
Abstract
Abstract
MacInnis, Martin J., Jim L. Rupert, Michael S. Koehle. Evaluation of the Balance Error Scoring System (BESS) in the diagnosis of acute mountain sickness at 4380 m. High Alt. Med. Biol. 13:93–97.—Ascent to altitude is associated with a decrease in balance; however, the effect of acute mountain sickness (AMS) status on balance is variable depending on the test used and the altitude at which the test is performed. Here, we report preliminary findings on the relationship between the balance error scoring system (BESS) and AMS at the 2010 Janai Purnima festival at Gosainkunda, Nepal (4380 m). All subjects (n=37) completed a shortened BESS test (mBESS) while a subset completed the full BESS test (n=27). Pulse oximetry was used to measure heart rate and oxygen saturation, and blood pressure was measured by sphygmomanometer. Balance test scores (BESS and mBESS) and physiological measurements were compared between groups with AMS (AMS+) and without AMS (AMS-). Receiver-operator characteristic (ROC) curves were used to compare the abilities of the BESS and mBESS tests to correctly identify the AMS status of subjects. The AMS+ group had significantly higher Lake Louise scores than the AMS- group (mean=4.0 (standard deviation=1.3) vs. 0.3 (0.6), p<0.001). The AMS+ group also scored significantly higher on both the mBESS (6.6 (3.5) vs. 2.7 (1.7) errors, p=0.018) and the BESS tests (19.2 (8.8) vs. 10.4 (6.0) errors, p=0.001) compared to the AMS- group, indicating inferior balance in the AMS+ group. The area under the ROC curve was significantly greater for the BESS test (0.895) compared to the mBESS test (0.690, p=0.02), implying that the full BESS test more accurately identified a subject's AMS status. Additional studies are needed to determine if BESS could be a useful adjunct to the clinical diagnosis of AMS.
Introduction
Balance, the maintenance of the centre of gravity over the base of support, is impaired with ascent to altitude resulting in ataxia (Cymerman et al., 2001). Severe ataxia is thought to mark the progression of AMS to HACE (Hackett and Roach, 2001). A coarse clinical assessment of balance (the heel-to-toe test) is often used in the evaluation of patients at altitude (especially in the diagnosis of HACE); however, it is not sensitive for AMS (e.g. Johnson et al., 2005b; Baumgartner et al., 2002), it is difficult to quantify, and it lacks normative data to which it can be compared. A sensitive and objective assessment of balance easily administered in austere environments would be a useful addition to aid in the diagnosis of AMS as well as to assess acclimatization, monitor recovery from AMS, and detect progression to HACE.
The balance error scoring system (BESS) test is commonly used to assess changes in balance following sports-related concussions (Guskiewicz, 2001). The test is easy to administer in a laboratory or field setting, requiring only a flat surface, a foam pad, and a stopwatch. In a recent study from our laboratory, mean BESS scores were significantly greater during 8 hours of normobaric hypoxia exposure (4500 m equivalent) compared to a sham condition (unpublished data). To evaluate the relationship between BESS score and AMS under hypobaric hypoxic conditions in the field, we performed BESS testing in subjects with AMS (AMS+) and without AMS (AMS-) at Gosainkunda, LangTang, Nepal (4380 m). Our hypotheses were that AMS+ subjects would have impaired balance compared to AMS- subjects and that BESS score would correlate with severity of AMS.
Methods
Subjects
During the annual Janai Purnima Festival, more than ten thousand Nepalese pilgrims ascend on foot from low altitudes (<2000 m) to Gosainkunda (4380 m), usually completing the trip in less than 48 hours. An incidence of 68% for AMS has been reported among these pilgrims (Basnyat et al., 2000), which may be a result of the typically rapid ascent in combination with the lack of prophylactic medication.
At the 2010 festival, 37 subjects were recruited at the Himalayan Rescue Association temporary medical clinic, 17 of whom were AMS+ and 20 of whom were AMS-. Seven AMS- subjects were taking acetazolamide tablets to prevent AMS; none of the AMS+ subjects were using medication to prevent AMS. No subjects had lower leg injuries contraindicating the BESS test, and subjects rested for approximately five minutes prior to undergoing assessment. The University of British Columbia and the Nepal Health Research Council granted ethical approval for this study, and each subject provided informed consent prior to testing.
AMS diagnosis
Physicians trained in high-altitude medicine diagnosed the subjects as AMS+ or AMS- using patient history, physical examination, and the LLS questionnaire. Subjects with a LLS ≥3 (with a headache score of at least 1) were assigned to the AMS+ group; subjects with a LLS <3 were assigned to the AMS- group.
Measurement of physiological variables
Oxygen saturation (SpO2), heart rate (HR), and blood pressure (BP) were measured while subjects were seated. Oxygen saturation and HR were measured by pulse oximetry, and systolic and diastolic blood pressures (SBP and DBP) were measured via auscultation with a manual sphygmomanometer.
Balance tests
All subjects underwent the BESS test or a slightly modified version (mBESS). Briefly, the BESS test consists of three stances (double, single, and tandem-legged) performed twice each (once on a firm surface and once on a dense foam Airex pad (approximately 40×50×6.5 cm in dimension; Fitter International Inc., Calgary, Canada) for a total of six 20-second trials (see Guskiewicz (2001) for more details). The mBESS was implemented for a subset of subjects when time limitations restricted the implementation of the full test: the foam pad was not used, and each stance was only performed once on a firm surface, for a total of three 20-second trials with scores assigned in a similar manner to the full BESS test. All trials were performed barefoot. To avoid learning effects (Valovich et al., 2003; Valovich McLeod et al., 2004) each subject was tested a single time with no familiarization trial. For each stance, subjects were instructed to keep their eyes closed and their hands rested on the iliac crests of their hips. The number of errors from each of the trials was counted, and all trials were summed to determine the overall balance score. Each of the following was considered an error: opening eyes, removing hands from hips, flexing or abducting hips more than 30 degrees, exaggerated lateral flexion, or changing foot position. If a subject was unable to complete a particular trial, they received the maximum score (12) for that trial. Twenty-seven subjects completed the BESS test, and an additional 10 completed the mBESS test only (note: because the BESS test included the mBESS test, all subjects were included in the mBESS cohort). The results of the BESS and mBESS tests were analyzed separately.
Statistical analysis
Differences between AMS+ and AMS- subjects for background variables (age, ascent time, LLS), physiological variables (HR, SpO2, DBP, SBP) and balance test scores (BESS and mBESS) were assessed with independent two-tail t-tests. Pearson's correlations were calculated for pairs of continuous variables. Logistic regression was used to analyze relationships between continuous and dichotomous variables (e.g., AMS status: AMS+/AMS-). The above analyses were performed with SPSS (Somers, NY) and α was set to 0.05.
The abilities of the BESS and mBESS tests to correctly identify the AMS status of subjects were assessed using receiver operator characteristic (ROC) curves. A web-based calculator was used for creating the ROC curves (Eng, 2007). MedCalc (Mariakerke, Belgium) was used to compare ROC curves statistically (using the methods of DeLong et al., 1988) and to determine the optimal thresholds for the number of errors that would signify an AMS diagnosis. The negative and positive predictive values (NPV and PPV) of these thresholds were determined with the same program.
Results
Demographics and ascent
The AMS+ group had a significantly greater mean LLS than the AMS- group (Table 1). The mean age and mean ascent time (from ∼2000 m to 4380 m) were not significantly different between the AMS+ and AMS- groups (for those who completed the mBESS or BESS tests; Table 1). In both tests, the majority of subjects were male (84% for mBESS and 81% for BESS; Table 1).
Values are presented as mean (standard deviation).
SpO2, oxygen saturation; HR, heart rate; SBP, systolic blood pressure; DBP, diastolic blood pressure; NA, not applicable.
Physiological differences between AMS+ and AMS- groups
The mean BESS and mBESS scores were significantly greater in the AMS+ group compared to the AMS- group (Fig. 1), and the correlation between the two balance tests was large (r=0.886; p<0.001). For the mBESS test, the AMS- group had a significantly greater SpO2 compared to the AMS+ group, but the same relationship did not reach significance in subjects who completed the full BESS test (Table 1). The HR, SBP and DBP values were not significantly different between the AMS+ and AMS- groups for either balance test (Table 1).
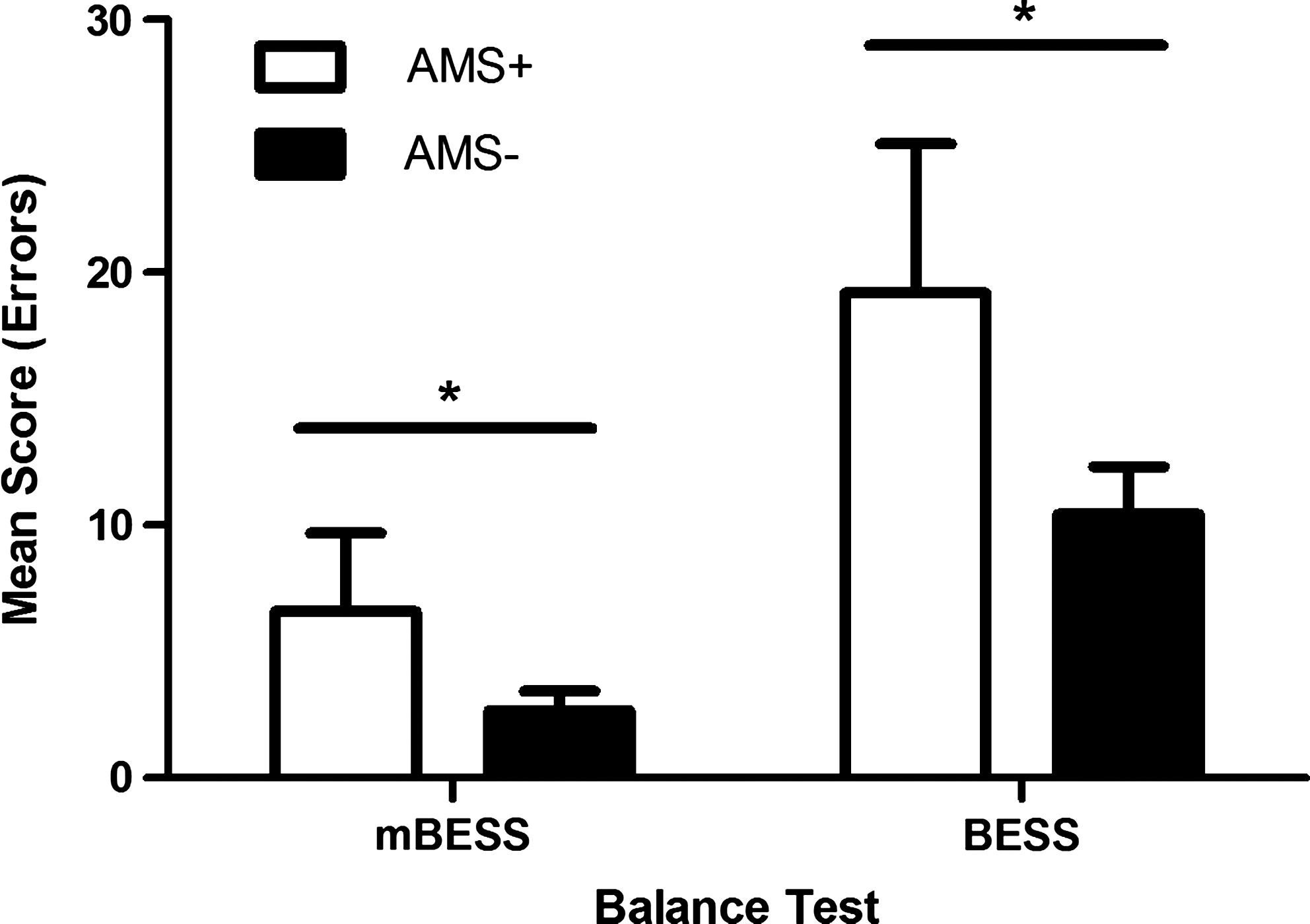
Mean error scores for subjects with (AMS+) and without (AMS-) AMS who completed the mBESS and BESS tests. For mBESS, n=37 and p=0.018 and for BESS, n=27, p=0.001. * Significantly greater mean error score in AMS+ group compared to AMS- group.
The correlations between mBESS score and LLS and the correlation between BESS score and LLS were significant (r=0.413, p=0.011; r=0.606, p<0.001, respectively); however, the correlations between each balance test and SpO2 were not significant (mBESS: r=−0.254, p=0.135; BESS: r=−0.134, p=0.504). Heart rate, SBP, and DBP were not correlated with BESS or mBESS scores (p>0.05).
The BESS and mBESS tests as diagnostic tools for AMS
The ROC curves for BESS and mBESS are shown in Fig. 2. The area under the curve, a measure of the overall performance of the test, was significantly greater for the BESS test (0.895) compared to the mBESS test (0.690; p=0.02; Fig. 2). Scores of more than 3 errors (PPV=72%, NPV=79%) for the mBESS and more than 16 errors (PPV=100%, NPV=84%) for the BESS test corresponded with the optimal false positive and false negative rates of these tests. Logistic regression was used to assess the relationship between the two balance tests and AMS status (i.e. AMS+ or AMS-). Both the mBESS and BESS tests accurately identified the AMS status of subjects (odds ratio (OR)=1.429, p=0.032 and OR=1.584, p=0.014, respectively).
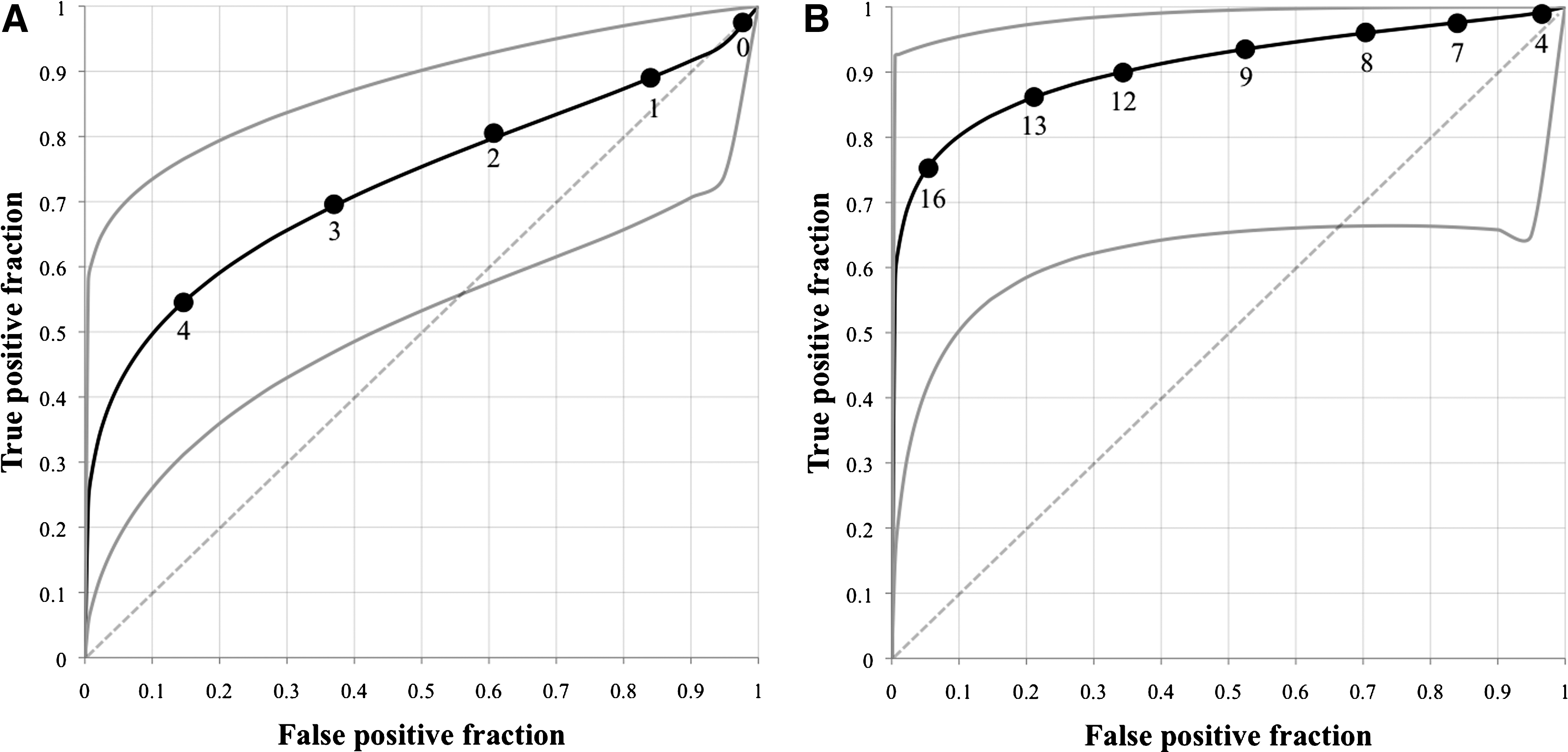
Receiver operator characteristic (ROC) curves for the mBESS (
Discussion
AMS and balance
Balance is often reported to be impaired with ascent to altitude, but differences in balance between AMS+ and AMS- subjects are not always observed (e.g., Baumgartner et al., 2002). In our study, we evaluated the relationship between BESS score and AMS status and severity. In visitors to 4380 m, the BESS test (n=27) and mBESS test (n=37, including the 27 BESS test subjects) scores correlated with AMS status and severity. Our ROC analysis showed that the BESS test was better than the mBESS test at correctly identifying the AMS status of subjects. The current LLS guidelines recommend the heel-to-toe test as an adjunct for AMS diagnosis, but as others have shown, the heel-to-toe test is not sensitive for AMS (Baumgartner et al., 2002). Here, we report preliminary data suggesting that BESS could be an adjunct tool for the assessment of AMS.
In this study, AMS+ subjects scored higher on the BESS test and the mBESS test compared to AMS- subjects, and both balance test scores were significantly correlated with LLS. The association of AMS with a reduction in ability to balance is in agreement with studies by Johnson and colleagues (2005a; 2005b). Ataxia measured with a wobble board did not increase at altitude, but AMS+ subjects made more errors than AMS- subjects at 4650 m and 5005 m (Johnson et al., 2005a). In contrast, ataxia measured with the sharpened Romberg test (which requires subjects to stand heel-to-toe with their eyes closed for up to four 60-second periods) increased with altitude (Johnson et al., 2005b). On an ascent to 5260 m, the sharpened Romberg test was able to distinguish between AMS+ and AMS- subjects at 5260m, but not at lower altitudes (including 3610 m and 4750 m, Johnson et al., 2005b). Balance under simulated laboratory conditions (5000 m hypobaric hypoxia) improved with acclimatization to altitude (i.e., after 84 days at altitude while ascending to 8201 m), suggesting that a balance test might be suitable for tracking one's acclimatization to altitude (Hoshikawa et al., 2010).
The results of the present study differ from studies by Baumgartner et al. (2002) and Cymerman et al. (2001) possibly due to differences in measuring ataxia or AMS symptoms. Stability in stance, measured by static platform posturography (Baumgartner et al., 2002) and dynamic platform balance system (Cymerman et al., 2001), was impaired with increases in altitude, but there was no difference between AMS+ and AMS- groups, implying that impaired balance was not related to AMS pathology. If our findings are correct, one reason for this discrepancy might be the method by which balance was assessed. Baumgartner et al. (2002) and Cymerman et al. (2001) assessed balance while subjects stood with their eyes open or closed for 20 s–30 s tests, which is similar to the tandem leg stance of the BESS test. In the current study, the tandem leg stance by itself (with or without a foam pad) was not sensitive enough to distinguish between AMS+ and AMS- subjects (data not shown). With respect to the BESS test, the difference in BESS score between patients with mild head injury and controls increased as stance difficulty increased (e.g. adding a foam pad; Riemann and Guskiewicz, 2000). Furthermore, both studies (Cymerman et al., 2001; Baumgartner et al., 2002) used the Environmental Symptom Questionnaire (ESQ) to assess AMS, and the sensitivities and specificities of the ESQ and LLS are not equivalent (Dellasanta et al., 2007), making comparisons with our study difficult. It should be noted that the inhalation of supplemental oxygen raised SpO2 and decreased AMS symptoms but did not improve balance (Baumgartner and Bartsch 2002), indicating that AMS symptoms resolve quicker than balance impairments with supplemental oxygen treatment.
Receiver operator characteristic (ROC) curves and logistic regression were used to assess the ability of the mBESS and BESS tests to correctly identify a subject's AMS status. The full BESS test was a more sensitive test for AMS compared to the mBESS test; therefore, even though the BESS test requires more equipment (a foam pad) and twice as much time to administer, it is a significantly better assessment of AMS status than the mBESS test. In our sample from 4380 m, a score of more than 16 errors during the BESS test was the optimal threshold for a positive AMS diagnosis.
Although several AMS- subjects were taking acetazolamide, which is known to improve ataxia in individuals with ion-channel mutations (Calandriello et al., 1997; Denier et al., 1999), the removal of subjects taking acetazolamide from our analyses did not change the results (data not shown).
Limitations and future directions
This study has several important limitations. Due to the cross-sectional design, we were unable to assess the BESS scores of individuals prior to or during ascent; thus, we cannot conclude that BESS score increases with ascent to altitude. As sea-level data are rarely available to physicians working in high-altitude clinics, and sea-level balance is not likely related to AMS susceptibility, the cross-sectional design does affect our analysis or our conclusions. We cannot rule out the possibility that the balance test scores of the AMS+ group were greater than the AMS- group prior to ascent and could remain greater after acclimatization to altitude (i.e., when AMS subsides); however, compared to normative data (Iverson et al., 2008), the AMS+ subjects scored significantly higher than adults aged 20-39 assessed at sea level, but there was no difference between the AMS- group and low-altitude residents (analysis not shown). Finally, the optimal threshold for the numbers of errors committed is likely specific to the altitude and population of this study. Larger sample sizes and studies performed at a series of altitudes are needed to refine the thresholds indicative of AMS.
Although the BESS is not an alternative for the LLS, it might have the potential to be a useful adjunct to the LLS, especially in high-altitude environments where medical equipment is limited and emergency evacuations are expensive and restricted by local terrain and weather. The LLS on its own lacks specificity in ruling out other conditions that might mimic AMS, such as dehydration, hangover, migraine, sleep deficit, fatigue, and carbon monoxide poisoning. Further research is needed to determine whether or not BESS could have a role in discriminating these conditions from AMS. The BESS may also have value in assessing acclimatization, tracking one's recovery from AMS, or assessing one's progression to HACE; however, as this is a preliminary study, we cannot recommend BESS for any of these purposes at this time. Nevertheless, BESS scores were related to the AMS status and severity of trekkers at 4380 m.
Footnotes
Disclosures
MK and JR are Natural Science and Engineering Research Council of Canada (NSERC) funded researchers. MM is a recipient of a NSERC Graduate Scholarship. MM, JR, and MK have no conflicts of interest or financial ties to disclose.
Acknowledgments
The authors are thankful for Himalayan Rescue Association's assistance in subject recruitment, AMS diagnosis, and logistics.