1991; Fischer et al., 2004; Gertsch et al., 2004; Gertsch et al., 2010; Greene et al., 1981; Hackett et al., 1976; Hillenbrand et al., 2006; Kronenberg and Cain, 1967; Larson et al., 1982; Moraga et al., 2007; Nicholson et al., 1988; Reinhart et al., 1994; Tissot van Patot et al., 2008; Utz et al., 1970; Zell and Goodman, 1988). The trials were published between 1967 and 2011. Since publication of the previous systematic review in 2000 (Dumont et al., 2000), 12 new randomized trials were published. Until 2000, none of the trials had tested acetazolamide 250 mg/day; since 2000, 5 have tested acetazolamide 250 mg/day, and 1 has tested 255 mg/day (Fig. 2). No dichotomous data on presence or absence of AMS could be extracted from three trials, although they provided valid data on adverse drug reactions (Bradwell et al., 1981; Greene et al., 1981; Reinhart et al., 1994).
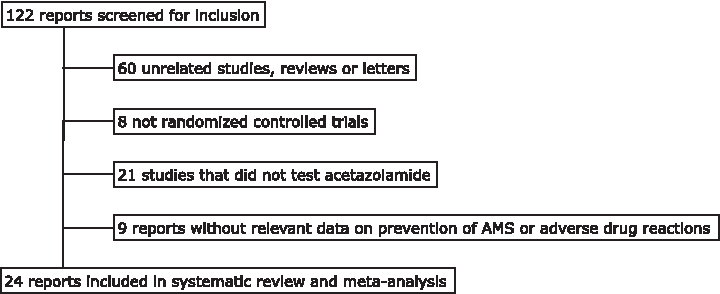
Study selection. AMS, acute mountain sickness.
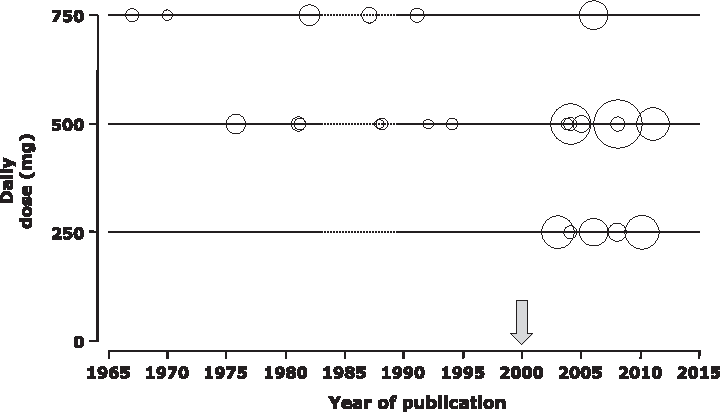
Publication of acetazolamide trials since 1965. Randomized trials testing the efficacy of different daily regimens of acetazolamide compared with placebo for the prevention of acute mountain sickness. Each bubble represents one comparison; sizes of bubbles are proportional to the number of analyzed subjects. Vertical arrow: year of publication of Dumont et al. (2000).
Data from 1865 subjects were analyzed; 1011 received acetazolamide 250, 500, or 750 mg/day, and 854 were controls (Table 1). We included into the 250 mg/day data 1 trial that tested 255 mg/day (3 times 85 mg) (Gertsch et al., 2010). None of the trials tested a dose below 250 mg/day.
ACT=Acetazolamide; AMS=Acute mountain sickness; Plac=Placebo; HC=Hypobaric chamber; LLS=Lake Louise score; ESQ=Environmental symptoms score; GHAQ=General high altitude questionnaire; R/B/W=randomization (0-2 points), blinding (0-2 points), withdrawals (0-1 point).
The median quality score was 4 (range, 2–5). Funnel plot analysis did not provide evidence of asymmetry (Fig. 3).
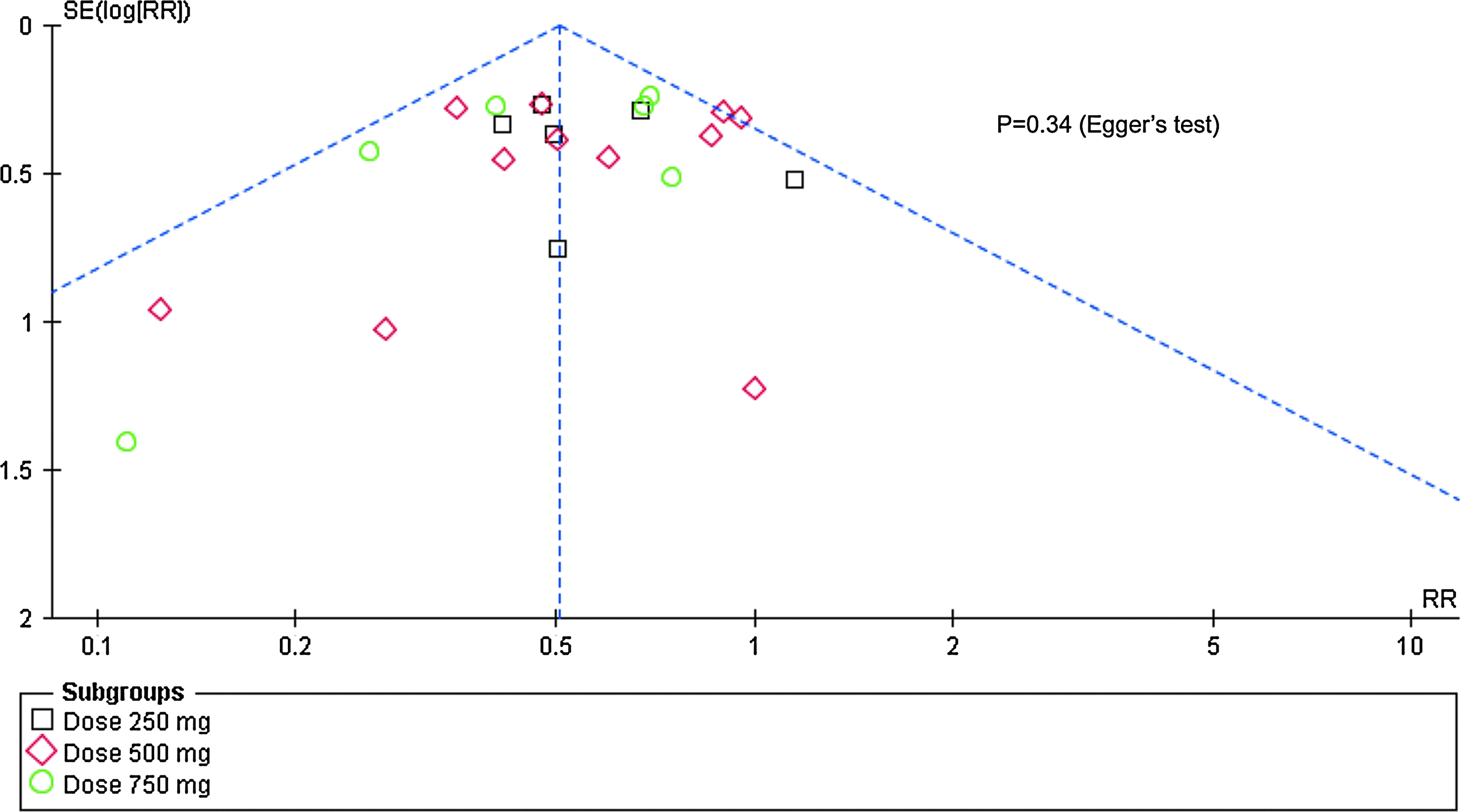
Funnel plot. Outcome was prevention of acute mountain sickness with 3 different doses of acetazolamide. No evidence of asymmetry and thus of publication bias.
Efficacy analysis independent of baseline risk
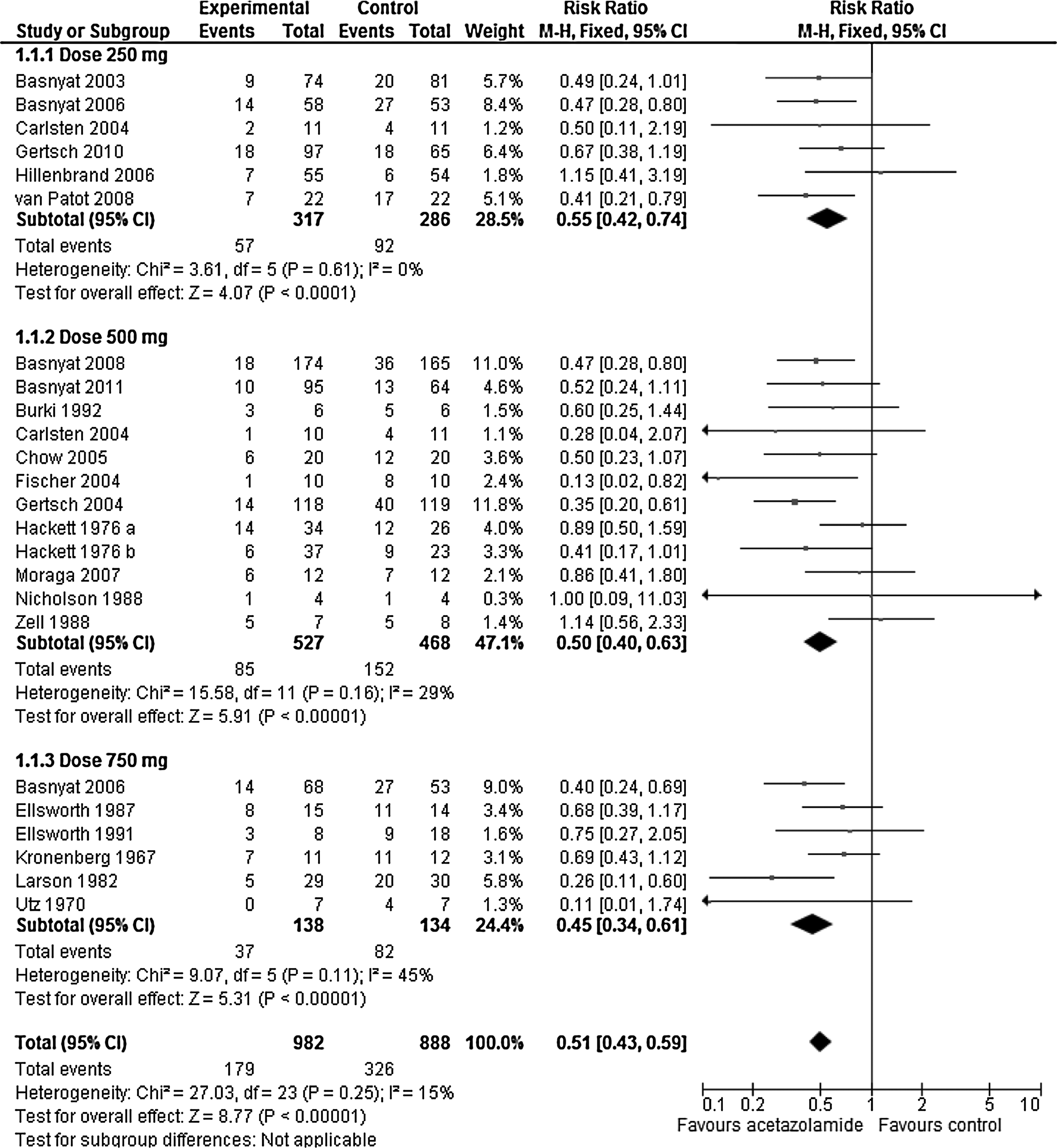
The combined risk ratios of developing AMS symptoms with acetazolamide compared with placebo and independent of the baseline risk ratio was 0.55 (95% confidence interval [CI], 0.42 to 0.74) with 250 mg/day, was 0.50 (95% CI, 0.40 to 0.63) with 500 mg/day, and was 0.45 (95% CI, 0.34 to 0.61) with 750 mg/day; p value for heterogeneity was 0.21 (Fig. 4). Point estimates of risk ratios decreased consistently with increasing doses, by 9% when increasing from 250 to 500 mg/day, and by an additional 9% when increasing from 500 to 750 mg/day.
Sensitivity analysis
The included trials reported on different subject cohorts and used a variety of recruitment methods. Two studies In particular, both testing acetazolamide 250 mg/day, differed from the others (Carlsten et al., 2004; Hillenbrand et al., 2006). In one, nonacclimatized tourists arriving by airplane at high altitude (3630 m) were offered acetazolamide in the first 2 hours upon arrival (Carlsten et al., 2004). Some tourists already had symptoms upon enrollment and this study may thus be classified as a treatment, rather than a prophylaxis, study. In the other, both high- and lowlander subjects were included, and the baseline risk of AMS was 11% only (Hillenbrand et al., 2006). We therefore tested the robustness of the results excluding these two reports from the 250 mg/day analysis. Combining data from the four remaining studies (Basnyat et al., 2003; Basnyat et al., 2006; Gertsch et al., 2010; Tissot van Patot et al., 2008), there were 48 of 251 subjects (19.1%) receiving acetazolamide 250 mg who had AMS compared with 82 of 221 (37.1%) controls; risk ratio 0.51 (95% CI, 0.38 to 0.74). This result was not significantly different from the combined analysis including all 250 mg/day data.
Mode of ascent, speed of ascent, and baseline risk
Data on mode and speed of ascent could be extracted from 15 trials (Fig. 4, Table 2) (Basnyat et al., 2006; Burki et al., 1992; Carlsten et al., 2004; Chow et al., 2005; Ellsworth et al., 1987; Ellsworth et al., 1991; Fischer et al., 2004; Hackett et al., 1976; Hillenbrand et al., 2006; Kronenberg and Cain, 1967; Larson et al., 1982; Moraga et al., 2007; Nicholson et al., 1988; Tissot van Patot et al., 2008; Zell and Goodman, 1988). One of those reported on two subgroups with two different modes and speeds of ascent (Hackett et al., 1976).
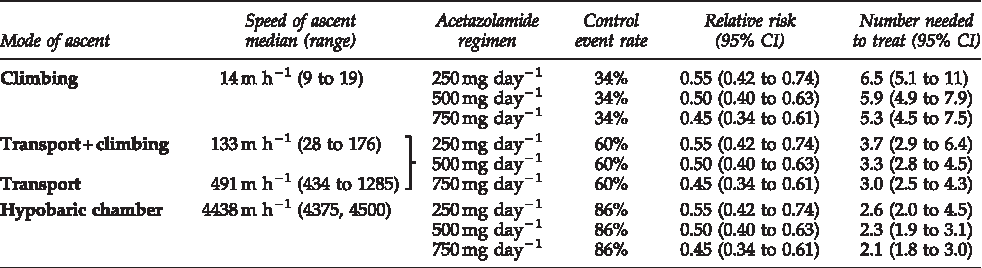
Modes and speeds of ascent and respective studies: see, Table 1. Control event rate=Average incidence of acute mountain sickness in control subjects of all trials that were using this mode of ascent. Average control event rate for “Transport+climbing” was 59%, for “Transport” was 63%; for simplicity, both were averaged to 60% Relative risks were taken from Figure 4. Numbers needed to treat with 95% confidence intervals were computed using relative risk point estimates and their 95% confidence intervals and control event rates.
In 4 trials, mode of ascent was climbing (Basnyat et al., 2006; Hackett et al., 1976; Hillenbrand et al., 2006; Nicholson et al., 1988). Median speed of ascent was 14 m/h (range, 9–19 m/h). The average control event rate was 34% (46 of 137 control subjects were reported to have AMS). The number needed to treat to prevent AMS with acetazolamide compared with placebo, using this average control event rate and the risk ratio of each dose (see Fig. 4), was 6.5 with 250 mg/day, 5.9 with 500 mg/day, and 5.3 with 750 mg/day (Table 2).
In 5 trials, mode of ascent was transport with subsequent climbing (Ellsworth et al., 1987; Ellsworth et al., 1991; Hackett et al., 1976; Larson et al., 1982; Zell and Goodman, 1988). Median speed of ascent was 133 m/h (range, 28–176 m/h). The average control event rate was 59% (55 of 93 control subjects were reported to have AMS). In a further 5 trials, subjects ascended exclusively by transport (Burki et al., 1992; Carlsten et al., 2004; Chow et al., 2005; Moraga et al., 2007; Tissot van Patot et al., 2008). Median speed of ascent was 491 m/h (range, 434–1285 m/h). The average control event rate was 63% (45 of 71 control subjects were reported to have AMS). Since average control event rates were very similar with the subgroups that ascended through transport with or without climbing, we combined these data within 1 mode of ascent. When ascending by transport, with or without climbing, the number needed to treat to prevent AMS with acetazolamide compared with placebo, using this average control event rate and the risk ratio of each dose (see Fig. 4), was 3.7 with 250 mg/day, 3.3 with 500 mg/day, and 3.0 with 750 mg/day (Table 2).
Finally, 2 trials were performed with volunteers in hypobaric chambers (Fisher, 1998; Kronenberg and Cain, 1967). Median speed of ascent was 4438 m/h. The average control event rate was 86% (19 of 22 control subjects had AMS). The number needed to treat to prevent AMS with acetazolamide compared with placebo, using this average control event rate and the risk ratio of each dose (see Fig. 4), was 2.6 with 250 mg/day, 2.3 with 500 mg/day, and 2.1 with 750 mg/day (Table 2).
Adverse drug reactions
Paresthesia, polyuria, and taste disturbance were most frequently described. The risk of paresthesia was increased compared with placebo and independent of the dose of acetazolamide (Table 3). Point estimates of risk ratios suggested that the likelihood of polyuria and taste disturbance was increased with acetazolamide 500 or 750 mg/day but not with 250 mg/day.
CI=confidence interval. Risk ratios between acetazolamide and placebo.
Discussion
Analysis of aggregate data from randomized trials provides consistent evidence that within a dose range of 250 to 750 mg/day, the efficacy of acetazolamide for the prevention of AMS depends on mode of ascent and speed of ascent. There is weak evidence of dose-responsiveness. The risk of paresthesia is increased independent of the dose, while the risk of polyuria and taste disturbance is increased with 500 and 750 mg/day only.
The optimal dose of acetazolamide for the prevention of AMS has been contentious for many years. Ten years ago, systematic review suggested that 750 mg/day was efficacious and that there was a lack of evidence of efficacy for lower doses (Dumont et al., 2000). The reasonable conclusion from that analysis at that time was that lower doses should not be recommended for prevention (Dumont et al., 2000). However, international expert panels have continued recommending doses as low as 250 mg/day for the prevention of AMS despite the lack of a convincing evidence base (Luks et al., 2010; Seupaul, 2011). Of note is that until 2000, when the initial meta-analysis was published, no trial had tested 250 mg/day. Between 2000 and 2010, 6 trials have tested 250 mg/day.
Baseline risk and efficacy of prophylaxis
It is well known that the baseline risk of AMS depends on speed and mode of ascent (Dumont et al., 2000; Gaillard et al., 2004; Hackett et al., 1976; Maggiorini et al., 1998). In the included studies, ascent rates were lowest with climbing and, accordingly, AMS rates in controls were lowest too, suggesting that with climbing, the baseline risk was minor compared with, for instance, rapid transport to altitude. Within each mode of ascent stratum, there was weak, but consistent, evidence of dose-responsiveness with acetazolamide. Risk ratios were quite similar between dosage regimens (ranging from 0.45 to 0.55), but consistently improved with increasing dose, with CIs always below unity. Numbers needed to treat allowed for estimation of the effort needed to benefit an individual, depending on both baseline risk and dose. With climbing, for instance, the baseline risk was low (only 34% of control subjects receiving placebo had AMS symptoms) and the number needed to treat to prevent 1 case of AMS was almost 7 with the lowest dose and improved to 5 with the highest. This suggests that of 7 subjects taking acetazolamide 250 mg/day and ascending to altitude through climbing, one would profit from prophylaxis (he would develop AMS symptoms had they not received prophylaxis), 4 (66%) would not develop AMS symptoms anyway, and 2 would have AMS symptoms despite prophylaxis. Increasing the dose to 750 mg/day would not significantly improve this degree of efficacy. In hypobaric chambers, however, where speed of ascent and control event rates were highest, numbers needed to treat were 2 to 3 times lower (i.e. efficacy was 2 to 3 times higher), while dose-responsiveness was still maintained, although the difference between doses was less prominent. Even though the data obtained in volunteers in hypobaric chambers provide theoretical information on drug efficacy only, they confirm the tight relationship between underlying risk and efficacy of prophylaxis. It may be inferred from our results that when the baseline risk is low, as with climbing, mono-prophylaxis with acetazolamide, independent of the dose, has only a limited degree of efficacy, as a considerable number of subjects need to receive prophylaxis for one to benefit. When ascending by transport, with or without climbing, the baseline risk is much higher though, and accordingly, prophylaxis with acetazolamide may be considered worthwhile, as recommended by the guidelines of the Wilderness Medical Society (Luks et al. 2010).
Exercise at altitude has been reported to aggravate AMS symptoms (Hackett et al., 2001). It may be inferred that climbing subjects need higher doses of acetazolamide for AMS prevention than those passively exposed to high altitude; especially rapid ascent, for instance, through transport, and subsequent exercise, may trigger AMS development. Interestingly, the risk of AMS in control subjects who were ascending by transport followed by climbing or who were ascending exclusively by transport were very similar, although speeds of ascent were faster in those who were ascending by transport only. This may suggest that in those who ascend by a combination of transport and subsequent climbing, the baseline risk of AMS is driven by the rapid transport ascent. Consequently, subjects who ascend to high altitude with transport should be considered as a high-risk population for the development of AMS, even if a part of their ascent is by climbing. This finding corroborates the findings of the early hallmark study of Hackett (Hackett et al., 1976).
In some studies, subjects were recruited at altitude, sometimes above 4000 meters (Basnyat et al., 2003; Basnyat et al., 2008; Basnyat et al., 2011; Gertsch et al., 2004; Gertsch et al., 2010). According to the authors of these studies, subjects who already presented AMS symptoms were not considered for inclusion. Consequently, these cohorts may have consisted, at least partially, in selected subjects who were less prone to get the illness since they were already acclimatized or had low susceptibility for AMS. However, when the underlying risk is low, prophylaxis has less scope to show efficacy.
Two included trials, both testing a 250 mg/day regimen, may be criticized due to their study designs (Carlsten et al., 2004; Hillenbrand et al., 2006). However, exclusion of these trials in a sensitivity analysis did not significantly change the overall result for efficacy of the 250 mg/day regimen, although the difference in risk ratio point estimates of the combined 250 mg and 500 mg data became smaller.
Our analysis provides a rational basis for decision-making for subjects who would like to prevent AMS symptoms with acetazolamide. One argument may be that the differences in numbers-needed-to-treat between doses are shallow and that therefore the lowest effective dose should be chosen. However, there is also an argument to try to tailor the optimal acetazolamide regimen according to mode (and speed) of ascent, the individual's susceptibility for AMS, expectations of the potency of prophylaxis, and the willingness to accept some adverse drug reactions. The risk of both polyuria and taste disturbance was increased with 500 and 750 mg/day but not with the lowest dose. This clearly favors the lowest dose for those who perceive polyuria and taste disturbance as unacceptable. On the other hand, the risk of paresthesia was increased to a similar extent with all doses; tingling of fingers or toes can, therefore, not further inform decision-making. As all 3 doses showed efficacy, an individual might prefer to start with the minimal effective dose that still provides a certain degree of protection but with a lesser risk of adverse effects, and push the dose up depending on clinical efficacy and adverse effects. Alternatively, a subject may want to start with a higher dose that ensures better protection and eventually decrease the dose if unacceptable adverse effects should occur. It must be stressed that regimens below 250 mg/day have not been tested so far, and, therefore, should not be recommended.
A word of caution is indicated though. Pharmacology should not replace widely accepted precautions in subjects traveling to high altitude, such as appropriate acclimatization through slow ascent. Prophylaxis of AMS with acetazolamide is not without risk. The majority of reported drug-related adverse effects concerned paresthesia, polyuria, and taste disturbance. However, other adverse effects may be observed in subjects taking acetazolamide; they are related to metabolic acidosis and electrolyte imbalance (Epstein and Grant 1977; Luks and Swenson 2008), even though these are probably only clinically relevant in cases of pre-existing metabolic acidosis or kidney disease and in individuals taking diuretics with kalieuretic effects. It is of note that some of the typical acetazolamide-related adverse effects (nausea, vomiting, drowsiness, confusion) cannot be clearly separated from the symptoms of AMS and may have obscured some of the prophylactic effect of acetazolamide on AMS. Acetazolamide has also been related to ‘sulfa allergy’-like adverse effects, which are regularly mentioned in recommendations. Anaphylactic reactions cannot be excluded, although the risk of sulfa cross-reactivity is probably low (Kelly and Hackett 2010; Lee et al., 2004). Finally, it is important to realize that even with high dose acetazolamide, or any other prophylactic option, nonacclimatized individuals who ascend too fast may still get sick.
Limitations
Our analysis has limitations. First, the choice of absence of AMS as a dichotomous endpoint may be considered problematic for a variety of reasons. For instance, AMS is a composite of several symptoms, each with different degrees of intensity. Yet any decrease in the intensity of one or more symptoms may represent a relevant benefit. Thus, pharmacological prophylaxis that alleviates AMS symptoms to some extent may be considered useful. Also, the symptoms that are considered for the diagnosis of AMS are subjective, and therefore, researchers have to trust individuals' self-reporting (Roach and Kayser, 2007). Finally, a variety of scores have been used to assess AMS (Dellasanta et al., 2007). However, increasingly standardized methods to quantify AMS with the Lake Louise Scoring System have improved the validity of outcome measurements. Furthermore, the dichotomous endpoint “absence versus presence of AMS” allows overcoming variability in endpoint reporting, avoids interpretation bias, and enables combining data from different trials, and thus increases power. Second, our data are not applicable to all subjects at high altitude. For instance, subjects who had been at high altitude shortly before were not studied in these trials. Effects of acclimatization do not disappear immediately after descent and protect against AMS upon a subsequent exposure (Kayser, 1991; Wu et al., 2009). It may be expected that these subjects would not need any prophylaxis, or would, perhaps, do with a very low dose of acetazolamide. Third, most trials were small. There is empirical evidence that trials of limited size have the tendency to overestimate the efficacy of a treatment (see, for instance, Moore et al., 1998). Consequently, the cautious conclusion would be that the degree of efficacy of prophylaxis as reported in these trials is likely to be overestimated. Finally, all trials studied fixed doses of acetazolamide, independent of gender or body mass. It has been reported that the efficacy of acetazolamide may not only depend on dose and baseline risk but also on body mass and gender (Hoag et al., 2003).
To confirm or refute the results of our meta-analysis, it would take a well-designed, large, randomized dose-finding study in nonacclimatized subjects, starting at low altitude and ascending to high altitude at various climbing speeds (Dumont et al., 2005). It is unsure whether such a trial would significantly advance knowledge, as our analyses suggest that with the tested dose-range (i.e. 250 to 750 mg/day), the upper horizontal part of the sigmoid-shaped dose-response curve may be reached. For reasons of comfort related to adverse effects, minimal effective doses of acetazolamide may be sought. Alternatively, we contend that drug combinations should be tested, as no drug when used on its own was shown to be universally efficacious for the prevention of AMS (Dumont et al., 2000; Luks et al., 2010; Luks and Swenson, 2008). Additive or even synergistic effects may be expected from combinations; doses could be reduced, and the risk of adverse effects minimized. Two small trials showed superiority of a combination of acetazolamide and dexamethasone compared with acetazolamide alone (Bernhard et al., 1998; Zell and Goodman, 1988). These results need to be confirmed. Future studies should take into account the pharmacokinetics of the drugs studied (Ritschel et al., 1998) and consider age, stature, body mass, body composition, and gender of subjects (Hoag et al., 2003). Finally, studies should use uniform ways to diagnose AMS and quantify its severity.
Conclusion
Our review suggests that for the prevention of AMS the efficacy of oral acetazolamide, 250 to 750 mg/day is limited when the baseline risk is low, and there is some evidence of dose-responsiveness. Paresthesia occurs independent of the dose. The risk of polyuria and taste disturbance is increased with 500 and 750 mg/day only.
Footnotes
Disclosure Statement
This research was supported by institutional funds. None of the authors reported disclosures; none had support from any pharmaceutical company for the submitted work, none has any relationship with any company that might have an interest in the submitted work in the previous three years, and their spouses, partners, or children have no financial relationships that may be relevant to the submitted work.